Subpart P - Determining Disability and Blindness
Source:
45 FR 55584, Aug. 20, 1980, unless otherwise noted.
General
§ 404.1501 Scope of subpart.
In order for you to become entitled to any benefits based upon disability or blindness or to have a period of disability established, you must be disabled or blind as defined in title II of the Social Security Act. This subpart explains how we determine whether you are disabled or blind. We discuss a period of disability in subpart D of this part. We have organized the rules in the following way.
(a) We define general terms, then discuss who makes our disability determinations and state that disability determinations made under other programs are not binding on our determinations.
(b) We explain the term disability and note some of the major factors that are considered in determining whether you are disabled in §§ 404.1505 through 404.1510.
(c) Sections 404.1512 through 404.1518 contain our rules on evidence. We explain your responsibilities for submitting evidence of your impairment, state what we consider to be acceptable sources of medical evidence, and describe what information should be included in medical reports.
(d) Our general rules on evaluating disability if you are filing a new application are stated in §§ 404.1520 through 404.1523. We describe the steps that we go through and the order in which they are considered.
(e) Our rules on medical considerations are found in §§ 404.1525 through 404.1530. We explain in these rules—
(1) The purpose of the Listing of Impairments found in appendix 1 of this subpart and how to use it;
(2) What we mean by the term medical equivalence and how we determine medical equivalence;
(3) The effect of a conclusion by your physician that you are disabled;
(4) What we mean by symptoms, signs, and laboratory findings;
(5) How we evaluate pain and other symptoms; and
(6) The effect on your benefits if you fail to follow treatment that is expected to restore your ability to work, and how we apply the rule.
(f) In §§ 404.1545 through 404.1546 we explain what we mean by the term residual functional capacity, state when an assessment of residual functional capacity is required, and who may make it.
(g) Our rules on vocational considerations are in §§ 404.1560 through 404.1569a. We explain in these rules—
(1) When we must consider vocational factors along with the medical evidence;
(2) How we use our residual functional capacity assessment to determine if you can still do your past relevant work or other work;
(3) How we consider the vocational factors of age, education, and work experience;
(4) What we mean by “work which exists in the national economy”;
(5) How we consider the exertional, nonexertional, and skill requirements of work, and when we will consider the limitations or restrictions that result from your impairment(s) and related symptoms to be exertional, nonexertional, or a combination of both; and
(6) How we use the Medical-Vocational Guidelines in appendix 2 of this subpart.
(h) Our rules on substantial gainful activity are found in §§ 404.1571 through 404.1574. These explain what we mean by substantial gainful activity and how we evaluate your work activity.
(i) In §§ 404.1577, 404.1578, and 404.1579, we explain the special rules covering disability for widows, widowers, and surviving divorced spouses for monthly benefits payable for months prior to January 1991, and in §§ 404.1581 through 404.1587 we discuss disability due to blindness.
(j) Our rules on when disability continues and stops are contained in § 404.1579 and §§ 404.1588 through 404.1598. We explain what your responsibilities are in telling us of any events that may cause a change in your disability status, when you may have a trial work period, and when we will review to see if you are still disabled. We also explain how we consider the issue of medical improvement (and the exceptions to medical improvement) in deciding whether you are still disabled.
[45 FR 55584, Aug. 20, 1980, as amended at 50 FR 50126, Dec. 6, 1985; 56 FR 57941, Nov. 14, 1991; 57 FR 30120, July 8, 1992; 68 FR 51161, Aug. 26, 2003]
§ 404.1502 Definitions for this subpart.
As used in the subpart—
(a) Acceptable medical source means a medical source who is a:
(1) Licensed physician (medical or osteopathic doctor);
(2) Licensed psychologist, which includes:
(i) A licensed or certified psychologist at the independent practice level; or
(ii) A licensed or certified school psychologist, or other licensed or certified individual with another title who performs the same function as a school psychologist in a school setting, for impairments of intellectual disability, learning disabilities, and borderline intellectual functioning only;
(3) Licensed optometrist for impairments of visual disorders, or measurement of visual acuity and visual fields only, depending on the scope of practice in the State in which the optometrist practices;
(4) Licensed podiatrist for impairments of the foot, or foot and ankle only, depending on whether the State in which the podiatrist practices permits the practice of podiatry on the foot only, or the foot and ankle;
(5) Qualified speech-language pathologist for speech or language impairments only. For this source, qualified means that the speech-language pathologist must be licensed by the State professional licensing agency, or be fully certified by the State education agency in the State in which he or she practices, or hold a Certificate of Clinical Competence in Speech-Language Pathology from the American Speech-Language-Hearing Association;
(6) Licensed audiologist for impairments of hearing loss, auditory processing disorders, and balance disorders within the licensed scope of practice only (with respect to claims filed (see § 404.614) on or after March 27, 2017);
(7) Licensed Advanced Practice Registered Nurse, or other licensed advanced practice nurse with another title, for impairments within his or her licensed scope of practice (only with respect to claims filed (see § 404.614) on or after March 27, 2017); or
(8) Licensed Physician Assistant for impairments within his or her licensed scope of practice (only with respect to claims filed (see § 404.614) on or after March 27, 2017).
(b) Commissioner means the Commissioner of Social Security or his or her authorized designee.
(c) Laboratory findings means one or more anatomical, physiological, or psychological phenomena that can be shown by the use of medically acceptable laboratory diagnostic techniques. Diagnostic techniques include chemical tests (such as blood tests), electrophysiological studies (such as electrocardiograms and electroencephalograms), medical imaging (such as X-rays), and psychological tests.
(d) Medical source means an individual who is licensed as a healthcare worker by a State and working within the scope of practice permitted under State or Federal law, or an individual who is certified by a State as a speech-language pathologist or a school psychologist and acting within the scope of practice permitted under State or Federal law.
(e) Nonmedical source means a source of evidence who is not a medical source. This includes, but is not limited to:
(1) You;
(2) Educational personnel (for example, school teachers, counselors, early intervention team members, developmental center workers, and daycare center workers);
(3) Public and private social welfare agency personnel; and
(4) Family members, caregivers, friends, neighbors, employers, and clergy.
(f) Objective medical evidence means signs, laboratory findings, or both.
(g) Signs means one or more anatomical, physiological, or psychological abnormalities that can be observed, apart from your statements (symptoms). Signs must be shown by medically acceptable clinical diagnostic techniques. Psychiatric signs are medically demonstrable phenomena that indicate specific psychological abnormalities, e.g., abnormalities of behavior, mood, thought, memory, orientation, development, or perception, and must also be shown by observable facts that can be medically described and evaluated.
(h) State agency means an agency of a State designated by that State to carry out the disability or blindness determination function.
(i) Symptoms means your own description of your physical or mental impairment.
(j) We or us means, as appropriate, either the Social Security Administration or the State agency making the disability or blindness determination.
(k) You or your means, as appropriate, the person who applies for benefits or for a period of disability, the person for whom an application is filed, or the person who is receiving benefits based on disability or blindness.
[82 FR 5864, Jan. 18, 2017; 82 FR 15132, Mar. 27, 2017]
Determinations
§ 404.1503 Who makes disability and blindness determinations.
(a) State agencies. State agencies make disability and blindness determinations for the Commissioner for most persons living in the State. State agencies make these disability and blindness determinations under regulations containing performance standards and other administrative requirements relating to the disability and blindness determination function. States have the option of turning the function over to the Federal Government if they no longer want to make disability determinations. Also, the Commissioner may take the function away from any State which has substantially failed to make disability and blindness determinations in accordance with these regulations. Subpart Q of this part contains the rules the States must follow in making disability and blindness determinations.
(b) Social Security Administration. The Social Security Administration will make disability and blindness determinations for—
(1) Any person living in a State which is not making for the Commissioner any disability and blindness determinations or which is not making those determinations for the class of claimants to which that person belongs; and
(2) Any person living outside the United States.
(c) What determinations are authorized. The Commissioner has authorized the State agencies and the Social Security Administration to make determinations about—
(1) Whether you are disabled or blind;
(2) The date your disability or blindness began; and
(3) The date your disability or blindness stopped.
(d) Review of State Agency determinations. On review of a State agency determination or redetermination of disability or blindness we may find that—
(1) You are, or are not, disabled or blind, regardless of what the State agency found;
(2) Your disability or blindness began earlier or later than the date found by the State agency; and
(3) Your disability or blindness stopped earlier or later than the date found by the State agency.
[46 FR 29204, May 29, 1981, as amended at 52 FR 33926, Sept. 9, 1987; 62 FR 38451, July 18, 1997; 65 FR 34957, June 1, 2000; 71 FR 16443, Mar. 31, 2006; 72 FR 51177, Sept. 6, 2007; 82 FR 5864, Jan. 18, 2017]
§ 404.1503a Program integrity.
We will not use in our program any individual or entity, except to provide existing medical evidence, who is currently excluded, suspended, or otherwise barred from participation in the Medicare or Medicaid programs, or any other Federal or Federally-assisted program; whose license to provide health care services is currently revoked or suspended by any State licensing authority pursuant to adequate due process procedures for reasons bearing on professional competence, professional conduct, or financial integrity; or who, until a final determination is made, has surrendered such a license while formal disciplinary proceedings involving professional conduct are pending. By individual or entity we mean a medical or psychological consultant, consultative examination provider, or diagnostic test facility. Also see §§ 404.1519 and 404.1519g(b).
[56 FR 36954, Aug. 1, 1991]
§ 404.1503b Evidence from excluded medical sources of evidence.
(a) General. We will not consider evidence from the following medical sources excluded under section 223(d)(5)(C)(i) of the Social Security Act (Act), as amended, unless we find good cause under paragraph (b) of this section:
(1) Any medical source that has been convicted of a felony under section 208 or under section 1632 of the Act;
(2) Any medical source that has been excluded from participation in any Federal health care program under section 1128 of the Act; or
(3) Any medical source that has received a final decision imposing a civil monetary penalty or assessment, or both, for submitting false evidence under section 1129 of the Act.
(b) Good cause. We may find good cause to consider evidence from an excluded medical source of evidence under section 223(d)(5)(C)(i) of the Act, as amended, if:
(1) The evidence from the medical source consists of evidence of treatment that occurred before the date the source was convicted of a felony under section 208 or under section 1632 of the Act;
(2) The evidence from the medical source consists of evidence of treatment that occurred during a period in which the source was not excluded from participation in any Federal health care program under section 1128 of the Act;
(3) The evidence from the medical source consists of evidence of treatment that occurred before the date the source received a final decision imposing a civil monetary penalty or assessment, or both, for submitting false evidence under section 1129 of the Act;
(4) The sole basis for the medical source's exclusion under section 223(d)(5)(C)(i) of the Act, as amended, is that the source cannot participate in any Federal health care program under section 1128 of the Act, but the Office of Inspector General of the Department of Health and Human Services granted a waiver of the section 1128 exclusion; or
(5) The evidence is a laboratory finding about a physical impairment and there is no indication that the finding is unreliable.
(c) Reporting requirements for excluded medical sources of evidence. Excluded medical sources of evidence (as described in paragraph (a) of this section) must inform us in writing that they are excluded under section 223(d)(5)(C)(i) of the Act, as amended, each time they submit evidence related to a claim for initial or continuing benefits under titles II or XVI of the Act. This reporting requirement applies to evidence that excluded medical sources of evidence submit to us either directly or through a representative, claimant, or other individual or entity.
(1) Excluded medical sources of evidence must provide a written statement, which contains the following information:
(i) A heading stating: “WRITTEN STATEMENT REGARDING SECTION 223(d)(5)(C) OF THE SOCIAL SECURITY ACT—DO NOT REMOVE”
(ii) The name and title of the medical source;
(iii) The applicable excluding event(s) stated in paragraph (a)(1)-(a)(3) of this section;
(iv) The date of the medical source's felony conviction under sections 208 or 1632 of the Act, if applicable;
(v) The date of the imposition of a civil monetary penalty or assessment, or both, for the submission of false evidence, under section 1129 of the Act, if applicable; and
(vi) The basis, effective date, anticipated length of the exclusion, and whether the Office of the Inspector General of the Department of Health and Human Services waived the exclusion, if the excluding event was the medical source's exclusion from participation in any Federal health care program under section 1128 of the Act.
(2) The written statement provided by an excluded medical source of evidence may not be removed by any individual or entity prior to submitting evidence to us.
(3) We may request that the excluded medical source of evidence provide us with additional information or clarify any information submitted that bears on the medical source's exclusion(s) under section 223(d)(5)(C)(i) of the Act, as amended.
[81 FR 65540, Sept. 22, 2016]
§ 404.1504 Decisions by other governmental agencies and nongovernmental entities.
Other governmental agencies and nongovernmental entities—such as the Department of Veterans Affairs, the Department of Defense, the Department of Labor, the Office of Personnel Management, State agencies, and private insurers— make disability, blindness, employability, Medicaid, workers' compensation, and other benefits decisions for their own programs using their own rules. Because a decision by any other governmental agency or a nongovernmental entity about whether you are disabled, blind, employable, or entitled to any benefits is based on its rules, it is not binding on us and is not our decision about whether you are disabled or blind under our rules. Therefore, in claims filed (see § 404.614) on or after March 27, 2017, we will not provide any analysis in our determination or decision about a decision made by any other governmental agency or a nongovernmental entity about whether you are disabled, blind, employable, or entitled to any benefits. However, we will consider all of the supporting evidence underlying the other governmental agency or nongovernmental entity's decision that we receive as evidence in your claim in accordance with § 404.1513(a)(1) through (4).
[82 FR 5864, Jan. 18, 2017]
Definition of Disability
§ 404.1505 Basic definition of disability.
(a) The law defines disability as the inability to do any substantial gainful activity by reason of any medically determinable physical or mental impairment which can be expected to result in death or which has lasted or can be expected to last for a continuous period of not less than 12 months. To meet this definition, you must have a severe impairment(s) that makes you unable to do your past relevant work (see § 404.1560(b)) or any other substantial gainful work that exists in the national economy. If your severe impairment(s) does not meet or medically equal a listing in appendix 1, we will assess your residual functional capacity as provided in §§ 404.1520(e) and 404.1545. (See §§ 404.1520(g)(2) and 404.1562 for an exception to this rule.) We will use this residual functional capacity assessment to determine if you can do your past relevant work. If we find that you cannot do your past relevant work, we will use the same residual functional capacity assessment and your vocational factors of age, education, and work experience to determine if you can do other work. (See § 404.1520(h) for an exception to this rule.) We will use this definition of disability if you are applying for a period of disability, or disability insurance benefits as a disabled worker, or child's insurance benefits based on disability before age 22 or, with respect to disability benefits payable for months after December 1990, as a widow, widower, or surviving divorced spouse.
(b) There are different rules for determining disability for individuals who are statutorily blind. We discuss these in §§ 404.1581 through 404.1587. There are also different rules for determining disability for widows, widowers, and surviving divorced spouses for monthly benefits for months prior to January 1991. We discuss these rules in §§ 404.1577, 404.1578, and 404.1579.
[45 FR 55584, Aug. 20, 1980, as amended at 51 FR 10616, Mar. 28, 1986; 57 FR 30120, July 8, 1992; 68 FR 51161, Aug. 26, 2003; 77 FR 43494, July 25, 2012]
§ 404.1506 When we will not consider your impairment.
(a) Permanent exclusion of felony-related impairment. In determining whether you are under a disability, we will not consider any physical or mental impairment, or any increase in severity (aggravation) of a preexisting impairment, which arises in connection with your commission of a felony after October 19, 1980, if you are subsequently convicted of this crime. Your subsequent conviction will invalidate any prior determination establishing disability if that determination was based upon any impairment, or aggravation, which we must exclude under this rule.
(b) Limited use of impairment arising in prison. In determining whether you are under a disability for purposes of benefit payments, we will not consider any physical or mental impairment, or any increase in severity (aggravation) of a preexisting impairment, which arises in connection with your confinement in a jail, prison, or other penal institution or correctional facility for conviction of a felony committed after October 19, 1980. The exclusion of the impairment, or aggravation, applies in determining disability for benefits payable for any month during which you are confined. This rule does not preclude the establishment of a period of disability based upon the impairment or aggravation. You may become entitled to benefits upon release from prison provided that you apply and are under a disability at the time.
(c) Felonious offenses. We will consider an offense a felony if—
(1) It is a felony under applicable law; or
(2) In a jurisdiction which does not classify any crime as a felony, it is an offense punishable by death or imprisonment for a term exceeding one year.
(d) Confinement. In general, a jail, prison, or other penal institution or correctional facility is a facility which is under the control and jurisdiction of the agency in charge of the penal system or in which convicted criminals can be incarcerated. Confinement in such a facility continues as long as you are under a sentence of confinement and have not been released due to parole or pardon. You are considered confined even though you are temporarily or intermittently outside of the facility (e.g., on work release, attending school, or hospitalized).
[48 FR 5714, Feb. 8, 1983]
§ 404.1508 [Reserved]
§ 404.1509 How long the impairment must last.
Unless your impairment is expected to result in death, it must have lasted or must be expected to last for a continuous period of at least 12 months. We call this the duration requirement.
§ 404.1510 Meaning of substantial gainful activity.
Substantial gainful activity means work that—
(a) Involves doing significant and productive physical or mental duties; and
(b) Is done (or intended) for pay or profit.
(See § 404.1572 for further details about what we mean by substantial gainful activity.)
§ 404.1511 Definition of a disabling impairment.
(a) Disabled workers, persons disabled since childhood and, for months after December 1990, disabled widows, widowers, and surviving divorced spouses. If you are entitled to disability cash benefits as a disabled worker, or to child's insurance benefits, or, for monthly benefits payable after December 1990, to widow's, widower's, or surviving divorced spouse's monthly benefits, a disabling impairment is an impairment (or combination of impairments) which, of itself, is so severe that it meets or equals a set of criteria in the Listing of Impairments in appendix 1 of this subpart or which, when considered with your age, education, and work experience, would result in a finding that you are disabled under § 404.1594. In determining whether you have a disabling impairment, earnings are not considered.
(b) Disabled widows, widowers, and surviving divorced spouses, for monthly benefits for months prior to January 1991. If you have been entitled to disability benefits as a disabled widow, widower, or surviving divorced spouse and we must decide whether you had a disabling impairment for any time prior to January 1991, a disabling impairment is an impairment (or combination of impairments) which, of itself, was so severe that it met or equaled a set of criteria in the Listing of Impairments in appendix 1 of this subpart, or results in a finding that you were disabled under § 404.1579. In determining whether you had a disabling impairment, earnings are not considered.
[57 FR 30120, July 8, 1992]
Evidence
§ 404.1512 Responsibility for evidence.
(a) Your responsibility —
(1) General. In general, you have to prove to us that you are blind or disabled. You must inform us about or submit all evidence known to you that relates to whether or not you are blind or disabled (see § 404.1513). This duty is ongoing and requires you to disclose any additional related evidence about which you become aware. This duty applies at each level of the administrative review process, including the Appeals Council level if the evidence relates to the period on or before the date of the administrative law judge hearing decision. We will consider only impairment(s) you say you have or about which we receive evidence. When you submit evidence received from another source, you must submit that evidence in its entirety, unless you previously submitted the same evidence to us or we instruct you otherwise. If we ask you, you must inform us about:
(i) Your medical source(s);
(ii) Your age;
(iii) Your education and training;
(iv) Your work experience;
(v) Your daily activities both before and after the date you say that you became disabled;
(vi) Your efforts to work; and
(vii) Any other factors showing how your impairment(s) affects your ability to work. In §§ 404.1560 through 404.1569, we discuss in more detail the evidence we need when we consider vocational factors.
(2) Completeness. The evidence in your case record must be complete and detailed enough to allow us to make a determination or decision about whether you are disabled or blind. It must allow us to determine—
(i) The nature and severity of your impairment(s) for any period in question;
(ii) Whether the duration requirement described in § 404.1509 is met; and
(iii) Your residual functional capacity to do work-related physical and mental activities, when the evaluation steps described in § 404.1520(e) or (f)(1) apply.
(b) Our responsibility —
(1) Development. Before we make a determination that you are not disabled, we will develop your complete medical history for at least the 12 months preceding the month in which you file your application unless there is a reason to believe that development of an earlier period is necessary or unless you say that your disability began less than 12 months before you filed your application. We will make every reasonable effort to help you get medical evidence from your own medical sources and entities that maintain your medical sources' evidence when you give us permission to request the reports.
(i) Every reasonable effort means that we will make an initial request for evidence from your medical source or entity that maintains your medical source's evidence, and, at any time between 10 and 20 calendar days after the initial request, if the evidence has not been received, we will make one follow-up request to obtain the medical evidence necessary to make a determination. The medical source or entity that maintains your medical source's evidence will have a minimum of 10 calendar days from the date of our follow-up request to reply, unless our experience with that source indicates that a longer period is advisable in a particular case.
(ii) Complete medical history means the records of your medical source(s) covering at least the 12 months preceding the month in which you file your application. If you say that your disability began less than 12 months before you filed your application, we will develop your complete medical history beginning with the month you say your disability began unless we have reason to believe your disability began earlier. If applicable, we will develop your complete medical history for the 12-month period prior to the month you were last insured for disability insurance benefits (see § 404.130), the month ending the 7-year period you may have to establish your disability and you are applying for widow's or widower's benefits based on disability (see § 404.335(c)(1)), or the month you attain age 22 and you are applying for child's benefits based on disability (see § 404.350).
(2) Obtaining a consultative examination. We may ask you to attend one or more consultative examinations at our expense. See §§ 404.1517 through 404.1519t for the rules governing the consultative examination process. Generally, we will not request a consultative examination until we have made every reasonable effort to obtain evidence from your own medical sources. We may order a consultative examination while awaiting receipt of medical source evidence in some instances, such as when we know a source is not productive, is uncooperative, or is unable to provide certain tests or procedures. We will not evaluate this evidence until we have made every reasonable effort to obtain evidence from your medical sources.
(3) Other work. In order to determine under § 404.1520(g) that you are able to adjust to other work, we must provide evidence about the existence of work in the national economy that you can do (see §§ 404.1560 through 404.1569a), given your residual functional capacity (which we have already assessed, as described in § 404.1520(e)), age, education, and work experience.
[82 FR 5864, Jan. 18, 2017]
§ 404.1513 Categories of evidence.
(a) What we mean by evidence. Subject to the provisions of paragraph (b), evidence is anything you or anyone else submits to us or that we obtain that relates to your claim. We consider evidence under §§ 404.1520b, 404.1520c (or under § 404.1527 for claims filed (see § 404.614) before March 27, 2017). We evaluate evidence we receive according to the rules pertaining to the relevant category of evidence. The categories of evidence are:
(1) Objective medical evidence. Objective medical evidence is medical signs, laboratory findings, or both, as defined in § 404.1502(f).
(2) Medical opinion. A medical opinion is a statement from a medical source about what you can still do despite your impairment(s) and whether you have one or more impairment-related limitations or restrictions in the following abilities: (For claims filed (see § 404.614) before March 27, 2017, see § 404.1527(a) for the definition of medical opinion.)
(i) Your ability to perform physical demands of work activities, such as sitting, standing, walking, lifting, carrying, pushing, pulling, or other physical functions (including manipulative or postural functions, such as reaching, handling, stooping, or crouching);
(ii) Your ability to perform mental demands of work activities, such as understanding; remembering; maintaining concentration, persistence, or pace; carrying out instructions; or responding appropriately to supervision, co-workers, or work pressures in a work setting;
(iii) Your ability to perform other demands of work, such as seeing, hearing, or using other senses; and
(iv) Your ability to adapt to environmental conditions, such as temperature extremes or fumes.
(3) Other medical evidence. Other medical evidence is evidence from a medical source that is not objective medical evidence or a medical opinion, including judgments about the nature and severity of your impairments, your medical history, clinical findings, diagnosis, treatment prescribed with response, or prognosis. (For claims filed (see § 404.614) before March 27, 2017, other medical evidence does not include a diagnosis, prognosis, or a statement that reflects a judgment(s) about the nature and severity of your impairment(s)).
(4) Evidence from nonmedical sources. Evidence from nonmedical sources is any information or statement(s) from a nonmedical source (including you) about any issue in your claim. We may receive evidence from nonmedical sources either directly from the nonmedical source or indirectly, such as from forms we receive and our administrative records.
(5) Prior administrative medical finding. A prior administrative medical finding is a finding, other than the ultimate determination about whether you are disabled, about a medical issue made by our Federal and State agency medical and psychological consultants at a prior level of review (see § 404.900) in your current claim based on their review of the evidence in your case record, such as:
(i) The existence and severity of your impairment(s);
(ii) The existence and severity of your symptoms;
(iii) Statements about whether your impairment(s) meets or medically equals any listing in the Listing of Impairments in Part 404, Subpart P, Appendix 1;
(iv) Your residual functional capacity;
(v) Whether your impairment(s) meets the duration requirement; and
(vi) How failure to follow prescribed treatment (see § 404.1530) and drug addiction and alcoholism (see § 404.1535) relate to your claim.
(b) Exceptions for privileged communications.
(1) The privileged communications listed in paragraphs (b)(1)(i) and (b)(1)(ii) of this section are not evidence, and we will neither consider nor provide any analysis about them in your determination or decision. This exception for privileged communications applies equally whether your representative is an attorney or a non-attorney.
(i) Oral or written communications between you and your representative that are subject to the attorney-client privilege, unless you voluntarily disclose the communication to us.
(ii) Your representative's analysis of your claim, unless he or she voluntarily discloses it to us. This analysis means information that is subject to the attorney work product doctrine, but it does not include medical evidence, medical opinions, or any other factual matter that we may consider in determining whether or not you are entitled to benefits (see paragraph (b)(2) of this section).
(2) The attorney-client privilege generally protects confidential communications between an attorney and his or her client that are related to providing or obtaining legal advice. The attorney work product doctrine generally protects an attorney's analyses, theories, mental impressions, and notes. In the context of your disability claim, neither the attorney-client privilege nor the attorney work product doctrine allow you to withhold factual information, medical opinions, or other medical evidence that we may consider in determining whether or not you are entitled to benefits. For example, if you tell your representative about the medical sources you have seen, your representative cannot refuse to disclose the identity of those medical sources to us based on the attorney-client privilege. As another example, if your representative asks a medical source to complete an opinion form related to your impairment(s), symptoms, or limitations, your representative cannot withhold the completed opinion form from us based on the attorney work product doctrine. The attorney work product doctrine would not protect the source's opinions on the completed form, regardless of whether or not your representative used the form in his or her analysis of your claim or made handwritten notes on the face of the report.
[82 FR 5865, Jan. 18, 2017; 82 FR 15132, Mar. 27, 2017]
§ 404.1513a Evidence from our Federal or State agency medical or psychological consultants.
The following rules apply to our Federal or State agency medical or psychological consultants that we consult in connection with administrative law judge hearings and Appeals Council reviews:
(a) In claims adjudicated by the State agency, a State agency medical or psychological consultant may make the determination of disability together with a State agency disability examiner or provide medical evidence to a State agency disability examiner when the disability examiner makes the initial or reconsideration determination alone (see § 404.1615(c)). The following rules apply:
(1) When a State agency medical or psychological consultant makes the determination together with a State agency disability examiner at the initial or reconsideration level of the administrative review process as provided in § 404.1615(c)(1), he or she will consider the evidence in your case record and make administrative findings about the medical issues, including, but not limited to, the existence and severity of your impairment(s), the existence and severity of your symptoms, whether your impairment(s) meets or medically equals the requirements for any impairment listed in appendix 1 to this subpart, and your residual functional capacity. These administrative medical findings are based on the evidence in your case but are not in themselves evidence at the level of the administrative review process at which they are made. See § 404.1513(a)(5).
(2) When a State agency disability examiner makes the initial determination alone as provided in § 404.1615(c)(3), he or she may obtain medical evidence from a State agency medical or psychological consultant about one or more of the medical issues listed in paragraph (a)(1) of this section. In these cases, the State agency disability examiner will consider the medical evidence of the State agency medical or psychological consultant under §§ 404.1520b, 404.1520c, and 404.1527.
(3) When a State agency disability examiner makes a reconsideration determination alone as provided in § 404.1615(c)(3), he or she will consider prior administrative medical findings made by a State agency medical or psychological consultant at the initial level of the administrative review process, and any medical evidence provided by such consultants at the initial and reconsideration levels, about one or more of the medical issues listed in paragraph (a)(1)(i) of this section under §§ 404.1520b, 404.1520c, and 404.1527.
(b) Administrative law judges are responsible for reviewing the evidence and making administrative findings of fact and conclusions of law. They will consider prior administrative medical findings and medical evidence from our Federal or State agency medical or psychological consultants as follows:
(1) Administrative law judges are not required to adopt any prior administrative medical findings, but they must consider this evidence according to §§ 404.1520b, 404.1520c, and 404.1527, as appropriate, because our Federal or State agency medical or psychological consultants are highly qualified and experts in Social Security disability evaluation.
(2) Administrative law judges may also ask for medical evidence from expert medical sources. Administrative law judges will consider this evidence under §§ 404.1520b, 404.1520c, and 404.1527, as appropriate.
(c) When the Appeals Council makes a decision, it will consider prior administrative medical findings according to the same rules for considering prior administrative medical findings as administrative law judges follow under paragraph (b) of this section.
[82 FR 5866, Jan 18, 2017]
§ 404.1514 When we will purchase existing evidence.
We need specific medical evidence to determine whether you are disabled or blind. You are responsible for providing that evidence. However, we will pay physicians not employed by the Federal government and other non-Federal providers of medical services for the reasonable cost of providing us with existing medical evidence that we need and ask for after November 30, 1980.
[46 FR 45757, Sept. 15, 1981]
§ 404.1515 Where and how to submit evidence.
You may give us evidence about your impairment at any of our offices or at the office of any State agency authorized to make disability determinations. You may also give evidence to one of our employees authorized to accept evidence at another place. For more information about this, see subpart H of this part.
§ 404.1516 If you fail to submit medical and other evidence.
If you do not give us the medical and other evidence that we need and request, we will have to make a decision based on information available in your case. We will not excuse you from giving us evidence because you have religious or personal reasons against medical examinations, tests, or treatment.
§ 404.1517 Consultative examination at our expense.
If your medical sources cannot or will not give us sufficient medical evidence about your impairment for us to determine whether you are disabled or blind, we may ask you to have one or more physical or mental examinations or tests. We will pay for these examinations. However, we will not pay for any medical examination arranged by you or your representative without our advance approval. If we arrange for the examination or test, we will give you reasonable notice of the date, time, and place the examination or test will be given, and the name of the person or facility who will do it. We will also give the examiner any necessary background information about your condition.
[56 FR 36956, Aug. 1, 1991]
§ 404.1518 If you do not appear at a consultative examination.
(a) General. If you are applying for benefits and do not have a good reason for failing or refusing to take part in a consultative examination or test which we arrange for you to get information we need to determine your disability or blindness, we may find that you are not disabled or blind. If you are already receiving benefits and do not have a good reason for failing or refusing to take part in a consultative examination or test which we arranged for you, we may determine that your disability or blindness has stopped because of your failure or refusal. Therefore, if you have any reason why you cannot go for the scheduled appointment, you should tell us about this as soon as possible before the examination date. If you have a good reason, we will schedule another examination. We will consider your physical, mental, educational, and linguistic limitations (including any lack of facility with the English language) when determining if you have a good reason for failing to attend a consultative examination.
(b) Examples of good reasons for failure to appear. Some examples of what we consider good reasons for not going to a scheduled examination include—
(1) Illness on the date of the scheduled examination or test;
(2) Not receiving timely notice of the scheduled examination or test, or receiving no notice at all;
(3) Being furnished incorrect or incomplete information, or being given incorrect information about the physician involved or the time or place of the examination or test, or;
(4) Having had death or serious illness occur in your immediate family.
(c) Objections by your medical source(s). If any of your medical sources tell you that you should not take the examination or test, you should tell us at once. In many cases, we may be able to get the information we need in another way. Your medical source(s) may agree to another type of examination for the same purpose.
[45 FR 55584, Aug. 20, 1980, as amended at 59 FR 1635, Jan. 12, 1994; 82 FR 5866, Jan. 18, 2017]
Standards To Be Used in Determining When a Consultative Examination Will Be Obtained in Connection With Disability Determinations
§ 404.1519 The consultative examination.
A consultative examination is a physical or mental examination or test purchased for you at our request and expense from a treating source or another medical source, including a pediatrician when appropriate. The decision to purchase a consultative examination will be made on an individual case basis in accordance with the provisions of §§ 404.1519a through 404.1519f. Selection of the source for the examination will be consistent with the provisions of § 404.1503a and §§ 404.1519g through 404.1519j. The rules and procedures for requesting consultative examinations set forth in §§ 404.1519a and 404.1519b are applicable at the reconsideration and hearing levels of review, as well as the initial level of determination.
[56 FR 36956, Aug. 1, 1991, as amended at 65 FR 11875, Mar. 7, 2000]
§ 404.1519a When we will purchase a consultative examination and how we will use it.
(a) General. If we cannot get the information we need from your medical sources, we may decide to purchase a consultative examination. See § 404.1512 for the procedures we will follow to obtain evidence from your medical sources and § 404.1520b for how we consider evidence. Before purchasing a consultative examination, we will consider not only existing medical reports, but also the disability interview form containing your allegations as well as other pertinent evidence in your file.
(b) Situations that may require a consultative examination. We may purchase a consultative examination to try to resolve an inconsistency in the evidence, or when the evidence as a whole is insufficient to allow us to make a determination or decision on your claim. Some examples of when we might purchase a consultative examination to secure needed medical evidence, such as clinical findings, laboratory tests, a diagnosis, or prognosis, include but are not limited to:
(1) The additional evidence needed is not contained in the records of your medical sources;
(2) The evidence that may have been available from your treating or other medical sources cannot be obtained for reasons beyond your control, such as death or noncooperation of a medical source;
(3) Highly technical or specialized medical evidence that we need is not available from your treating or other medical sources; or
(4) There is an indication of a change in your condition that is likely to affect your ability to work, but the current severity of your impairment is not established.
[56 FR 36956, Aug. 1, 1991, as amended at 77 FR 10655, Feb. 23, 2012]
§ 404.1519b When we will not purchase a consultative examination.
We will not purchase a consultative examination in situations including, but not limited to, the following situations:
(a) In period of disability and disability insurance benefit claims, when you do not meet the insured status requirement in the calendar quarter you allege you became disabled or later and there is no possibility of establishing an earlier onset;
(b) In claims for widow's or widower's benefits based on disability, when your alleged month of disability is after the end of the 7-year period specified in § 404.335(c)(1) and there is no possibility of establishing an earlier onset date, or when the 7-year period expired in the past and there is no possibility of establishing an onset date prior to the date the 7-year period expired;
(c) In disability insurance benefit claims, when your insured status expired in the past and there is no possibility of establishing an onset date prior to the date your insured status expired;
(d) When any issues about your actual performance of substantial gainful activity or gainful activity have not been resolved;
(e) In claims for child's benefits based on disability, when it is determined that your alleged disability did not begin before the month you attained age 22, and there is no possibility of establishing an onset date earlier than the month in which you attained age 22;
(f) In claims for child's benefits based on disability that are filed concurrently with the insured individual's claim and entitlement cannot be established for the insured individual;
(g) In claims for child's benefits based on disability where entitlement is precluded based on other nondisability factors.
[56 FR 36956, Aug. 1, 1991]
Standards for the Type of Referral and for Report Content
§ 404.1519f Type of purchased examinations.
We will purchase only the specific examinations and tests we need to make a determination in your claim. For example, we will not authorize a comprehensive medical examination when the only evidence we need is a special test, such as an X-ray, blood studies, or an electrocardiogram.
[56 FR 36956, Aug. 1, 1991]
§ 404.1519g Who we will select to perform a consultative examination.
(a) We will purchase a consultative examination only from a qualified medical source. The medical source may be your own medical source or another medical source. If you are a child, the medical source we choose may be a pediatrician.
(b) By “qualified,” we mean that the medical source must be currently licensed in the State and have the training and experience to perform the type of examination or test we will request; the medical source must not be barred from participation in our programs under the provisions of § 404.1503a. The medical source must also have the equipment required to provide an adequate assessment and record of the existence and level of severity of your alleged impairments.
(c) The medical source we choose may use support staff to help perform the consultative examination. Any such support staff (e.g., X-ray technician, nurse) must meet appropriate licensing or certification requirements of the State. See § 404.1503a.
[56 FR 36957, Aug. 1, 1991, as amended at 65 FR 11876, Mar. 7, 2000; 82 FR 5866, Jan. 18, 2017]
§ 404.1519h Your medical source.
When, in our judgment, your medical source is qualified, equipped, and willing to perform the additional examination or test(s) for the fee schedule payment, and generally furnishes complete and timely reports, your medical source will be the preferred source for the purchased examination or test(s).
[82 FR 5866, Jan. 18, 2017]
§ 404.1519i Other sources for consultative examinations.
We will use a different medical source than your medical source for a purchased examination or test in situations including, but not limited to, the following:
(a) Your medical source prefers not to perform such an examination or does not have the equipment to provide the specific data needed;
(b) There are conflicts or inconsistencies in your file that cannot be resolved by going back to your medical source;
(c) You prefer a source other than your medical source and have a good reason for your preference;
(d) We know from prior experience that your medical source may not be a productive source, such as when he or she has consistently failed to provide complete or timely reports; or
(e) Your medical source is not a qualified medical source as defined in § 404.1519g.
[82 FR 5866, Jan. 18, 2017]
§ 404.1519j Objections to the medical source designated to perform the consultative examination.
You or your representative may object to your being examined by a medical source we have designated to perform a consultative examination. If there is a good reason for the objection, we will schedule the examination with another medical source. A good reason may be that the medical source we designated had previously represented an interest adverse to you. For example, the medical source may have represented your employer in a workers' compensation case or may have been involved in an insurance claim or legal action adverse to you. Other things we will consider include: The presence of a language barrier, the medical source's office location (e.g., 2nd floor, no elevator), travel restrictions, and whether the medical source had examined you in connection with a previous disability determination or decision that was unfavorable to you. If your objection is that a medical source allegedly “lacks objectivity” in general, but not in relation to you personally, we will review the allegations. See § 404.1519s. To avoid a delay in processing your claim, the consultative examination in your case will be changed to another medical source while a review is being conducted. We will handle any objection to use of the substitute medical source in the same manner. However, if we had previously conducted such a review and found that the reports of the medical source in question conformed to our guidelines, we will not change your examination.
[65 FR 11876, Mar. 7, 2000]
§ 404.1519k Purchase of medical examinations, laboratory tests, and other services.
We may purchase medical examinations, including psychiatric and psychological examinations, X-rays and laboratory tests (including specialized tests, such as pulmonary function studies, electrocardiograms, and stress tests) from a medical source.
(a) The rate of payment for purchasing medical or other services necessary to make determinations of disability may not exceed the highest rate paid by Federal or public agencies in the State for the same or similar types of service. See §§ 404.1624 and 404.1626 of this part.
(b) If a physician's bill or a request for payment for a physician's services includes a charge for a laboratory test for which payment may be made under this part, the amount payable with respect to the test shall be determined as follows:
(1) If the bill or request for payment indicates that the test was personally performed or supervised by the physician who submitted the bill (or for whose services the request for payment was made) or by another physician with whom that physician shares his or her practice, the payment will be based on the physician's usual and customary charge for the test or the rates of payment which the State uses for purchasing such services, whichever is the lesser amount.
(2) If the bill or request for payment indicates that the test was performed by an independent laboratory, the amount of reimbursement will not exceed the billed cost of the independent laboratory or the rate of payment which the State uses for purchasing such services, whichever is the lesser amount. A nominal payment may be made to the physician for collecting, handling and shipping a specimen to the laboratory if the physician bills for such a service. The total reimbursement may not exceed the rate of payment which the State uses for purchasing such services.
(c) The State will assure that it can support the rate of payment it uses. The State shall also be responsible for monitoring and overseeing the rate of payment it uses to ensure compliance with paragraphs (a) and (b) of this section.
[56 FR 36957, Aug. 1, 1991, as amended at 65 FR 11876, Mar. 7, 2000; 71 FR 16444, Mar. 31, 2006; 76 FR 24806, May 3, 2011]
§ 404.1519m Diagnostic tests or procedures.
We will request the results of any diagnostic tests or procedures that have been performed as part of a workup by your treating source or other medical source and will use the results to help us evaluate impairment severity or prognosis. However, we will not order diagnostic tests or procedures that involve significant risk to you, such as myelograms, arteriograms, or cardiac catheterizations for the evaluation of disability under the Social Security program. A State agency medical consultant must approve the ordering of any diagnostic test or procedure when there is a chance it may involve significant risk. The responsibility for deciding whether to perform the examination rests with the medical source designated to perform the consultative examination.
[56 FR 36957, Aug. 1, 1991, as amended at 65 FR 11876, Mar. 7, 2000; 71 FR 16444, Mar. 31, 2006; 76 FR 24806, May 3, 2011]
§ 404.1519n Informing the medical source of examination scheduling, report content, and signature requirements.
The medical sources who perform consultative examinations will have a good understanding of our disability programs and their evidentiary requirements. They will be made fully aware of their responsibilities and obligations regarding confidentiality as described in § 401.105(e). We will fully inform medical sources who perform consultative examinations at the time we first contact them, and at subsequent appropriate intervals, of the following obligations:
(a) Scheduling. In scheduling full consultative examinations, sufficient time should be allowed to permit the medical source to take a case history and perform the examination, including any needed tests. The following minimum scheduling intervals (i.e., time set aside for the individual, not the actual duration of the consultative examination) should be used.
(1) Comprehensive general medical examination—at least 30 minutes;
(2) Comprehensive musculoskeletal or neurological examination—at least 20 minutes;
(3) Comprehensive psychiatric examination—at least 40 minutes;
(4) Psychological examination—at least 60 minutes (Additional time may be required depending on types of psychological tests administered); and
(5) All others—at least 30 minutes, or in accordance with accepted medical practices.
We recognize that actual practice will dictate that some examinations may require longer scheduling intervals depending on the circumstances in a particular situation. We also recognize that these minimum intervals may have to be adjusted to allow for those claimants who do not attend their scheduled examination. The purpose of these minimum scheduling timeframes is to ensure that such examinations are complete and that sufficient time is made available to obtain the information needed to make an accurate determination in your case. State agencies will monitor the scheduling of examinations (through their normal consultative examination oversight activities) to ensure that any overscheduling is avoided, as overscheduling may lead to examinations that are not thorough.
(b) Report content. The reported results of your medical history, examination, requested laboratory findings, discussions and conclusions must conform to accepted professional standards and practices in the medical field for a complete and competent examination. The facts in a particular case and the information and findings already reported in the medical and other evidence of record will dictate the extent of detail needed in the consultative examination report for that case. Thus, the detail and format for reporting the results of a purchased examination will vary depending upon the type of examination or testing requested. The reporting of information will differ from one type of examination to another when the requested examination relates to the performance of tests such as ventilatory function tests, treadmill exercise tests, or audiological tests. The medical report must be complete enough to help us determine the nature, severity, and duration of the impairment, and residual functional capacity. The report should reflect your statement of your symptoms, not simply the medical source's statements or conclusions. The medical source's report of the consultative examination should include the objective medical facts as well as observations and opinions.
(c) Elements of a complete consultative examination. A complete consultative examination is one which involves all the elements of a standard examination in the applicable medical specialty. When the report of a complete consultative examination is involved, the report should include the following elements:
(1) Your major or chief complaint(s);
(2) A detailed description, within the area of specialty of the examination, of the history of your major complaint(s);
(3) A description, and disposition, of pertinent “positive” and “negative” detailed findings based on the history, examination and laboratory tests related to the major complaint(s), and any other abnormalities or lack thereof reported or found during examination or laboratory testing;
(4) The results of laboratory and other tests (e.g., X-rays) performed according to the requirements stated in the Listing of Impairments (see appendix 1 of this subpart P);
(5) The diagnosis and prognosis for your impairment(s);
(6) A medical opinion. Although we will ordinarily request a medical opinion as part of the consultative examination process, the absence of a medical opinion in a consultative examination report will not make the report incomplete. See § 404.1513(a)(3); and
(7) In addition, the medical source will consider, and provide some explanation or comment on, your major complaint(s) and any other abnormalities found during the history and examination or reported from the laboratory tests. The history, examination, evaluation of laboratory test results, and the conclusions will represent the information provided by the medical source who signs the report.
(d) When a complete consultative examination is not required. When the evidence we need does not require a complete consultative examination (for example, we need only a specific laboratory test result to complete the record), we may not require a report containing all of the elements in paragraph (c).
(e) Signature requirements. All consultative examination reports will be personally reviewed and signed by the medical source who actually performed the examination. This attests to the fact that the medical source doing the examination or testing is solely responsible for the report contents and for the conclusions, explanations or comments provided with respect to the history, examination and evaluation of laboratory test results. The signature of the medical source on a report annotated “not proofed” or “dictated but not read” is not acceptable. A rubber stamp signature of a medical source or the medical source's signature entered by any other person is not acceptable.
[56 FR 36958, Aug. 1, 1991, as amended at 65 FR 11876, Mar. 7, 2000; 82 FR 5866, Jan. 18, 2017]
§ 404.1519o When a properly signed consultative examination report has not been received.
If a consultative examination report is received unsigned or improperly signed we will take the following action.
(a) When we will make determinations and decisions without a properly signed report. We will make a determination or decision in the circumstances specified in paragraphs (a)(1) and (a)(2) of this section without waiting for a properly signed consultative examination report. After we have made the determination or decision, we will obtain a properly signed report and include it in the file unless the medical source who performed the original consultative examination has died:
(1) Continuous period of disability allowance with an onset date as alleged or earlier than alleged; or
(2) Continuance of disability.
(b) When we will not make determinations and decisions without a properly signed report. We will not use an unsigned or improperly signed consultative examination report to make the determinations or decisions specified in paragraphs (b)(1), (b)(2), (b)(3), and (b)(4) of this section. When we need a properly signed consultative examination report to make these determinations or decisions, we must obtain such a report. If the signature of the medical source who performed the original examination cannot be obtained because the medical source is out of the country for an extended period of time, or on an extended vacation, seriously ill, deceased, or for any other reason, the consultative examination will be rescheduled with another medical source:
(1) Denial; or
(2) Cessation; or
(3) Allowance of a period of disability which has ended; or
(4) Allowance with an onset date later than alleged.
[56 FR 36958, Aug. 1, 1991, as amended at 65 FR 11877, Mar. 7, 2000]
§ 404.1519p Reviewing reports of consultative examinations.
(a) We will review the report of the consultative examination to determine whether the specific information requested has been furnished. We will consider the following factors in reviewing the report:
(1) Whether the report provides evidence which serves as an adequate basis for decisionmaking in terms of the impairment it assesses;
(2) Whether the report is internally consistent; Whether all the diseases, impairments and complaints described in the history are adequately assessed and reported in the clinical findings; Whether the conclusions correlate the findings from your medical history, clinical examination and laboratory tests and explain all abnormalities;
(3) Whether the report is consistent with the other information available to us within the specialty of the examination requested; Whether the report fails to mention an important or relevant complaint within that specialty that is noted in other evidence in the file (e.g., your blindness in one eye, amputations, pain, alcoholism, depression);
(4) Whether this is an adequate report of examination as compared to standards set out in the course of a medical education; and
(5) Whether the report is properly signed.
(b) If the report is inadequate or incomplete, we will contact the medical source who performed the consultative examination, give an explanation of our evidentiary needs, and ask that the medical source furnish the missing information or prepare a revised report.
(c) With your permission, or when the examination discloses new diagnostic information or test results that reveal a potentially life-threatening situation, we will refer the consultative examination report to your treating source. When we refer the consultative examination report to your treating source without your permission, we will notify you that we have done so.
(d) We will perform ongoing special management studies on the quality of consultative examinations purchased from major medical sources and the appropriateness of the examinations authorized.
(e) We will take steps to ensure that consultative examinations are scheduled only with medical sources who have access to the equipment required to provide an adequate assessment and record of the existence and level of severity of your alleged impairments.
[56 FR 36959, Aug. 1, 1991, as amended at 65 FR 11877, Mar. 7, 2000]
§ 404.1519q Conflict of interest.
All implications of possible conflict of interest between medical or psychological consultants and their medical or psychological practices will be avoided. Such consultants are not only those physicians and psychologists who work for us directly but are also those who do review and adjudication work in the State agencies. Physicians and psychologists who work for us directly as employees or under contract will not work concurrently for a State agency. Physicians and psychologists who do review work for us will not perform consultative examinations for us without our prior approval. In such situations, the physician or psychologist will disassociate himself or herself from further involvement in the case and will not participate in the evaluation, decision, or appeal actions. In addition, neither they, nor any member of their families, will acquire or maintain, either directly or indirectly, any financial interest in a medical partnership, corporation, or similar relationship in which consultative examinations are provided. Sometimes physicians and psychologists who do review work for us will have prior knowledge of a case; for example, when the claimant was a patient. Where this is so, the physician or psychologist will not participate in the review or determination of the case. This does not preclude the physician or psychologist from submitting medical evidence based on treatment or examination of the claimant.
[56 FR 36959, Aug. 1, 1991]
Authorizing and Monitoring the Referral Process
§ 404.1519s Authorizing and monitoring the consultative examination.
(a) Day-to-day responsibility for the consultative examination process rests with the State agencies that make disability determinations for us.
(b) The State agency will maintain a good working relationship with the medical community in order to recruit sufficient numbers of physicians and other providers of medical services to ensure ready availability of consultative examination providers.
(c) Consistent with Federal and State laws, the State agency administrator will work to achieve appropriate rates of payment for purchased medical services.
(d) Each State agency will be responsible for comprehensive oversight management of its consultative examination program, with special emphasis on key providers.
(e) A key consultative examination provider is a provider that meets at least one of the following conditions:
(1) Any consultative examination provider with an estimated annual billing to the disability programs we administer of at least $150,000; or
(2) Any consultative examination provider with a practice directed primarily towards evaluation examinations rather than the treatment of patients; or
(3) Any consultative examination provider that does not meet the above criteria, but is one of the top five consultative examination providers in the State by dollar volume, as evidenced by prior year data.
(f) State agencies have flexibility in managing their consultative examination programs, but at a minimum will provide:
(1) An ongoing active recruitment program for consultative examination providers;
(2) A process for orientation, training, and review of new consultative examination providers, with respect to SSA's program requirements involving consultative examination report content and not with respect to medical techniques;
(3) Procedures for control of scheduling consultative examinations;
(4) Procedures to ensure that close attention is given to specific evaluation issues involved in each case;
(5) Procedures to ensure that only required examinations and tests are authorized in accordance with the standards set forth in this subpart;
(6) Procedures for providing medical or supervisory approval for the authorization or purchase of consultative examinations and for additional tests or studies requested by consulting medical sources. This includes physician approval for the ordering of any diagnostic test or procedure where the question of significant risk to the claimant/beneficiary might be raised. See § 404.1519m.
(7) Procedures for the ongoing review of consultative examination results to ensure compliance with written guidelines;
(8) Procedures to encourage active participation by physicians in the consultative examination oversight program;
(9) Procedures for handling complaints;
(10) Procedures for evaluating claimant reactions to key providers; and
(11) A program of systematic, onsite reviews of key providers that will include annual onsite reviews of such providers when claimants are present for examinations. This provision does not contemplate that such reviews will involve participation in the actual examinations but, rather, offer an opportunity to talk with claimants at the provider's site before and after the examination and to review the provider's overall operation.
(g) The State agencies will cooperate with us when we conduct monitoring activities in connection with their oversight management of their consultative examination programs.
[56 FR 36959, Aug. 1, 1991, as amended at 65 FR 11877, Mar. 7, 2000; 71 FR 16444, Mar. 31, 2006; 75 FR 32846, June 10, 2010; 76 FR 24806, May 3, 2011]
Procedures To Monitor the Consultative Examination
§ 404.1519t Consultative examination oversight.
(a) We will ensure that referrals for consultative examinations and purchases of consultative examinations are made in accordance with our policies. We will also monitor both the referral processes and the product of the consultative examinations obtained. This monitoring may include reviews by independent medical specialists under direct contract with SSA.
(b) Through our regional offices, we will undertake periodic comprehensive reviews of each State agency to evaluate each State's management of the consultative examination process. The review will involve visits to key providers, with State staff participating, including a program physician when the visit will deal with medical techniques or judgment, or factors that go to the core of medical professionalism.
(c) We will also perform ongoing special management studies of the quality of consultative examinations purchased from key providers and other sources and the appropriateness of the examinations authorized.
[56 FR 36960, Aug. 1, 1991]
Evaluation of Disability
§ 404.1520 Evaluation of disability in general.
(a) General —
(1) Purpose of this section. This section explains the five-step sequential evaluation process we use to decide whether you are disabled, as defined in § 404.1505.
(2) Applicability of these rules. These rules apply to you if you file an application for a period of disability or disability insurance benefits (or both) or for child's insurance benefits based on disability. They also apply if you file an application for widow's or widower's benefits based on disability for months after December 1990. (See § 404.1505(a).)
(3) Evidence considered. We will consider all evidence in your case record when we make a determination or decision whether you are disabled. See § 404.1520b.
(4) The five-step sequential evaluation process. The sequential evaluation process is a series of five “steps” that we follow in a set order. See paragraph (h) of this section for an exception to this rule. If we can find that you are disabled or not disabled at a step, we make our determination or decision and we do not go on to the next step. If we cannot find that you are disabled or not disabled at a step, we go on to the next step. Before we go from step three to step four, we assess your residual functional capacity. (See paragraph (e) of this section.) We use this residual functional capacity assessment at both step four and step five when we evaluate your claim at these steps. These are the five steps we follow:
(i) At the first step, we consider your work activity, if any. If you are doing substantial gainful activity, we will find that you are not disabled. (See paragraph (b) of this section.)
(ii) At the second step, we consider the medical severity of your impairment(s). If you do not have a severe medically determinable physical or mental impairment that meets the duration requirement in § 404.1509, or a combination of impairments that is severe and meets the duration requirement, we will find that you are not disabled. (See paragraph (c) of this section.)
(iii) At the third step, we also consider the medical severity of your impairment(s). If you have an impairment(s) that meets or equals one of our listings in appendix 1 of this subpart and meets the duration requirement, we will find that you are disabled. (See paragraph (d) of this section.)
(iv) At the fourth step, we consider our assessment of your residual functional capacity and your past relevant work. If you can still do your past relevant work, we will find that you are not disabled. See paragraphs (f) and (h) of this section and § 404.1560(b).
(v) At the fifth and last step, we consider our assessment of your residual functional capacity and your age, education, and work experience to see if you can make an adjustment to other work. If you can make an adjustment to other work, we will find that you are not disabled. If you cannot make an adjustment to other work, we will find that you are disabled. See paragraphs (g) and (h) of this section and § 404.1560(c).
(5) When you are already receiving disability benefits. If you are already receiving disability benefits, we will use a different sequential evaluation process to decide whether you continue to be disabled. We explain this process in § 404.1594(f).
(b) If you are working. If you are working and the work you are doing is substantial gainful activity, we will find that you are not disabled regardless of your medical condition or your age, education, and work experience.
(c) You must have a severe impairment. If you do not have any impairment or combination of impairments which significantly limits your physical or mental ability to do basic work activities, we will find that you do not have a severe impairment and are, therefore, not disabled. We will not consider your age, education, and work experience. However, it is possible for you to have a period of disability for a time in the past even though you do not now have a severe impairment.
(d) When your impairment(s) meets or equals a listed impairment in appendix 1. If you have an impairment(s) which meets the duration requirement and is listed in appendix 1 or is equal to a listed impairment(s), we will find you disabled without considering your age, education, and work experience.
(e) When your impairment(s) does not meet or equal a listed impairment. If your impairment(s) does not meet or equal a listed impairment, we will assess and make a finding about your residual functional capacity based on all the relevant medical and other evidence in your case record, as explained in § 404.1545. (See paragraph (g)(2) of this section and § 404.1562 for an exception to this rule.) We use our residual functional capacity assessment at the fourth step of the sequential evaluation process to determine if you can do your past relevant work (paragraph (f) of this section) and at the fifth step of the sequential evaluation process (if the evaluation proceeds to this step) to determine if you can adjust to other work (paragraph (g) of this section).
(f) Your impairment(s) must prevent you from doing your past relevant work. If we cannot make a determination or decision at the first three steps of the sequential evaluation process, we will compare our residual functional capacity assessment, which we made under paragraph (e) of this section, with the physical and mental demands of your past relevant work. See paragraph (h) of this section and § 404.1560(b). If you can still do this kind of work, we will find that you are not disabled.
(g) Your impairment(s) must prevent you from making an adjustment to any other work.
(1) If we find that you cannot do your past relevant work because you have a severe impairment(s) (or you do not have any past relevant work), we will consider the same residual functional capacity assessment we made under paragraph (e) of this section, together with your vocational factors (your age, education, and work experience) to determine if you can make an adjustment to other work. (See § 404.1560(c).) If you can make an adjustment to other work, we will find you not disabled. If you cannot, we will find you disabled.
(2) We use different rules if you meet one of the two special medical-vocational profiles described in § 404.1562. If you meet one of those profiles, we will find that you cannot make an adjustment to other work, and that you are disabled.
(h) Expedited process. If we do not find you disabled at the third step, and we do not have sufficient evidence about your past relevant work to make a finding at the fourth step, we may proceed to the fifth step of the sequential evaluation process. If we find that you can adjust to other work based solely on your age, education, and the same residual functional capacity assessment we made under paragraph (e) of this section, we will find that you are not disabled and will not make a finding about whether you can do your past relevant work at the fourth step. If we find that you may be unable to adjust to other work or if § 404.1562 may apply, we will assess your claim at the fourth step and make a finding about whether you can perform your past relevant work. See paragraph (g) of this section and § 404.1560(c).
[50 FR 8727, Mar. 5, 1985; 50 FR 19164, May 7, 1985, as amended at 56 FR 36960, Aug. 1, 1991; 65 FR 80308, Dec. 21, 2000; 68 FR 51161, Aug. 26, 2003; 77 FR 10655, Feb. 23, 2012; 77 FR 43494, July 25, 2012]
§ 404.1520a Evaluation of mental impairments.
(a) General. The steps outlined in § 404.1520 apply to the evaluation of physical and mental impairments. In addition, when we evaluate the severity of mental impairments for adults (persons age 18 and over) and in persons under age 18 when Part A of the Listing of Impairments is used, we must follow a special technique at each level in the administrative review process. We describe this special technique in paragraphs (b) through (e) of this section. Using the technique helps us:
(1) Identify the need for additional evidence to determine impairment severity;
(2) Consider and evaluate functional consequences of the mental disorder(s) relevant to your ability to work; and
(3) Organize and present our findings in a clear, concise, and consistent manner.
(b) Use of the technique.
(1) Under the special technique, we must first evaluate your pertinent symptoms, signs, and laboratory findings to determine whether you have a medically determinable mental impairment(s). See § 404.1521 for more information about what is needed to show a medically determinable impairment. If we determine that you have a medically determinable mental impairment(s), we must specify the symptoms, signs, and laboratory findings that substantiate the presence of the impairment(s) and document our findings in accordance with paragraph (e) of this section.
(2) We must then rate the degree of functional limitation resulting from the impairment(s) in accordance with paragraph (c) of this section and record our findings as set out in paragraph (e) of this section.
(c) Rating the degree of functional limitation.
(1) Assessment of functional limitations is a complex and highly individualized process that requires us to consider multiple issues and all relevant evidence to obtain a longitudinal picture of your overall degree of functional limitation. We will consider all relevant and available clinical signs and laboratory findings, the effects of your symptoms, and how your functioning may be affected by factors including, but not limited to, chronic mental disorders, structured settings, medication, and other treatment.
(2) We will rate the degree of your functional limitation based on the extent to which your impairment(s) interferes with your ability to function independently, appropriately, effectively, and on a sustained basis. Thus, we will consider such factors as the quality and level of your overall functional performance, any episodic limitations, the amount of supervision or assistance you require, and the settings in which you are able to function. See 12.00C through 12.00H of the Listing of Impairments in appendix 1 to this subpart for more information about the factors we consider when we rate the degree of your functional limitation.
(3) We have identified four broad functional areas in which we will rate the degree of your functional limitation: Understand, remember, or apply information; interact with others; concentrate, persist, or maintain pace; and adapt or manage oneself. See 12.00E of the Listing of Impairments in appendix 1 to this subpart.
(4) When we rate your degree of limitation in these areas (understand, remember, or apply information; interact with others; concentrate, persist, or maintain pace; and adapt or manage oneself), we will use the following five-point scale: None, mild, moderate, marked, and extreme. The last point on the scale represents a degree of limitation that is incompatible with the ability to do any gainful activity.
(d) Use of the technique to evaluate mental impairments. After we rate the degree of functional limitation resulting from your impairment(s), we will determine the severity of your mental impairment(s).
(1) If we rate the degrees of your limitation as “none” or “mild,” we will generally conclude that your impairment(s) is not severe, unless the evidence otherwise indicates that there is more than a minimal limitation in your ability to do basic work activities (see § 404.1522).
(2) If your mental impairment(s) is severe, we will then determine if it meets or is equivalent in severity to a listed mental disorder. We do this by comparing the medical findings about your impairment(s) and the rating of the degree of functional limitation to the criteria of the appropriate listed mental disorder. We will record the presence or absence of the criteria and the rating of the degree of functional limitation on a standard document at the initial and reconsideration levels of the administrative review process, or in the decision at the administrative law judge hearing and Appeals Council levels (in cases in which the Appeals Council issues a decision). See paragraph (e) of this section.
(3) If we find that you have a severe mental impairment(s) that neither meets nor is equivalent in severity to any listing, we will then assess your residual functional capacity.
(e) Documenting application of the technique. At the initial and reconsideration levels of the administrative review process, we will complete a standard document to record how we applied the technique. At the administrative law judge hearing and Appeals Council levels (in cases in which the Appeals Council issues a decision), we will document application of the technique in the decision. The following rules apply:
(1) When a State agency medical or psychological consultant makes the determination together with a State agency disability examiner at the initial or reconsideration level of the administrative review process as provided in § 404.1615(c)(1) of this part, the State agency medical or psychological consultant has overall responsibility for assessing medical severity. A State agency disability examiner may assist in preparing the standard document. However, our medical or psychological consultant must review and sign the document to attest that it is complete and that he or she is responsible for its content, including the findings of fact and any discussion of supporting evidence.
(2) When a State agency disability examiner makes the determination alone as provided in § 404.1615(c)(3), the State agency disability examiner has overall responsibility for assessing medical severity and for completing and signing the standard document.
(3) When a disability hearing officer makes a reconsideration determination as provided in § 404.1615(c)(4), the determination must document application of the technique, incorporating the disability hearing officer's pertinent findings and conclusions based on this technique.
(4) At the administrative law judge hearing and Appeals Council levels, the written decision must incorporate the pertinent findings and conclusions based on the technique. The decision must show the significant history, including examination and laboratory findings, and the functional limitations that were considered in reaching a conclusion about the severity of the mental impairment(s). The decision must include a specific finding as to the degree of limitation in each of the functional areas described in paragraph (c) of this section.
(5) If the administrative law judge requires the services of a medical expert to assist in applying the technique but such services are unavailable, the administrative law judge may return the case to the State agency or the appropriate Federal component, using the rules in § 404.941 of this part, for completion of the standard document. If, after reviewing the case file and completing the standard document, the State agency or Federal component concludes that a determination favorable to you is warranted, it will process the case using the rules found in § 404.941(d) or (e) of this part. If, after reviewing the case file and completing the standard document, the State agency or Federal component concludes that a determination favorable to you is not warranted, it will send the completed standard document and the case to the administrative law judge for further proceedings and a decision.
[65 FR 50774, Aug. 21, 2000; 65 FR 60584, Oct. 12, 2000, as amended at 71 FR 16444, Mar. 31, 2006; 75 FR 62680, Oct. 13, 2010; 76 FR 24806, May 3, 2011; 81 FR 66160, Sept. 26, 2016; 82 FR 5867. Jan. 18, 2017]
§ 404.1520b How we consider evidence.
After we review all of the evidence relevant to your claim, we make findings about what the evidence shows.
(a) Complete and consistent evidence. If all of the evidence we receive, including all medical opinion(s), is consistent and there is sufficient evidence for us to determine whether you are disabled, we will make our determination or decision based on that evidence.
(b) Incomplete or inconsistent evidence. In some situations, we may not be able to make our determination or decision because the evidence in your case record is insufficient or inconsistent. We consider evidence to be insufficient when it does not contain all the information we need to make our determination or decision. We consider evidence to be inconsistent when it conflicts with other evidence, contains an internal conflict, is ambiguous, or when the medical evidence does not appear to be based on medically acceptable clinical or laboratory diagnostic techniques. If the evidence in your case record is insufficient or inconsistent, we may need to take the additional actions in paragraphs (b)(1) through (4) of this section.
(1) If any of the evidence in your case record, including any medical opinion(s) and prior administrative medical findings, is inconsistent, we will consider the relevant evidence and see if we can determine whether you are disabled based on the evidence we have.
(2) If the evidence is consistent but we have insufficient evidence to determine whether you are disabled, or if after considering the evidence we determine we cannot reach a conclusion about whether you are disabled, we will determine the best way to resolve the inconsistency or insufficiency. The action(s) we take will depend on the nature of the inconsistency or insufficiency. We will try to resolve the inconsistency or insufficiency by taking any one or more of the actions listed in paragraphs (b)(2)(i) through (b)(2)(iv) of this section. We might not take all of the actions listed below. We will consider any additional evidence we receive together with the evidence we already have.
(i) We may recontact your medical source. We may choose not to seek additional evidence or clarification from a medical source if we know from experience that the source either cannot or will not provide the necessary evidence. If we obtain medical evidence over the telephone, we will send the telephone report to the source for review, signature, and return;
(ii) We may request additional existing evidence;
(iii) We may ask you to undergo a consultative examination at our expense (see §§ 404.1517 through 404.1519t); or
(iv) We may ask you or others for more information.
(3) When there are inconsistencies in the evidence that we cannot resolve or when, despite efforts to obtain additional evidence, the evidence is insufficient to determine whether you are disabled, we will make a determination or decision based on the evidence we have.
(c) Evidence that is inherently neither valuable nor persuasive. Paragraphs (c)(1) through (c)(3) apply in claims filed (see § 404.614) on or after March 27, 2017. Because the evidence listed in paragraphs (c)(1) through (c)(3) of this section is inherently neither valuable nor persuasive to the issue of whether you are disabled or blind under the Act, we will not provide any analysis about how we considered such evidence in our determination or decision, even under § 404.1520c:
(1) Decisions by other governmental agencies and nongovernmental entities. See § 404.1504.
(2) Disability examiner findings. Findings made by a State agency disability examiner made at a previous level of adjudication about a medical issue, vocational issue, or the ultimate determination about whether you are disabled.
(3) Statements on issues reserved to the Commissioner. The statements listed in paragraphs (c)(3)(i) through (c)(3)(viii) of this section would direct our determination or decision that you are or are not disabled or blind within the meaning of the Act, but we are responsible for making the determination or decision about whether you are disabled or blind:
(i) Statements that you are or are not disabled, blind, able to work, or able to perform regular or continuing work;
(ii) Statements about whether or not you have a severe impairment(s);
(iii) Statements about whether or not your impairment(s) meets the duration requirement (see § 404.1509);
(iv) Statements about whether or not your impairment(s) meets or medically equals any listing in the Listing of Impairments in Part 404, Subpart P, Appendix 1;
(v) Statements about what your residual functional capacity is using our programmatic terms about the functional exertional levels in Part 404, Subpart P, Appendix 2, Rule 200.00 instead of descriptions about your functional abilities and limitations (see § 404.1545);
(vi) Statements about whether or not your residual functional capacity prevents you from doing past relevant work (see § 404.1560);
(vii) Statements that you do or do not meet the requirements of a medical-vocational rule in Part 404, Subpart P, Appendix 2; and
(viii) Statements about whether or not your disability continues or ends when we conduct a continuing disability review (see § 404.1594).
[82 FR 5867, Jan. 18, 2017]
§ 404.1520c How we consider and articulate medical opinions and prior administrative medical findings for claims filed on or after March 27, 2017.
For claims filed (see § 404.614) on or after March 27, 2017, the rules in this section apply. For claims filed before March 27, 2017, the rules in § 404.1527 apply.
(a) How we consider medical opinions and prior administrative medical findings. We will not defer or give any specific evidentiary weight, including controlling weight, to any medical opinion(s) or prior administrative medical finding(s), including those from your medical sources. When a medical source provides one or more medical opinions or prior administrative medical findings, we will consider those medical opinions or prior administrative medical findings from that medical source together using the factors listed in paragraphs (c)(1) through (c)(5) of this section, as appropriate. The most important factors we consider when we evaluate the persuasiveness of medical opinions and prior administrative medical findings are supportability (paragraph (c)(1) of this section) and consistency (paragraph (c)(2) of this section). We will articulate how we considered the medical opinions and prior administrative medical findings in your claim according to paragraph (b) of this section.
(b) How we articulate our consideration of medical opinions and prior administrative medical findings. We will articulate in our determination or decision how persuasive we find all of the medical opinions and all of the prior administrative medical findings in your case record. Our articulation requirements are as follows:
(1) Source-level articulation. Because many claims have voluminous case records containing many types of evidence from different sources, it is not administratively feasible for us to articulate in each determination or decision how we considered all of the factors for all of the medical opinions and prior administrative medical findings in your case record. Instead, when a medical source provides multiple medical opinion(s) or prior administrative medical finding(s), we will articulate how we considered the medical opinions or prior administrative medical findings from that medical source together in a single analysis using the factors listed in paragraphs (c)(1) through (c)(5) of this section, as appropriate. We are not required to articulate how we considered each medical opinion or prior administrative medical finding from one medical source individually.
(2) Most important factors. The factors of supportability (paragraph (c)(1) of this section) and consistency (paragraph (c)(2) of this section) are the most important factors we consider when we determine how persuasive we find a medical source's medical opinions or prior administrative medical findings to be. Therefore, we will explain how we considered the supportability and consistency factors for a medical source's medical opinions or prior administrative medical findings in your determination or decision. We may, but are not required to, explain how we considered the factors in paragraphs (c)(3) through (c)(5) of this section, as appropriate, when we articulate how we consider medical opinions and prior administrative medical findings in your case record.
(3) Equally persuasive medical opinions or prior administrative medical findings about the same issue. When we find that two or more medical opinions or prior administrative medical findings about the same issue are both equally well-supported (paragraph (c)(1) of this section) and consistent with the record (paragraph (c)(2) of this section) but are not exactly the same, we will articulate how we considered the other most persuasive factors in paragraphs (c)(3) through (c)(5) of this section for those medical opinions or prior administrative medical findings in your determination or decision.
(c) Factors. We will consider the following factors when we consider the medical opinion(s) and prior administrative medical finding(s) in your case:
(1) Supportability. The more relevant the objective medical evidence and supporting explanations presented by a medical source are to support his or her medical opinion(s) or prior administrative medical finding(s), the more persuasive the medical opinions or prior administrative medical finding(s) will be.
(2) Consistency. The more consistent a medical opinion(s) or prior administrative medical finding(s) is with the evidence from other medical sources and nonmedical sources in the claim, the more persuasive the medical opinion(s) or prior administrative medical finding(s) will be.
(3) Relationship with the claimant. This factor combines consideration of the issues in paragraphs (c)(3)(i) through (v) of this section.
(i) Length of the treatment relationship. The length of time a medical source has treated you may help demonstrate whether the medical source has a longitudinal understanding of your impairment(s).
(ii) Frequency of examinations. The frequency of your visits with the medical source may help demonstrate whether the medical source has a longitudinal understanding of your impairment(s).
(iii) Purpose of the treatment relationship. The purpose for treatment you received from the medical source may help demonstrate the level of knowledge the medical source has of your impairment(s).
(iv) Extent of the treatment relationship. The kinds and extent of examinations and testing the medical source has performed or ordered from specialists or independent laboratories may help demonstrate the level of knowledge the medical source has of your impairment(s).
(v) Examining relationship. A medical source may have a better understanding of your impairment(s) if he or she examines you than if the medical source only reviews evidence in your folder.
(4) Specialization. The medical opinion or prior administrative medical finding of a medical source who has received advanced education and training to become a specialist may be more persuasive about medical issues related to his or her area of specialty than the medical opinion or prior administrative medical finding of a medical source who is not a specialist in the relevant area of specialty.
(5) Other factors. We will consider other factors that tend to support or contradict a medical opinion or prior administrative medical finding. This includes, but is not limited to, evidence showing a medical source has familiarity with the other evidence in the claim or an understanding of our disability program's policies and evidentiary requirements. When we consider a medical source's familiarity with the other evidence in a claim, we will also consider whether new evidence we receive after the medical source made his or her medical opinion or prior administrative medical finding makes the medical opinion or prior administrative medical finding more or less persuasive.
(d) Evidence from nonmedical sources. We are not required to articulate how we considered evidence from nonmedical sources using the requirements in paragraphs (a)-(c) in this section.
[82 FR 5867, Jan. 18, 2017]
§ 404.1521 Establishing that you have a medically determinable impairment(s).
If you are not doing substantial gainful activity, we will then determine whether you have a medically determinable physical or mental impairment(s) (see § 404.1520(a)(4)(ii)). Your impairment(s) must result from anatomical, physiological, or psychological abnormalities that can be shown by medically acceptable clinical and laboratory diagnostic techniques. Therefore, a physical or mental impairment must be established by objective medical evidence from an acceptable medical source. We will not use your statement of symptoms, a diagnosis, or a medical opinion to establish the existence of an impairment(s). After we establish that you have a medically determinable impairment(s), then we determine whether your impairment(s) is severe.
[82 FR 5868, Jan. 18, 2017]
§ 404.1522 What we mean by an impairment(s) that is not severe.
(a) Non-severe impairment(s). An impairment or combination of impairments is not severe if it does not significantly limit your physical or mental ability to do basic work activities.
(b) Basic work activities. When we talk about basic work activities, we mean the abilities and aptitudes necessary to do most jobs. Examples of these include—
(1) Physical functions such as walking, standing, sitting, lifting, pushing, pulling, reaching, carrying, or handling;
(2) Capacities for seeing, hearing, and speaking;
(3) Understanding, carrying out, and remembering simple instructions;
(4) Use of judgment;
(5) Responding appropriately to supervision, co-workers and usual work situations; and
(6) Dealing with changes in a routine work setting.
[82 FR 5869, Jan. 18, 2017]
§ 404.1523 Multiple impairments.
(a) Unrelated severe impairments. We cannot combine two or more unrelated severe impairments to meet the 12-month duration test. If you have a severe impairment(s) and then develop another unrelated severe impairment(s) but neither one is expected to last for 12 months, we cannot find you disabled, even though the two impairments in combination last for 12 months.
(b) Concurrent impairments. If you have two or more concurrent impairments that, when considered in combination, are severe, we must determine whether the combined effect of your impairments can be expected to continue to be severe for 12 months. If one or more of your impairments improves or is expected to improve within 12 months, so that the combined effect of your remaining impairments is no longer severe, we will find that you do not meet the 12-month duration test.
(c) Combined effect. In determining whether your physical or mental impairment or impairments are of a sufficient medical severity that such impairment or impairments could be the basis of eligibility under the law, we will consider the combined effect of all of your impairments without regard to whether any such impairment, if considered separately, would be of sufficient severity. If we do find a medically severe combination of impairments, we will consider the combined impact of the impairments throughout the disability determination process. If we do not find that you have a medically severe combination of impairments, we will determine that you are not disabled (see § 404.1520).
[82 FR 5869, Jan. 18, 2017]
Medical Considerations
§ 404.1525 Listing of Impairments in appendix 1.
(a) What is the purpose of the Listing of Impairments? The Listing of Impairments (the listings) is in appendix 1 of this subpart. It describes for each of the major body systems impairments that we consider to be severe enough to prevent an individual from doing any gainful activity, regardless of his or her age, education, or work experience.
(b) How is appendix 1 organized? There are two parts in appendix 1:
(1) Part A contains criteria that apply to individuals age 18 and over. We may also use part A for individuals who are under age 18 if the disease processes have a similar effect on adults and children.
(2) Part B contains criteria that apply only to individuals who are under age 18; we never use the listings in part B to evaluate individuals who are age 18 or older. In evaluating disability for a person under age 18, we use part B first. If the criteria in part B do not apply, we may use the criteria in part A when those criteria give appropriate consideration to the effects of the impairment(s) in children. To the extent possible, we number the provisions in part B to maintain a relationship with their counterparts in part A.
(c) How do we use the listings?
(1) Most body system sections in parts A and B of appendix 1 are in two parts: an introduction, followed by the specific listings.
(2) The introduction to each body system contains information relevant to the use of the listings in that body system; for example, examples of common impairments in the body system and definitions used in the listings for that body system. We may also include specific criteria for establishing a diagnosis, confirming the existence of an impairment, or establishing that your impairment(s) satisfies the criteria of a particular listing in the body system. Even if we do not include specific criteria for establishing a diagnosis or confirming the existence of your impairment, you must still show that you have a severe medically determinable impairment(s), as defined in § 404.1521.
(3) In most cases, the specific listings follow the introduction in each body system, after the heading, Category of Impairments. Within each listing, we specify the objective medical and other findings needed to satisfy the criteria of that listing. We will find that your impairment(s) meets the requirements of a listing when it satisfies all of the criteria of that listing, including any relevant criteria in the introduction, and meets the duration requirement (see § 404.1509).
(4) Most of the listed impairments are permanent or expected to result in death. For some listings, we state a specific period of time for which your impairment(s) will meet the listing. For all others, the evidence must show that your impairment(s) has lasted or can be expected to last for a continuous period of at least 12 months.
(5) If your impairment(s) does not meet the criteria of a listing, it can medically equal the criteria of a listing. We explain our rules for medical equivalence in § 404.1526. We use the listings only to find that you are disabled or still disabled. If your impairment(s) does not meet or medically equal the criteria of a listing, we may find that you are disabled or still disabled at a later step in the sequential evaluation process.
(d) Can your impairment(s) meet a listing based only on a diagnosis? No. Your impairment(s) cannot meet the criteria of a listing based only on a diagnosis. To meet the requirements of a listing, you must have a medically determinable impairment(s) that satisfies all of the criteria in the listing.
(e) How do we consider your symptoms when we determine whether your impairment(s) meets a listing? Some listed impairments include symptoms, such as pain, as criteria. Section 404.1529(d)(2) explains how we consider your symptoms when your symptoms are included as criteria in a listing.
[71 FR 10428, Mar. 1, 2006, as amended at 76 FR 19696, Apr. 8, 2011; 82 FR 5868, Jan. 18, 2017]
§ 404.1526 Medical equivalence.
(a) What is medical equivalence? Your impairment(s) is medically equivalent to a listed impairment in appendix 1 if it is at least equal in severity and duration to the criteria of any listed impairment.
(b) How do we determine medical equivalence? We can find medical equivalence in three ways.
(1)
(i) If you have an impairment that is described in appendix 1, but —
(A) You do not exhibit one or more of the findings specified in the particular listing, or
(B) You exhibit all of the findings, but one or more of the findings is not as severe as specified in the particular listing,
(ii) We will find that your impairment is medically equivalent to that listing if you have other findings related to your impairment that are at least of equal medical significance to the required criteria.
(2) If you have an impairment(s) that is not described in appendix 1, we will compare your findings with those for closely analogous listed impairments. If the findings related to your impairment(s) are at least of equal medical significance to those of a listed impairment, we will find that your impairment(s) is medically equivalent to the analogous listing.
(3) If you have a combination of impairments, no one of which meets a listing (see § 404.1525(c)(3)), we will compare your findings with those for closely analogous listed impairments. If the findings related to your impairments are at least of equal medical significance to those of a listed impairment, we will find that your combination of impairments is medically equivalent to that listing.
(4) Section 404.1529(d)(3) explains how we consider your symptoms, such as pain, when we make findings about medical equivalence.
(c) What evidence do we consider when we determine if your impairment(s) medically equals a listing? When we determine if your impairment medically equals a listing, we consider all evidence in your case record about your impairment(s) and its effects on you that is relevant to this finding. We do not consider your vocational factors of age, education, and work experience (see, for example, § 404.1560(c)(1)). We also consider the opinion given by one or more medical or psychological consultants designated by the Commissioner. (See § 404.1616.)
(d) Who is a designated medical or psychological consultant? A medical or psychological consultant designated by the Commissioner includes any medical or psychological consultant employed or engaged to make medical judgments by the Social Security Administration, the Railroad Retirement Board, or a State agency authorized to make disability determinations. See § 404.1616 for the necessary qualifications for medical consultants and psychological consultants.
(e) Who is responsible for determining medical equivalence?
(1) In cases where the State agency or other designee of the Commissioner makes the initial or reconsideration disability determination, a State agency medical or psychological consultant or other designee of the Commissioner (see § 404.1616 of this part) has the overall responsibility for determining medical equivalence.
(2) For cases in the disability hearing process or otherwise decided by a disability hearing officer, the responsibility for determining medical equivalence rests with either the disability hearing officer or, if the disability hearing officer's reconsideration determination is changed under § 404.918 of this part, with the Associate Commissioner for Disability Policy or his or her delegate.
(3) For cases at the administrative law judge or Appeals Council level, the responsibility for deciding medical equivalence rests with the administrative law judge or Appeals Council.
[45 FR 55584, Aug. 20, 1980, as amended at 52 FR 33926, Sept. 9, 1987; 62 FR 38451, July 18, 1997; 65 FR 34957, June 1, 2000; 71 FR 10429, Mar. 1, 2006; 71 FR 16445, Mar. 31, 2006; 71 FR 57415, Sept. 29, 2006; 76 FR 24807, May 3, 2011; 82 FR 5869, Jan. 18, 2017; 82 FR 15132, Mar. 27, 2017]
§ 404.1527 Evaluating opinion evidence for claims filed before March 27, 2017.
For claims filed (see § 404.614) before March 27, 2017, the rules in this section apply. For claims filed on or after March 27, 2017, the rules in § 404.1520c apply.
(a) Definitions.
(1) Medical opinions. Medical opinions are statements from acceptable medical sources that reflect judgments about the nature and severity of your impairment(s), including your symptoms, diagnosis and prognosis, what you can still do despite impairment(s), and your physical or mental restrictions.
(2) Treating source. Treating source means your own acceptable medical source who provides you, or has provided you, with medical treatment or evaluation and who has, or has had, an ongoing treatment relationship with you. Generally, we will consider that you have an ongoing treatment relationship with an acceptable medical source when the medical evidence establishes that you see, or have seen, the source with a frequency consistent with accepted medical practice for the type of treatment and/or evaluation required for your medical condition(s). We may consider an acceptable medical source who has treated or evaluated you only a few times or only after long intervals (e.g., twice a year) to be your treating source if the nature and frequency of the treatment or evaluation is typical for your condition(s). We will not consider an acceptable medical source to be your treating source if your relationship with the source is not based on your medical need for treatment or evaluation, but solely on your need to obtain a report in support of your claim for disability. In such a case, we will consider the acceptable medical source to be a nontreating source.
(b) How we consider medical opinions. In determining whether you are disabled, we will always consider the medical opinions in your case record together with the rest of the relevant evidence we receive. See § 404.1520b.
(c) How we weigh medical opinions. Regardless of its source, we will evaluate every medical opinion we receive. Unless we give a treating source's medical opinion controlling weight under paragraph (c)(2) of this section, we consider all of the following factors in deciding the weight we give to any medical opinion.
(1) Examining relationship. Generally, we give more weight to the medical opinion of a source who has examined you than to the medical opinion of a medical source who has not examined you.
(2) Treatment relationship. Generally, we give more weight to medical opinions from your treating sources, since these sources are likely to be the medical professionals most able to provide a detailed, longitudinal picture of your medical impairment(s) and may bring a unique perspective to the medical evidence that cannot be obtained from the objective medical findings alone or from reports of individual examinations, such as consultative examinations or brief hospitalizations. If we find that a treating source's medical opinion on the issue(s) of the nature and severity of your impairment(s) is well-supported by medically acceptable clinical and laboratory diagnostic techniques and is not inconsistent with the other substantial evidence in your case record, we will give it controlling weight. When we do not give the treating source's medical opinion controlling weight, we apply the factors listed in paragraphs (c)(2)(i) and (c)(2)(ii) of this section, as well as the factors in paragraphs (c)(3) through (c)(6) of this section in determining the weight to give the medical opinion. We will always give good reasons in our notice of determination or decision for the weight we give your treating source's medical opinion.
(i) Length of the treatment relationship and the frequency of examination. Generally, the longer a treating source has treated you and the more times you have been seen by a treating source, the more weight we will give to the source's medical opinion. When the treating source has seen you a number of times and long enough to have obtained a longitudinal picture of your impairment, we will give the medical source's medical opinion more weight than we would give it if it were from a nontreating source.
(ii) Nature and extent of the treatment relationship. Generally, the more knowledge a treating source has about your impairment(s) the more weight we will give to the source's medical opinion. We will look at the treatment the source has provided and at the kinds and extent of examinations and testing the source has performed or ordered from specialists and independent laboratories. For example, if your ophthalmologist notices that you have complained of neck pain during your eye examinations, we will consider his or her medical opinion with respect to your neck pain, but we will give it less weight than that of another physician who has treated you for the neck pain. When the treating source has reasonable knowledge of your impairment(s), we will give the source's medical opinion more weight than we would give it if it were from a nontreating source.
(3) Supportability. The more a medical source presents relevant evidence to support a medical opinion, particularly medical signs and laboratory findings, the more weight we will give that medical opinion. The better an explanation a source provides for a medical opinion, the more weight we will give that medical opinion. Furthermore, because nonexamining sources have no examining or treating relationship with you, the weight we will give their medical opinions will depend on the degree to which they provide supporting explanations for their medical opinions. We will evaluate the degree to which these medical opinions consider all of the pertinent evidence in your claim, including medical opinions of treating and other examining sources.
(4) Consistency. Generally, the more consistent a medical opinion is with the record as a whole, the more weight we will give to that medical opinion.
(5) Specialization. We generally give more weight to the medical opinion of a specialist about medical issues related to his or her area of specialty than to the medical opinion of a source who is not a specialist.
(6) Other factors. When we consider how much weight to give to a medical opinion, we will also consider any factors you or others bring to our attention, or of which we are aware, which tend to support or contradict the medical opinion. For example, the amount of understanding of our disability programs and their evidentiary requirements that a medical source has, regardless of the source of that understanding, and the extent to which a medical source is familiar with the other information in your case record are relevant factors that we will consider in deciding the weight to give to a medical opinion.
(d) Medical source opinions on issues reserved to the Commissioner. Opinions on some issues, such as the examples that follow, are not medical opinions, as described in paragraph (a)(1) of this section, but are, instead, opinions on issues reserved to the Commissioner because they are administrative findings that are dispositive of a case; i.e., that would direct the determination or decision of disability.
(1) Opinions that you are disabled. We are responsible for making the determination or decision about whether you meet the statutory definition of disability. In so doing, we review all of the medical findings and other evidence that support a medical source's statement that you are disabled. A statement by a medical source that you are “disabled” or “unable to work” does not mean that we will determine that you are disabled.
(2) Other opinions on issues reserved to the Commissioner. We use medical sources, including your treating source, to provide evidence, including opinions, on the nature and severity of your impairment(s). Although we consider opinions from medical sources on issues such as whether your impairment(s) meets or equals the requirements of any impairment(s) in the Listing of Impairments in appendix 1 to this subpart, your residual functional capacity (see §§ 404.1545 and 404.1546), or the application of vocational factors, the final responsibility for deciding these issues is reserved to the Commissioner.
(3) We will not give any special significance to the source of an opinion on issues reserved to the Commissioner described in paragraphs (d)(1) and (d)(2) of this section.
(e) Evidence from our Federal or State agency medical or psychological consultants. The rules in § 404.1513a apply except that when an administrative law judge gives controlling weight to a treating source's medical opinion, the administrative law judge is not required to explain in the decision the weight he or she gave to the prior administrative medical findings in the claim.
(f) Opinions from medical sources who are not acceptable medical sources and from nonmedical sources.
(1) Consideration. Opinions from medical sources who are not acceptable medical sources and from nonmedical sources may reflect the source's judgment about some of the same issues addressed in medical opinions from acceptable medical sources. Although we will consider these opinions using the same factors as listed in paragraph (c)(1) through (c)(6) in this section, not every factor for weighing opinion evidence will apply in every case because the evaluation of an opinion from a medical source who is not an acceptable medical source or from a nonmedical source depends on the particular facts in each case. Depending on the particular facts in a case, and after applying the factors for weighing opinion evidence, an opinion from a medical source who is not an acceptable medical source or from a nonmedical source may outweigh the medical opinion of an acceptable medical source, including the medical opinion of a treating source. For example, it may be appropriate to give more weight to the opinion of a medical source who is not an acceptable medical source if he or she has seen the individual more often than the treating source, has provided better supporting evidence and a better explanation for the opinion, and the opinion is more consistent with the evidence as a whole.
(2) Articulation. The adjudicator generally should explain the weight given to opinions from these sources or otherwise ensure that the discussion of the evidence in the determination or decision allows a claimant or subsequent reviewer to follow the adjudicator's reasoning, when such opinions may have an effect on the outcome of the case. In addition, when an adjudicator determines that an opinion from such a source is entitled to greater weight than a medical opinion from a treating source, the adjudicator must explain the reasons in the notice of decision in hearing cases and in the notice of determination (that is, in the personalized disability notice) at the initial and reconsideration levels, if the determination is less than fully favorable.
[82 FR 5869, Jan. 18, 2017; 82 FR 15132, Mar. 27, 2017]
§ 404.1528 [Reserved]
§ 404.1529 How we evaluate symptoms, including pain.
(a) General. In determining whether you are disabled, we consider all your symptoms, including pain, and the extent to which your symptoms can reasonably be accepted as consistent with the objective medical evidence and other evidence. We will consider all of your statements about your symptoms, such as pain, and any description your medical sources or nonmedical sources may provide about how the symptoms affect your activities of daily living and your ability to work. However, statements about your pain or other symptoms will not alone establish that you are disabled. There must be objective medical evidence from an acceptable medical source that shows you have a medical impairment(s) which could reasonably be expected to produce the pain or other symptoms alleged and that, when considered with all of the other evidence (including statements about the intensity and persistence of your pain or other symptoms which may reasonably be accepted as consistent with the medical signs and laboratory findings), would lead to a conclusion that you are disabled. In evaluating the intensity and persistence of your symptoms, including pain, we will consider all of the available evidence, including your medical history, the medical signs and laboratory findings, and statements about how your symptoms affect you. We will then determine the extent to which your alleged functional limitations and restrictions due to pain or other symptoms can reasonably be accepted as consistent with the medical signs and laboratory findings and other evidence to decide how your symptoms affect your ability to work.
(b) Need for medically determinable impairment that could reasonably be expected to produce your symptoms, such as pain. Your symptoms, such as pain, fatigue, shortness of breath, weakness, or nervousness, will not be found to affect your ability to do basic work activities unless medical signs or laboratory findings show that a medically determinable impairment(s) is present. Medical signs and laboratory findings, established by medically acceptable clinical or laboratory diagnostic techniques, must show the existence of a medical impairment(s) which results from anatomical, physiological, or psychological abnormalities and which could reasonably be expected to produce the pain or other symptoms alleged. In cases decided by a State agency (except in disability hearings under §§ 404.914 through 404.918 of this part and in fully favorable determinations made by State agency disability examiners alone under § 404.1615(c)(3) of this part), a State agency medical or psychological consultant or other medical or psychological consultant designated by the Commissioner directly participates in determining whether your medically determinable impairment(s) could reasonably be expected to produce your alleged symptoms. In the disability hearing process, a medical or psychological consultant may provide an advisory assessment to assist a disability hearing officer in determining whether your impairment(s) could reasonably be expected to produce your alleged symptoms. At the administrative law judge hearing or Appeals Council level of the administrative review process, the adjudicator(s) may ask for and consider the opinion of a medical or psychological expert concerning whether your impairment(s) could reasonably be expected to produce your alleged symptoms. The finding that your impairment(s) could reasonably be expected to produce your pain or other symptoms does not involve a determination as to the intensity, persistence, or functionally limiting effects of your symptoms. We will develop evidence regarding the possibility of a medically determinable mental impairment when we have information to suggest that such an impairment exists, and you allege pain or other symptoms but the medical signs and laboratory findings do not substantiate any physical impairment(s) capable of producing the pain or other symptoms.
(c) Evaluating the intensity and persistence of your symptoms, such as pain, and determining the extent to which your symptoms limit your capacity for work —
(1) General. When the medical signs or laboratory findings show that you have a medically determinable impairment(s) that could reasonably be expected to produce your symptoms, such as pain, we must then evaluate the intensity and persistence of your symptoms so that we can determine how your symptoms limit your capacity for work. In evaluating the intensity and persistence of your symptoms, we consider all of the available evidence from your medical sources and nonmedical sources about how your symptoms affect you. We also consider the medical opinions as explained in § 404.1520c. Paragraphs (c)(2) through (c)(4) of this section explain further how we evaluate the intensity and persistence of your symptoms and how we determine the extent to which your symptoms limit your capacity for work, when the medical signs or laboratory findings show that you have a medically determinable impairment(s) that could reasonably be expected to produce your symptoms, such as pain.
(2) Consideration of objective medical evidence. Objective medical evidence is evidence obtained from the application of medically acceptable clinical and laboratory diagnostic techniques, such as evidence of reduced joint motion, muscle spasm, sensory deficit or motor disruption. Objective medical evidence of this type is a useful indicator to assist us in making reasonable conclusions about the intensity and persistence of your symptoms and the effect those symptoms, such as pain, may have on your ability to work. We must always attempt to obtain objective medical evidence and, when it is obtained, we will consider it in reaching a conclusion as to whether you are disabled. However, we will not reject your statements about the intensity and persistence of your pain or other symptoms or about the effect your symptoms have on your ability to work solely because the available objective medical evidence does not substantiate your statements.
(3) Consideration of other evidence. Because symptoms sometimes suggest a greater severity of impairment than can be shown by objective medical evidence alone, we will carefully consider any other information you may submit about your symptoms. The information that your medical sources or nonmedical sources provide about your pain or other symptoms (e.g., what may precipitate or aggravate your symptoms, what medications, treatments or other methods you use to alleviate them, and how the symptoms may affect your pattern of daily living) is also an important indicator of the intensity and persistence of your symptoms. Because symptoms, such as pain, are subjective and difficult to quantify, any symptom-related functional limitations and restrictions that your medical sources or nonmedical sources report, which can reasonably be accepted as consistent with the objective medical evidence and other evidence, will be taken into account as explained in paragraph (c)(4) of this section in reaching a conclusion as to whether you are disabled. We will consider all of the evidence presented, including information about your prior work record, your statements about your symptoms, evidence submitted by your medical sources, and observations by our employees and other persons. Section 404.1520c explains in detail how we consider medical opinions and prior administrative medical findings about the nature and severity of your impairment(s) and any related symptoms, such as pain. Factors relevant to your symptoms, such as pain, which we will consider include:
(i) Your daily activities;
(ii) The location, duration, frequency, and intensity of your pain or other symptoms;
(iii) Precipitating and aggravating factors;
(iv) The type, dosage, effectiveness, and side effects of any medication you take or have taken to alleviate your pain or other symptoms;
(v) Treatment, other than medication, you receive or have received for relief of your pain or other symptoms;
(vi) Any measures you use or have used to relieve your pain or other symptoms (e.g., lying flat on your back, standing for 15 to 20 minutes every hour, sleeping on a board, etc.); and
(vii) Other factors concerning your functional limitations and restrictions due to pain or other symptoms.
(4) How we determine the extent to which symptoms, such as pain, affect your capacity to perform basic work activities. In determining the extent to which your symptoms, such as pain, affect your capacity to perform basic work activities, we consider all of the available evidence described in paragraphs (c)(1) through (c)(3) of this section. We will consider your statements about the intensity, persistence, and limiting effects of your symptoms, and we will evaluate your statements in relation to the objective medical evidence and other evidence, in reaching a conclusion as to whether you are disabled. We will consider whether there are any inconsistencies in the evidence and the extent to which there are any conflicts between your statements and the rest of the evidence, including your history, the signs and laboratory findings, and statements by your medical sources or other persons about how your symptoms affect you. Your symptoms, including pain, will be determined to diminish your capacity for basic work activities to the extent that your alleged functional limitations and restrictions due to symptoms, such as pain, can reasonably be accepted as consistent with the objective medical evidence and other evidence.
(d) Consideration of symptoms in the disability determination process. We follow a set order of steps to determine whether you are disabled. If you are not doing substantial gainful activity, we consider your symptoms, such as pain, to evaluate whether you have a severe physical or mental impairment(s), and at each of the remaining steps in the process. Sections 404.1520 and 404.1520a explain this process in detail. We also consider your symptoms, such as pain, at the appropriate steps in our review when we consider whether your disability continues. Sections 404.1579 and 404.1594 explain the procedure we follow in reviewing whether your disability continues.
(1) Need to establish a severe medically determinable impairment(s). Your symptoms, such as pain, fatigue, shortness of breath, weakness, or nervousness, are considered in making a determination as to whether your impairment or combination of impairment(s) is severe. (See § 404.1520(c).)
(2) Decision whether the Listing of Impairments is met. Some listed impairments include symptoms usually associated with those impairments as criteria. Generally, when a symptom is one of the criteria in a listing, it is only necessary that the symptom be present in combination with the other criteria. It is not necessary, unless the listing specifically states otherwise, to provide information about the intensity, persistence, or limiting effects of the symptom as long as all other findings required by the specific listing are present.
(3) Decision whether the Listing of Impairments is medically equaled. If your impairment is not the same as a listed impairment, we must determine whether your impairment(s) is medically equivalent to a listed impairment. Section 404.1526 explains how we make this determination. Under § 404.1526(b), we will consider medical equivalence based on all evidence in your case record about your impairment(s) and its effects on you that is relevant to this finding. In considering whether your symptoms, signs, and laboratory findings are medically equal to the symptoms, signs, and laboratory findings of a listed impairment, we will look to see whether your symptoms, signs, and laboratory findings are at least equal in severity to the listed criteria. However, we will not substitute your allegations of pain or other symptoms for a missing or deficient sign or laboratory finding to raise the severity of your impairment(s) to that of a listed impairment. If the symptoms, signs, and laboratory findings of your impairment(s) are equivalent in severity to those of a listed impairment, we will find you disabled. If it does not, we will consider the impact of your symptoms on your residual functional capacity. (See paragraph (d)(4) of this section.)
(4) Impact of symptoms (including pain) on residual functional capacity. If you have a medically determinable severe physical or mental impairment(s), but your impairment(s) does not meet or equal an impairment listed in appendix 1 of this subpart, we will consider the impact of your impairment(s) and any related symptoms, including pain, on your residual functional capacity. (See § 404.1545.)
[56 FR 57941, Nov. 14, 1991, as amended at 62 FR 38451, July 18, 1997; 71 FR 10429, Mar. 1, 2006; 71 FR 16445, Mar. 31, 2006; 75 FR 62681, Oct. 13, 2010; 76 FR 24807, May 3, 2011; 82 FR 5871, Jan. 18, 2017]
§ 404.1530 Need to follow prescribed treatment.
(a) What treatment you must follow. In order to get benefits, you must follow treatment prescribed by your medical source(s) if this treatment is expected to restore your ability to work.
(b) When you do not follow prescribed treatment. If you do not follow the prescribed treatment without a good reason, we will not find you disabled or, if you are already receiving benefits, we will stop paying you benefits.
(c) Acceptable reasons for failure to follow prescribed treatment. We will consider your physical, mental, educational, and linguistic limitations (including any lack of facility with the English language) when determining if you have an acceptable reason for failure to follow prescribed treatment. The following are examples of a good reason for not following treatment:
(1) The specific medical treatment is contrary to the established teaching and tenets of your religion.
(2) The prescribed treatment would be cataract surgery for one eye, when there is an impairment of the other eye resulting in a severe loss of vision and is not subject to improvement through treatment.
(3) Surgery was previously performed with unsuccessful results and the same surgery is again being recommended for the same impairment.
(4) The treatment because of its magnitude (e.g., open heart surgery), unusual nature (e.g., organ transplant), or other reason is very risky for you; or
(5) The treatment involves amputation of an extremity, or a major part of an extremity.
[45 FR 55584, Aug. 20, 1980, as amended at 59 FR 1635, Jan. 12, 1994; 82 FR 5871, Jan. 18, 2017]
§ 404.1535 How we will determine whether your drug addiction or alcoholism is a contributing factor material to the determination of disability.
(a) General. If we find that you are disabled and have medical evidence of your drug addiction or alcoholism, we must determine whether your drug addiction or alcoholism is a contributing factor material to the determination of disability.
(b) Process we will follow when we have medical evidence of your drug addiction or alcoholism.
(1) The key factor we will examine in determining whether drug addiction or alcoholism is a contributing factor material to the determination of disability is whether we would still find you disabled if you stopped using drugs or alcohol.
(2) In making this determination, we will evaluate which of your current physical and mental limitations, upon which we based our current disability determination, would remain if you stopped using drugs or alcohol and then determine whether any or all of your remaining limitations would be disabling.
(i) If we determine that your remaining limitations would not be disabling, we will find that your drug addiction or alcoholism is a contributing factor material to the determination of disability.
(ii) If we determine that your remaining limitations are disabling, you are disabled independent of your drug addiction or alcoholism and we will find that your drug addiction or alcoholism is not a contributing factor material to the determination of disability.
[60 FR 8147, Feb. 10, 1995]
§ 404.1536 Treatment required for individuals whose drug addiction or alcoholism is a contributing factor material to the determination of disability.
(a) If we determine that you are disabled and drug addiction or alcoholism is a contributing factor material to the determination of disability (as described in § 404.1535), you must avail yourself of appropriate treatment for your drug addiction or alcoholism at an institution or facility approved by us when this treatment is available and make progress in your treatment. Generally, you are not expected to pay for this treatment. You will not be paid benefits for any month after the month we have notified you in writing that—
(1) You did not comply with the terms, conditions and requirements of the treatment which has been made available to you; or
(2) You did not avail yourself of the treatment after you had been notified that it is available to you.
(b) If your benefits are suspended for failure to comply with treatment requirements, your benefits can be reinstated in accordance with the rules in § 404.470.
[60 FR 8147, Feb. 10, 1995]
§ 404.1537 What we mean by appropriate treatment.
By appropriate treatment, we mean treatment for drug addiction or alcoholism that serves the needs of the individual in the least restrictive setting possible consistent with your treatment plan. These settings range from outpatient counseling services through a variety of residential treatment settings including acute detoxification, short-term intensive residential treatment, long-term therapeutic residential treatment, and long-term recovery houses. Appropriate treatment is determined with the involvement of a State licensed or certified addiction professional on the basis of a detailed assessment of the individual's presenting symptomatology, psychosocial profile, and other relevant factors. This assessment may lead to a determination that more than one treatment modality is appropriate for the individual. The treatment will be provided or overseen by an approved institution or facility. This treatment may include (but is not limited to)—
(a) Medical examination and medical management;
(b) Detoxification;
(c) Medication management to include substitution therapy (e.g., methadone);
(d) Psychiatric, psychological, psychosocial, vocational, or other substance abuse counseling in a residential or outpatient treatment setting; or
(e) Relapse prevention.
[60 FR 8148, Feb. 10, 1995]
§ 404.1538 What we mean by approved institutions or facilities.
Institutions or facilities that we may approve include—
(a) An institution or facility that furnishes medically recognized treatment for drug addiction or alcoholism in conformity with applicable Federal or State laws and regulations;
(b) An institution or facility used by or licensed by an appropriate State agency which is authorized to refer persons for treatment of drug addiction or alcoholism;
(c) State licensed or certified care providers;
(d) Programs accredited by the Commission on Accreditation for Rehabilitation Facilities (CARF) and/or the Joint Commission for the Accreditation of Healthcare Organizations (JCAHO) for the treatment of drug addiction or alcoholism;
(e) Medicare or Medicaid certified care providers; or
(f) Nationally recognized self-help drug addiction or alcoholism recovery programs (e.g., Alcoholics Anonymous or Narcotics Anonymous) when participation in these programs is specifically prescribed by a treatment professional at an institution or facility described in paragraphs (a) through (e) of this section as part of an individual's treatment plan.
[60 FR 8148, Feb. 10, 1995]
§ 404.1539 How we consider whether treatment is available.
Our determination about whether treatment is available to you for your drug addiction or your alcoholism will depend upon—
(a) The capacity of an approved institution or facility to admit you for appropriate treatment;
(b) The location of the approved institution or facility, or the place where treatment, services or resources could be provided to you;
(c) The availability and cost of transportation for you to the place of treatment;
(d) Your general health, including your ability to travel and capacity to understand and follow the prescribed treatment;
(e) Your particular condition and circumstances; and
(f) The treatment that is prescribed for your drug addiction or alcoholism.
[60 FR 8148, Feb. 10, 1995]
§ 404.1540 Evaluating compliance with the treatment requirements.
(a) General. Generally, we will consider information from the treatment institution or facility to evaluate your compliance with your treatment plan. The treatment institution or facility will:
(1) Monitor your attendance at and participation in treatment sessions;
(2) Provide reports of the results of any clinical testing (such as, hematological or urinalysis studies for individuals with drug addiction and hematological studies and breath analysis for individuals with alcoholism) when such tests are likely to yield important information;
(3) Provide observational reports from the treatment professionals familiar with your individual case (subject to verification and Federal confidentiality requirements); or
(4) Provide their assessment or views on your noncompliance with treatment requirements.
(b) Measuring progress. Generally, we will consider information from the treatment institution or facility to evaluate your progress in completing your treatment plan. Examples of milestones for measuring your progress with the treatment which has been prescribed for your drug addiction or alcoholism may include (but are not limited to)—
(1) Abstinence from drug or alcohol use (initial progress may include significant reduction in use);
(2) Consistent attendance at and participation in treatment sessions;
(3) Improved social functioning and levels of gainful activity;
(4) Participation in vocational rehabilitation activities; or
(5) Avoidance of criminal activity.
[60 FR 8148, Feb. 10, 1995]
§ 404.1541 Establishment and use of referral and monitoring agencies.
We will contract with one or more agencies in each of the States, Puerto Rico and the District of Columbia to provide services to individuals whose disabilities are based on a determination that drug addiction or alcoholism is a contributing factor material to the determination of disability (as described in § 404.1535) and to submit information to us which we will use to make decisions about these individuals' benefits. These agencies will be known as referral and monitoring agencies. Their duties and responsibilities include (but are not limited to)—
(a) Identifying appropriate treatment placements for individuals we refer to them;
(b) Referring these individuals for treatment;
(c) Monitoring the compliance and progress with the appropriate treatment of these individuals; and
(d) Promptly reporting to us any individual's failure to comply with treatment requirements as well as failure to achieve progress through the treatment.
[60 FR 8148, Feb. 10, 1995]
Residual Functional Capacity
§ 404.1545 Your residual functional capacity.
(a) General —
(1) Residual functional capacity assessment. Your impairment(s), and any related symptoms, such as pain, may cause physical and mental limitations that affect what you can do in a work setting. Your residual functional capacity is the most you can still do despite your limitations. We will assess your residual functional capacity based on all the relevant evidence in your case record. (See §§ 404.1512(d) through (e).)
(2) If you have more than one impairment. We will consider all of your medically determinable impairments of which we are aware, including your medically determinable impairments that are not “severe,” as explained in §§ 404.1520(c), 404.1521, and 404.1523, when we assess your residual functional capacity. (See paragraph (e) of this section.)
(3) Evidence we use to assess your residual functional capacity. We will assess your residual functional capacity based on all of the relevant medical and other evidence. In general, you are responsible for providing the evidence we will use to make a finding about your residual functional capacity. (See § 404.1512(c).) However, before we make a determination that you are not disabled, we are responsible for developing your complete medical history, including arranging for a consultative examination(s) if necessary, and making every reasonable effort to help you get medical reports from your own medical sources. (See §§ 404.1512(d) through (f).) We will consider any statements about what you can still do that have been provided by medical sources, whether or not they are based on formal medical examinations. (See § 404.1513.) We will also consider descriptions and observations of your limitations from your impairment(s), including limitations that result from your symptoms, such as pain, provided by you, your family, neighbors, friends, or other persons. (See paragraph (e) of this section and § 404.1529.)
(4) What we will consider in assessing residual functional capacity. When we assess your residual functional capacity, we will consider your ability to meet the physical, mental, sensory, and other requirements of work, as described in paragraphs (b), (c), and (d) of this section.
(5) How we will use our residual functional capacity assessment.
(i) We will first use our residual functional capacity assessment at step four of the sequential evaluation process to decide if you can do your past relevant work. (See §§ 404.1520(f) and 404.1560(b).)
(ii) If we find that you cannot do your past relevant work, you do not have any past relevant work, or if we use the procedures in § 404.1520(h) and § 404.1562 does not apply, we will use the same assessment of your residual functional capacity at step five of the sequential evaluation process to decide if you can adjust to any other work that exists in the national economy. (See §§ 404.1520(g) and 404.1566.) At this step, we will not use our assessment of your residual functional capacity alone to decide if you are disabled. We will use the guidelines in §§ 404.1560 through 404.1569a, and consider our residual functional capacity assessment together with the information about your vocational background to make our disability determination or decision. For our rules on residual functional capacity assessment in deciding whether your disability continues or ends, see § 404.1594.
(b) Physical abilities. When we assess your physical abilities, we first assess the nature and extent of your physical limitations and then determine your residual functional capacity for work activity on a regular and continuing basis. A limited ability to perform certain physical demands of work activity, such as sitting, standing, walking, lifting, carrying, pushing, pulling, or other physical functions (including manipulative or postural functions, such as reaching, handling, stooping or crouching), may reduce your ability to do past work and other work.
(c) Mental abilities. When we assess your mental abilities, we first assess the nature and extent of your mental limitations and restrictions and then determine your residual functional capacity for work activity on a regular and continuing basis. A limited ability to carry out certain mental activities, such as limitations in understanding, remembering, and carrying out instructions, and in responding appropriately to supervision, co-workers, and work pressures in a work setting, may reduce your ability to do past work and other work.
(d) Other abilities affected by impairment(s). Some medically determinable impairment(s), such as skin impairment(s), epilepsy, impairment(s) of vision, hearing or other senses, and impairment(s) which impose environmental restrictions, may cause limitations and restrictions which affect other work-related abilities. If you have this type of impairment(s), we consider any resulting limitations and restrictions which may reduce your ability to do past work and other work in deciding your residual functional capacity.
(e) Total limiting effects. When you have a severe impairment(s), but your symptoms, signs, and laboratory findings do not meet or equal those of a listed impairment in appendix 1 of this subpart, we will consider the limiting effects of all your impairment(s), even those that are not severe, in determining your residual functional capacity. Pain or other symptoms may cause a limitation of function beyond that which can be determined on the basis of the anatomical, physiological or psychological abnormalities considered alone; e.g., someone with a low back disorder may be fully capable of the physical demands consistent with those of sustained medium work activity, but another person with the same disorder, because of pain, may not be capable of more than the physical demands consistent with those of light work activity on a sustained basis. In assessing the total limiting effects of your impairment(s) and any related symptoms, we will consider all of the medical and nonmedical evidence, including the information described in § 404.1529(c).
[56 FR 57943, Nov. 14, 1991, as amended at 68 FR 51162, Aug. 26, 2003; 77 FR 10656, Feb. 23, 2012; 77 FR 43494, July 25, 2012]
§ 404.1546 Responsibility for assessing your residual functional capacity.
(a) Responsibility for assessing residual functional capacity at the State agency. When a State agency medical or psychological consultant and a State agency disability examiner make the disability determination as provided in § 404.1615(c)(1) of this part, a State agency medical or psychological consultant(s) is responsible for assessing your residual functional capacity. When a State agency disability examiner makes a disability determination alone as provided in § 404.1615(c)(3), the disability examiner is responsible for assessing your residual functional capacity.
(b) Responsibility for assessing residual functional capacity in the disability hearings process. If your case involves a disability hearing under § 404.914, a disability hearing officer is responsible for assessing your residual functional capacity. However, if the disability hearing officer's reconsidered determination is changed under § 404.918, the Associate Commissioner for the Office of Disability Determinations or his or her delegate is responsible for assessing your residual functional capacity.
(c) Responsibility for assessing residual functional capacity at the administrative law judge hearing or Appeals Council level. If your case is at the administrative law judge hearing level or at the Appeals Council review level, the administrative law judge or the administrative appeals judge at the Appeals Council (when the Appeals Council makes a decision) is responsible for assessing your residual functional capacity.
[68 FR 51162, Aug. 26, 2003, as amended at 71 FR 16445, Mar. 31, 2006; 75 FR 62681, Oct. 13, 2010; 76 FR 24807, May 3, 2011]
Vocational Considerations
§ 404.1560 When we will consider your vocational background.
(a) General. If you are applying for a period of disability, or disability insurance benefits as a disabled worker, or child's insurance benefits based on disability which began before age 22, or widow's or widower's benefits based on disability for months after December 1990, and we cannot decide whether you are disabled at one of the first three steps of the sequential evaluation process (see § 404.1520), we will consider your residual functional capacity together with your vocational background, as discussed in paragraphs (b) and (c) of this section.
(b) Past relevant work. We will first compare our assessment of your residual functional capacity with the physical and mental demands of your past relevant work. See § 404.1520(h) for an exception to this rule.
(1) Definition of past relevant work. Past relevant work is work that you have done within the past 15 years, that was substantial gainful activity, and that lasted long enough for you to learn to do it. (See § 404.1565(a).)
(2) Determining whether you can do your past relevant work. We will ask you for information about work you have done in the past. We may also ask other people who know about your work. (See § 404.1565(b).) We may use the services of vocational experts or vocational specialists, or other resources, such as the “Dictionary of Occupational Titles” and its companion volumes and supplements, published by the Department of Labor, to obtain evidence we need to help us determine whether you can do your past relevant work, given your residual functional capacity. A vocational expert or specialist may offer relevant evidence within his or her expertise or knowledge concerning the physical and mental demands of a claimant's past relevant work, either as the claimant actually performed it or as generally performed in the national economy. Such evidence may be helpful in supplementing or evaluating the accuracy of the claimant's description of his past work. In addition, a vocational expert or specialist may offer expert opinion testimony in response to a hypothetical question about whether a person with the physical and mental limitations imposed by the claimant's medical impairment(s) can meet the demands of the claimant's previous work, either as the claimant actually performed it or as generally performed in the national economy.
(3) If you can do your past relevant work. If we find that you have the residual functional capacity to do your past relevant work, we will determine that you can still do your past work and are not disabled. We will not consider your vocational factors of age, education, and work experience or whether your past relevant work exists in significant numbers in the national economy.
(c) Other work.
(1) If we find that your residual functional capacity does not enable you to do any of your past relevant work or if we use the procedures in § 404.1520(h), we will use the same residual functional capacity assessment when we decide if you can adjust to any other work. We will look at your ability to adjust to other work by considering your residual functional capacity and the vocational factors of age, education, and work experience, as appropriate in your case. (See § 404.1520(h) for an exception to this rule.) Any other work (jobs) that you can adjust to must exist in significant numbers in the national economy (either in the region where you live or in several regions in the country).
(2) In order to support a finding that you are not disabled at this fifth step of the sequential evaluation process, we are responsible for providing evidence that demonstrates that other work exists in significant numbers in the national economy that you can do, given your residual functional capacity and vocational factors. We are not responsible for providing additional evidence about your residual functional capacity because we will use the same residual functional capacity assessment that we used to determine if you can do your past relevant work.
[68 FR 51163, Aug. 26, 2003, as amended at 77 FR 43494, July 25, 2012]
§ 404.1562 Medical-vocational profiles showing an inability to make an adjustment to other work.
(a) If you have done only arduous unskilled physical labor. If you have no more than a marginal education (see § 404.1564) and work experience of 35 years or more during which you did only arduous unskilled physical labor, and you are not working and are no longer able to do this kind of work because of a severe impairment(s) (see §§ 404.1520(c), 404.1521, and 404.1523), we will consider you unable to do lighter work, and therefore, disabled.
Example to paragraph (a):
B is a 58-year-old miner's helper with a fourth grade education who has a lifelong history of unskilled arduous physical labor. B says that he is disabled because of arthritis of the spine, hips, and knees, and other impairments. Medical evidence shows a “severe” combination of impairments that prevents B from performing his past relevant work. Under these circumstances, we will find that B is disabled.
(b) If you are at least 55 years old, have no more than a limited education, and have no past relevant work experience. If you have a severe, medically determinable impairment(s) (see §§ 404.1520(c), 404.1521, and 404.1523), are of advanced age (age 55 or older, see § 404.1563), have a limited education or less (see § 404.1564), and have no past relevant work experience (see § 404.1565), we will find you disabled. If the evidence shows that you meet this profile, we will not need to assess your residual functional capacity or consider the rules in appendix 2 to this subpart.
[68 FR 51163, Aug. 26, 2003]
§ 404.1563 Your age as a vocational factor.
(a) General. “Age” means your chronological age. When we decide whether you are disabled under § 404.1520(g)(1), we will consider your chronological age in combination with your residual functional capacity, education, and work experience. We will not consider your ability to adjust to other work on the basis of your age alone. In determining the extent to which age affects a person's ability to adjust to other work, we consider advancing age to be an increasingly limiting factor in the person's ability to make such an adjustment, as we explain in paragraphs (c) through (e) of this section. If you are unemployed but you still have the ability to adjust to other work, we will find that you are not disabled. In paragraphs (b) through (e) of this section and in appendix 2 to this subpart, we explain in more detail how we consider your age as a vocational factor.
(b) How we apply the age categories. When we make a finding about your ability to do other work under § 404.1520(f)(1), we will use the age categories in paragraphs (c) through (e) of this section. We will use each of the age categories that applies to you during the period for which we must determine if you are disabled. We will not apply the age categories mechanically in a borderline situation. If you are within a few days to a few months of reaching an older age category, and using the older age category would result in a determination or decision that you are disabled, we will consider whether to use the older age category after evaluating the overall impact of all the factors of your case.
(c) Younger person. If you are a younger person (under age 50), we generally do not consider that your age will seriously affect your ability to adjust to other work. However, in some circumstances, we consider that persons age 45-49 are more limited in their ability to adjust to other work than persons who have not attained age 45. See Rule 201.17 in appendix 2.
(d) Person closely approaching advanced age. If you are closely approaching advanced age (age 50-54), we will consider that your age along with a severe impairment(s) and limited work experience may seriously affect your ability to adjust to other work.
(e) Person of advanced age. We consider that at advanced age (age 55 or older), age significantly affects a person's ability to adjust to other work. We have special rules for persons of advanced age and for persons in this category who are closely approaching retirement age (age 60 or older). See § 404.1568(d)(4).
(f) Information about your age. We will usually not ask you to prove your age. However, if we need to know your exact age to determine whether you get disability benefits or if the amount of your benefit will be affected, we will ask you for evidence of your age.
[45 FR 55584, Aug. 20, 1980, as amended at 65 FR 18000, Apr. 6, 2000; 68 FR 51163, Aug. 26, 2003; 73 FR 64196, Oct. 29, 2008]
§ 404.1564 Your education as a vocational factor.
(a) General. Education is primarily used to mean formal schooling or other training which contributes to your ability to meet vocational requirements, for example, reasoning ability, communication skills, and arithmetical ability. However, if you do not have formal schooling, this does not necessarily mean that you are uneducated or lack these abilities. Past work experience and the kinds of responsibilities you had when you were working may show that you have intellectual abilities, although you may have little formal education. Your daily activities, hobbies, or the results of testing may also show that you have significant intellectual ability that can be used to work.
(b) How we evaluate your education. The importance of your educational background may depend upon how much time has passed between the completion of your formal education and the beginning of your physical or mental impairment(s) and by what you have done with your education in a work or other setting. Formal education that you completed many years before your impairment began, or unused skills and knowledge that were a part of your formal education, may no longer be useful or meaningful in terms of your ability to work. Therefore, the numerical grade level that you completed in school may not represent your actual educational abilities. These may be higher or lower. However, if there is no other evidence to contradict it, we will use your numerical grade level to determine your educational abilities. In evaluating your educational level, we use the following categories:
(1) Illiteracy. Illiteracy means the inability to read or write. We consider someone illiterate if the person cannot read or write a simple message such as instructions or inventory lists even though the person can sign his or her name. Generally, an illiterate person has had little or no formal schooling.
(2) Marginal education. Marginal education means ability in reasoning, arithmetic, and language skills which are needed to do simple, unskilled types of jobs. We generally consider that formal schooling at a 6th grade level or less is a marginal education.
(3) Limited education. Limited education means ability in reasoning, arithmetic, and language skills, but not enough to allow a person with these educational qualifications to do most of the more complex job duties needed in semi-skilled or skilled jobs. We generally consider that a 7th grade through the 11th grade level of formal education is a limited education.
(4) High school education and above. High school education and above means abilities in reasoning, arithmetic, and language skills acquired through formal schooling at a 12th grade level or above. We generally consider that someone with these educational abilities can do semi-skilled through skilled work.
(c) Information about your education. We will ask you how long you attended school, and whether you are able to understand, read, and write, and do at least simple arithmetic calculations. We will also consider other information about how much formal or informal education you may have had through your previous work, community projects, hobbies, and any other activities which might help you to work.
[45 FR 55584, Aug. 20, 1980, as amended at 85 FR 10602, Feb. 25, 2020]
§ 404.1565 Your work experience as a vocational factor.
(a) General. Work experience means skills and abilities you have acquired through work you have done which show the type of work you may be expected to do. Work you have already been able to do shows the kind of work that you may be expected to do. We consider that your work experience applies when it was done within the last 15 years, lasted long enough for you to learn to do it, and was substantial gainful activity. We do not usually consider that work you did 15 years or more before the time we are deciding whether you are disabled (or when the disability insured status requirement was last met, if earlier) applies. A gradual change occurs in most jobs so that after 15 years it is no longer realistic to expect that skills and abilities acquired in a job done then continue to apply. The 15-year guide is intended to insure that remote work experience is not currently applied. If you have no work experience or worked only “off-and-on” or for brief periods of time during the 15-year period, we generally consider that these do not apply. If you have acquired skills through your past work, we consider you to have these work skills unless you cannot use them in other skilled or semi-skilled work that you can now do. If you cannot use your skills in other skilled or semi-skilled work, we will consider your work background the same as unskilled. However, even if you have no work experience, we may consider that you are able to do unskilled work because it requires little or no judgment and can be learned in a short period of time.
(b) Information about your work. Under certain circumstances, we will ask you about the work you have done in the past. If you cannot give us all of the information we need, we may try, with your permission, to get it from your employer or other person who knows about your work, such as a member of your family or a co-worker. When we need to consider your work experience to decide whether you are able to do work that is different from what you have done in the past, we will ask you to tell us about all of the jobs you have had in the last 15 years. You must tell us the dates you worked, all of the duties you did, and any tools, machinery, and equipment you used. We will need to know about the amount of walking, standing, sitting, lifting and carrying you did during the work day, as well as any other physical or mental duties of your job. If all of your work in the past 15 years has been arduous and unskilled, and you have very little education, we will ask you to tell us about all of your work from the time you first began working. This information could help you to get disability benefits.
[45 FR 55584, Aug. 20, 1980, as amended at 77 FR 43494, July 25, 2012]
§ 404.1566 Work which exists in the national economy.
(a) General. We consider that work exists in the national economy when it exists in significant numbers either in the region where you live or in several other regions of the country. It does not matter whether—
(1) Work exists in the immediate area in which you live;
(2) A specific job vacancy exists for you; or
(3) You would be hired if you applied for work.
(b) How we determine the existence of work. Work exists in the national economy when there is a significant number of jobs (in one or more occupations) having requirements which you are able to meet with your physical or mental abilities and vocational qualifications. Isolated jobs that exist only in very limited numbers in relatively few locations outside of the region where you live are not considered “work which exists in the national economy”. We will not deny you disability benefits on the basis of the existence of these kinds of jobs. If work that you can do does not exist in the national economy, we will determine that you are disabled. However, if work that you can do does exist in the national economy, we will determine that you are not disabled.
(c) Inability to obtain work. We will determine that you are not disabled if your residual functional capacity and vocational abilities make it possible for you to do work which exists in the national economy, but you remain unemployed because of—
(1) Your inability to get work;
(2) Lack of work in your local area;
(3) The hiring practices of employers;
(4) Technological changes in the industry in which you have worked;
(5) Cyclical economic conditions;
(6) No job openings for you;
(7) You would not actually be hired to do work you could otherwise do; or
(8) You do not wish to do a particular type of work.
(d) Administrative notice of job data. When we determine that unskilled, sedentary, light, and medium jobs exist in the national economy (in significant numbers either in the region where you live or in several regions of the country), we will take administrative notice of reliable job information available from various governmental and other publications. For example, we will take notice of—
(1) Dictionary of Occupational Titles, published by the Department of Labor;
(2) County Business Patterns, published by the Bureau of the Census;
(3) Census Reports, also published by the Bureau of the Census;
(4) Occupational Analyses, prepared for the Social Security Administration by various State employment agencies; and
(5) Occupational Outlook Handbook, published by the Bureau of Labor Statistics.
(e) Use of vocational experts and other specialists. If the issue in determining whether you are disabled is whether your work skills can be used in other work and the specific occupations in which they can be used, or there is a similarly complex issue, we may use the services of a vocational expert or other specialist. We will decide whether to use a vocational expert or other specialist.
§ 404.1567 Physical exertion requirements.
To determine the physical exertion requirements of work in the national economy, we classify jobs as sedentary, light, medium, heavy, and very heavy. These terms have the same meaning as they have in the Dictionary of Occupational Titles, published by the Department of Labor. In making disability determinations under this subpart, we use the following definitions:
(a) Sedentary work. Sedentary work involves lifting no more than 10 pounds at a time and occasionally lifting or carrying articles like docket files, ledgers, and small tools. Although a sedentary job is defined as one which involves sitting, a certain amount of walking and standing is often necessary in carrying out job duties. Jobs are sedentary if walking and standing are required occasionally and other sedentary criteria are met.
(b) Light work. Light work involves lifting no more than 20 pounds at a time with frequent lifting or carrying of objects weighing up to 10 pounds. Even though the weight lifted may be very little, a job is in this category when it requires a good deal of walking or standing, or when it involves sitting most of the time with some pushing and pulling of arm or leg controls. To be considered capable of performing a full or wide range of light work, you must have the ability to do substantially all of these activities. If someone can do light work, we determine that he or she can also do sedentary work, unless there are additional limiting factors such as loss of fine dexterity or inability to sit for long periods of time.
(c) Medium work. Medium work involves lifting no more than 50 pounds at a time with frequent lifting or carrying of objects weighing up to 25 pounds. If someone can do medium work, we determine that he or she can also do sedentary and light work.
(d) Heavy work. Heavy work involves lifting no more than 100 pounds at a time with frequent lifting or carrying of objects weighing up to 50 pounds. If someone can do heavy work, we determine that he or she can also do medium, light, and sedentary work.
(e) Very heavy work. Very heavy work involves lifting objects weighing more than 100 pounds at a time with frequent lifting or carrying of objects weighing 50 pounds or more. If someone can do very heavy work, we determine that he or she can also do heavy, medium, light and sedentary work.
§ 404.1568 Skill requirements.
In order to evaluate your skills and to help determine the existence in the national economy of work you are able to do, occupations are classified as unskilled, semi-skilled, and skilled. In classifying these occupations, we use materials published by the Department of Labor. When we make disability determinations under this subpart, we use the following definitions:
(a) Unskilled work. Unskilled work is work which needs little or no judgment to do simple duties that can be learned on the job in a short period of time. The job may or may not require considerable strength. For example, we consider jobs unskilled if the primary work duties are handling, feeding and offbearing (that is, placing or removing materials from machines which are automatic or operated by others), or machine tending, and a person can usually learn to do the job in 30 days, and little specific vocational preparation and judgment are needed. A person does not gain work skills by doing unskilled jobs.
(b) Semi-skilled work. Semi-skilled work is work which needs some skills but does not require doing the more complex work duties. Semi-skilled jobs may require alertness and close attention to watching machine processes; or inspecting, testing or otherwise looking for irregularities; or tending or guarding equipment, property, materials, or persons against loss, damage or injury; or other types of activities which are similarly less complex than skilled work, but more complex than unskilled work. A job may be classified as semi-skilled where coordination and dexterity are necessary, as when hands or feet must be moved quickly to do repetitive tasks.
(c) Skilled work. Skilled work requires qualifications in which a person uses judgment to determine the machine and manual operations to be performed in order to obtain the proper form, quality, or quantity of material to be produced. Skilled work may require laying out work, estimating quality, determining the suitability and needed quantities of materials, making precise measurements, reading blueprints or other specifications, or making necessary computations or mechanical adjustments to control or regulate the work. Other skilled jobs may require dealing with people, facts, or figures or abstract ideas at a high level of complexity.
(d) Skills that can be used in other work (transferability) —
(1) What we mean by transferable skills. We consider you to have skills that can be used in other jobs, when the skilled or semi-skilled work activities you did in past work can be used to meet the requirements of skilled or semi-skilled work activities of other jobs or kinds of work. This depends largely on the similarity of occupationally significant work activities among different jobs.
(2) How we determine skills that can be transferred to other jobs. Transferability is most probable and meaningful among jobs in which—
(i) The same or a lesser degree of skill is required;
(ii) The same or similar tools and machines are used; and
(iii) The same or similar raw materials, products, processes, or services are involved.
(3) Degrees of transferability. There are degrees of transferability of skills ranging from very close similarities to remote and incidental similarities among jobs. A complete similarity of all three factors is not necessary for transferability. However, when skills are so specialized or have been acquired in such an isolated vocational setting (like many jobs in mining, agriculture, or fishing) that they are not readily usable in other industries, jobs, and work settings, we consider that they are not transferable.
(4) Transferability of skills for persons of advanced age. If you are of advanced age (age 55 or older), and you have a severe impairment(s) that limits you to sedentary or light work, we will find that you cannot make an adjustment to other work unless you have skills that you can transfer to other skilled or semiskilled work (or you have recently completed education which provides for direct entry into skilled work) that you can do despite your impairment(s). We will decide if you have transferable skills as follows. If you are of advanced age and you have a severe impairment(s) that limits you to no more than sedentary work, we will find that you have skills that are transferable to skilled or semiskilled sedentary work only if the sedentary work is so similar to your previous work that you would need to make very little, if any, vocational adjustment in terms of tools, work processes, work settings, or the industry. (See § 404.1567(a) and § 201.00(f) of appendix 2.) If you are of advanced age but have not attained age 60, and you have a severe impairment(s) that limits you to no more than light work, we will apply the rules in paragraphs (d)(1) through (d)(3) of this section to decide if you have skills that are transferable to skilled or semiskilled light work (see § 404.1567(b)). If you are closely approaching retirement age (age 60 or older) and you have a severe impairment(s) that limits you to no more than light work, we will find that you have skills that are transferable to skilled or semiskilled light work only if the light work is so similar to your previous work that you would need to make very little, if any, vocational adjustment in terms of tools, work processes, work settings, or the industry. (See § 404.1567(b) and Rule 202.00(f) of appendix 2 to this subpart.)
[45 FR 55584, Aug. 20, 1980, as amended at 65 FR 18000, Apr. 6, 2000; 73 FR 64197, Oct. 29, 2008]
§ 404.1569 Listing of Medical-Vocational Guidelines in appendix 2.
The Dictionary of Occupational Titles includes information about jobs (classified by their exertional and skill requirements) that exist in the national economy. Appendix 2 provides rules using this data reflecting major functional and vocational patterns. We apply these rules in cases where a person is not doing substantial gainful activity and is prevented by a severe medically determinable impairment from doing vocationally relevant past work. (See § 404.1520(h) for an exception to this rule.) The rules in appendix 2 do not cover all possible variations of factors. Also, as we explain in § 200.00 of appendix 2, we do not apply these rules if one of the findings of fact about the person's vocational factors and residual functional capacity is not the same as the corresponding criterion of a rule. In these instances, we give full consideration to all relevant facts in accordance with the definitions and discussions under vocational considerations. However, if the findings of fact made about all factors are the same as the rule, we use that rule to decide whether a person is disabled.
[45 FR 55584, Aug. 20, 1980, as amended at 77 FR 43494, July 25, 2012]
§ 404.1569a Exertional and nonexertional limitations.
(a) General. Your impairment(s) and related symptoms, such as pain, may cause limitations of function or restrictions which limit your ability to meet certain demands of jobs. These limitations may be exertional, nonexertional, or a combination of both. Limitations are classified as exertional if they affect your ability to meet the strength demands of jobs. The classification of a limitation as exertional is related to the United States Department of Labor's classification of jobs by various exertional levels (sedentary, light, medium, heavy, and very heavy) in terms of the strength demands for sitting, standing, walking, lifting, carrying, pushing, and pulling. Sections 404.1567 and 404.1569 explain how we use the classification of jobs by exertional levels (strength demands) which is contained in the Dictionary of Occupational Titles published by the Department of Labor, to determine the exertional requirements of work which exists in the national economy. Limitations or restrictions which affect your ability to meet the demands of jobs other than the strength demands, that is, demands other than sitting, standing, walking, lifting, carrying, pushing or pulling, are considered nonexertional. When we decide whether you can do your past relevant work (see §§ 404.1520(f) and 404.1594(f)(7)), we will compare our assessment of your residual functional capacity with the demands of your past relevant work. If you cannot do your past relevant work, we will use the same residual functional capacity assessment along with your age, education, and work experience to decide if you can adjust to any other work which exists in the national economy. (See §§ 404.1520(g) and 404.1594(f)(8).) Paragraphs (b), (c), and (d) of this section explain how we apply the medical-vocational guidelines in appendix 2 of this subpart in making this determination, depending on whether the limitations or restrictions imposed by your impairment(s) and related symptoms, such as pain, are exertional, nonexertional, or a combination of both.
(b) Exertional limitations. When the limitations and restrictions imposed by your impairment(s) and related symptoms, such as pain, affect only your ability to meet the strength demands of jobs (sitting, standing, walking, lifting, carrying, pushing, and pulling), we consider that you have only exertional limitations. When your impairment(s) and related symptoms only impose exertional limitations and your specific vocational profile is listed in a rule contained in appendix 2 of this subpart, we will directly apply that rule to decide whether you are disabled.
(c) Nonexertional limitations.
(1) When the limitations and restrictions imposed by your impairment(s) and related symptoms, such as pain, affect only your ability to meet the demands of jobs other than the strength demands, we consider that you have only nonexertional limitations or restrictions. Some examples of nonexertional limitations or restrictions include the following:
(i) You have difficulty functioning because you are nervous, anxious, or depressed;
(ii) You have difficulty maintaining attention or concentrating;
(iii) You have difficulty understanding or remembering detailed instructions;
(iv) You have difficulty in seeing or hearing;
(v) You have difficulty tolerating some physical feature(s) of certain work settings, e.g., you cannot tolerate dust or fumes; or
(vi) You have difficulty performing the manipulative or postural functions of some work such as reaching, handling, stooping, climbing, crawling, or crouching.
(2) If your impairment(s) and related symptoms, such as pain, only affect your ability to perform the nonexertional aspects of work-related activities, the rules in appendix 2 do not direct factual conclusions of disabled or not disabled. The determination as to whether disability exists will be based on the principles in the appropriate sections of the regulations, giving consideration to the rules for specific case situations in appendix 2.
(d) Combined exertional and nonexertional limitations. When the limitations and restrictions imposed by your impairment(s) and related symptoms, such as pain, affect your ability to meet both the strength and demands of jobs other than the strength demands, we consider that you have a combination of exertional and nonexertional limitations or restrictions. If your impairment(s) and related symptoms, such as pain, affect your ability to meet both the strength and demands of jobs other than the strength demands, we will not directly apply the rules in appendix 2 unless there is a rule that directs a conclusion that you are disabled based upon your strength limitations; otherwise the rules provide a framework to guide our decision.
[56 FR 57943, Nov. 14, 1991, as amended at 68 FR 51163, Aug. 26, 2003]
Substantial Gainful Activity
§ 404.1571 General.
The work, without regard to legality, that you have done during any period in which you believe you are disabled may show that you are able to work at the substantial gainful activity level. If you are able to engage in substantial gainful activity, we will find that you are not disabled. (We explain the rules for persons who are statutorily blind in § 404.1584.) Even if the work you have done was not substantial gainful activity, it may show that you are able to do more work than you actually did. We will consider all of the medical and vocational evidence in your file to decide whether or not you have the ability to engage in substantial gainful activity.
[45 FR 55584, Aug. 20, 1980, as amended at 65 FR 42783, July 11, 2000]
§ 404.1572 What we mean by substantial gainful activity.
Substantial gainful activity is work activity that is both substantial and gainful:
(a) Substantial work activity. Substantial work activity is work activity that involves doing significant physical or mental activities. Your work may be substantial even if it is done on a part-time basis or if you do less, get paid less, or have less responsibility than when you worked before.
(b) Gainful work activity. Gainful work activity is work activity that you do for pay or profit. Work activity is gainful if it is the kind of work usually done for pay or profit, whether or not a profit is realized.
(c) Some other activities. Generally, we do not consider activities like taking care of yourself, household tasks, hobbies, therapy, school attendance, club activities, or social programs to be substantial gainful activity.
§ 404.1573 General information about work activity.
(a) The nature of your work. If your duties require use of your experience, skills, supervision and responsibilities, or contribute substantially to the operation of a business, this tends to show that you have the ability to work at the substantial gainful activity level.
(b) How well you perform. We consider how well you do your work when we determine whether or not you are doing substantial gainful activity. If you do your work satisfactorily, this may show that you are working at the substantial gainful activity level. If you are unable, because of your impairments, to do ordinary or simple tasks satisfactorily without more supervision or assistance than is usually given other people doing similar work, this may show that you are not working at the substantial gainful activity level. If you are doing work that involves minimal duties that make little or no demands on you and that are of little or no use to your employer, or to the operation of a business if you are self-employed, this does not show that you are working at the substantial gainful activity level.
(c) If your work is done under special conditions. The work you are doing may be done under special conditions that take into account your impairment, such as work done in a sheltered workshop or as a patient in a hospital. If your work is done under special conditions, we may find that it does not show that you have the ability to do substantial gainful activity. Also, if you are forced to stop or reduce your work because of the removal of special conditions that were related to your impairment and essential to your work, we may find that your work does not show that you are able to do substantial gainful activity. However, work done under special conditions may show that you have the necessary skills and ability to work at the substantial gainful activity level. Examples of the special conditions that may relate to your impairment include, but are not limited to, situations in which—
(1) You required and received special assistance from other employees in performing your work;
(2) You were allowed to work irregular hours or take frequent rest periods;
(3) You were provided with special equipment or were assigned work especially suited to your impairment;
(4) You were able to work only because of specially arranged circumstances, for example, other persons helped you prepare for or get to and from your work;
(5) You were permitted to work at a lower standard of productivity or efficiency than other employees; or
(6) You were given the opportunity to work despite your impairment because of family relationship, past association with your employer, or your employer's concern for your welfare.
(d) If you are self-employed. Supervisory, managerial, advisory or other significant personal services that you perform as a self-employed individual may show that you are able to do substantial gainful activity.
(e) Time spent in work. While the time you spend in work is important, we will not decide whether or not you are doing substantial gainful activity only on that basis. We will still evaluate the work to decide whether it is substantial and gainful regardless of whether you spend more time or less time at the job than workers who are not impaired and who are doing similar work as a regular means of their livelihood.
[45 FR 55584, Aug. 20, 1980, as amended at 65 FR 42783, July 11, 2000]
§ 404.1574 Evaluation guides if you are an employee.
(a) We use several guides to decide whether the work you have done shows that you are able to do substantial gainful activity. If you are working or have worked as an employee, we will use the provisions in paragraphs (a) through (d) of this section that are relevant to your work activity. We will use these provisions whenever they are appropriate, whether in connection with your application for disability benefits (when we make an initial determination on your application and throughout any appeals you may request), after you have become entitled to a period of disability or to disability benefits, or both.
(1) Your earnings may show you have done substantial gainful activity. Generally, in evaluating your work activity for substantial gainful activity purposes, our primary consideration will be the earnings you derive from the work activity. We will use your earnings to determine whether you have done substantial gainful activity unless we have information from you, your employer, or others that shows that we should not count all of your earnings. The amount of your earnings from work you have done (regardless of whether it is unsheltered or sheltered work) may show that you have engaged in substantial gainful activity. Generally, if you worked for substantial earnings, we will find that you are able to do substantial gainful activity. However, the fact that your earnings were not substantial will not necessarily show that you are not able to do substantial gainful activity. We generally consider work that you are forced to stop or to reduce below the substantial gainful activity level after a short time because of your impairment to be an unsuccessful work attempt. Your earnings from an unsuccessful work attempt will not show that you are able to do substantial gainful activity. We will use the criteria in paragraph (c) of this section to determine if the work you did was an unsuccessful work attempt.
(2) We consider only the amounts you earn. When we decide whether your earnings show that you have done substantial gainful activity, we do not consider any income that is not directly related to your productivity. When your earnings exceed the reasonable value of the work you perform, we consider only that part of your pay which you actually earn. If your earnings are being subsidized, we do not consider the amount of the subsidy when we determine if your earnings show that you have done substantial gainful activity. We consider your work to be subsidized if the true value of your work, when compared with the same or similar work done by unimpaired persons, is less than the actual amount of earnings paid to you for your work. For example, when a person with a serious impairment does simple tasks under close and continuous supervision, our determination of whether that person has done substantial gainful activity will not be based only on the amount of the wages paid. We will first determine whether the person received a subsidy; that is, we will determine whether the person was being paid more than the reasonable value of the actual services performed. We will then subtract the value of the subsidy from the person's gross earnings to determine the earnings we will use to determine if he or she has done substantial gainful activity.
(3) If you are working in a sheltered or special environment. If you are working in a sheltered workshop, you may or may not be earning the amounts you are being paid. The fact that the sheltered workshop or similar facility is operating at a loss or is receiving some charitable contributions or governmental aid does not establish that you are not earning all you are being paid. Since persons in military service being treated for severe impairments usually continue to receive full pay, we evaluate work activity in a therapy program or while on limited duty by comparing it with similar work in the civilian work force or on the basis of reasonable worth of the work, rather than on the actual amount of the earnings.
(b) Earnings guidelines —
(1) General. If you are an employee, we first consider the criteria in paragraph (a) of this section and § 404.1576, and then the guides in paragraphs (b)(2) and (3) of this section. When we review your earnings to determine if you have been performing substantial gainful activity, we will subtract the value of any subsidized earnings (see paragraph (a)(2) of this section) and the reasonable cost of any impairment-related work expenses from your gross earnings (see § 404.1576). The resulting amount is the amount we use to determine if you have done substantial gainful activity. We will generally average your earnings for comparison with the earnings guidelines in paragraphs (b)(2) and (3) of this section. See § 404.1574a for our rules on averaging earnings.
(2) Earnings that will ordinarily show that you have engaged in substantial gainful activity. We will consider that your earnings from your work activity as an employee (including earnings from work in a sheltered workshop or a comparable facility especially set up for severely impaired persons) show that you engaged in substantial gainful activity if:
(i) Before January 1, 2001, they averaged more than the amount(s) in Table 1 of this section for the time(s) in which you worked.
(ii) Beginning January 1, 2001, and each year thereafter, they average more than the larger of:
(A) The amount for the previous year, or
(B) An amount adjusted for national wage growth, calculated by multiplying $700 by the ratio of the national average wage index for the year 2 calendar years before the year for which the amount is being calculated to the national average wage index for the year 1998. We will then round the resulting amount to the next higher multiple of $10 where such amount is a multiple of $5 but not of $10 and to the nearest multiple of $10 in any other case.
Table 1
| For months: | Your monthly earnings
averaged more than: |
|---|---|
| In calendar years before 1976 | $200 |
| In calendar year 1976 | 230 |
| In calendar year 1977 | 240 |
| In calendar year 1978 | 260 |
| In calendar year 1979 | 280 |
| In calendar years 1980-1989 | 300 |
| January 1990-June 1999 | 500 |
| July 1999-December 2000 | 700 |
(3) Earnings that will ordinarily show that you have not engaged in substantial gainful activity —
(i) General. If your average monthly earnings are equal to or less than the amount(s) determined under paragraph (b)(2) of this section for the year(s) in which you work, we will generally consider that the earnings from your work as an employee (including earnings from work in a sheltered workshop or comparable facility) will show that you have not engaged in substantial gainful activity. We will generally not consider other information in addition to your earnings except in the circumstances described in paragraph (b)(3)(ii) of this section.
(ii) When we will consider other information in addition to your earnings. We will generally consider other information in addition to your earnings if there is evidence indicating that you may be engaging in substantial gainful activity or that you are in a position to control when earnings are paid to you or the amount of wages paid to you (for example, if you are working for a small corporation owned by a relative). (See paragraph (b)(3)(iii) of this section for when we do not apply this rule.) Examples of other information we may consider include, whether—
(A) Your work is comparable to that of unimpaired people in your community who are doing the same or similar occupations as their means of livelihood, taking into account the time, energy, skill, and responsibility involved in the work; and
(B) Your work, although significantly less than that done by unimpaired people, is clearly worth the amounts shown in paragraph (b)(2) of this section, according to pay scales in your community.
(iii) Special rule for considering earnings alone when evaluating the work you do after you have received social security disability benefits for at least 24 months. Notwithstanding paragraph (b)(3)(ii) of this section, we will not consider other information in addition to your earnings to evaluate the work you are doing or have done if—
(A) At the time you do the work, you are entitled to social security disability benefits and you have received such benefits for at least 24 months (see paragraph (b)(3)(iv) of this section); and
(B) We are evaluating that work to consider whether you have engaged in substantial gainful activity or demonstrated the ability to engage in substantial gainful activity for the purpose of determining whether your disability has ceased because of your work activity (see §§ 404.1592a(a)(1) and (3)(ii) and 404.1594(d)(5) and (f)(1)).
(iv) When we consider you to have received social security disability benefits for at least 24 months. For purposes of paragraph (b)(3)(iii) of this section, social security disability benefits means disability insurance benefits for a disabled worker, child's insurance benefits based on disability, or widow's or widower's insurance benefits based on disability. We consider you to have received such benefits for at least 24 months beginning with the first day of the first month following the 24th month for which you actually received social security disability benefits that you were due or constructively received such benefits. The 24 months do not have to be consecutive. We will consider you to have constructively received a benefit for a month for purposes of the 24-month requirement if you were otherwise due a social security disability benefit for that month and your monthly benefit was withheld to recover an overpayment. Any months for which you were entitled to benefits but for which you did not actually or constructively receive a benefit payment will not be counted for the 24-month requirement. If you also receive supplemental security income payments based on disability or blindness under title XVI of the Social Security Act, months for which you received only supplemental security income payments will not be counted for the 24-month requirement.
(c) The unsuccessful work attempt —
(1) General. Ordinarily, work you have done will not show that you are able to do substantial gainful activity if, after you worked for a period of 6 months or less, your impairment forced you to stop working or to reduce the amount of work you do so that your earnings from such work fall below the substantial gainful activity earnings level in paragraph (b)(2) of this section, and you meet the conditions described in paragraphs (c)(2), (3), and (4) of this section. We will use the provisions of this paragraph when we make an initial determination on your application for disability benefits and throughout any appeal you may request. Except as set forth in § 404.1592a(a), we will also apply the provisions of this paragraph if you are already entitled to disability benefits, when you work and we consider whether the work you are doing is substantial gainful activity or demonstrates the ability to do substantial gainful activity.
(2) Event that must precede an unsuccessful work attempt. There must be a significant break in the continuity of your work before we will consider that you began a work attempt that later proved unsuccessful. You must have stopped working or reduced your work and earnings below the substantial gainful activity earnings level because of your impairment or because of the removal of special conditions that were essential to the further performance of your work. We explain what we mean by special conditions in § 404.1573(c). We will consider your prior work to be “discontinued” for a significant period if you were out of work at least 30 consecutive days. We will also consider your prior work to be “discontinued” if, because of your impairment, you were forced to change to another type of work or another employer.
(3) If you worked 6 months or less. We will consider work of 6 months or less to be an unsuccessful work attempt if you stopped working or you reduced your work and earnings below the substantial gainful activity earnings level because of your impairment or because of the removal of special conditions that took into account your impairment and permitted you to work.
(4) If you worked more than 6 months. We will not consider work you performed at the substantial gainful activity earnings level for more than 6 months to be an unsuccessful work attempt regardless of why it ended or was reduced below the substantial gainful activity earnings level.
(d) Work activity in certain volunteer programs. If you work as a volunteer in certain programs administered by the Federal government under the Domestic Volunteer Service Act of 1973 or the Small Business Act, we will not count any payments you receive from these programs as earnings when we determine whether you are engaging in substantial gainful activity. These payments may include a minimal stipend, payments for supportive services such as housing, supplies and equipment, an expense allowance, or reimbursement of out-of-pocket expenses. We will also disregard the services you perform as a volunteer in applying any of the substantial gainful activity tests discussed in paragraph (b)(6) of this section. This exclusion from the substantial gainful activity provisions will apply only if you are a volunteer in a program explicitly mentioned in the Domestic Volunteer Service Act of 1973 or the Small Business Act. Programs explicitly mentioned in those Acts include Volunteers in Service to America, University Year for ACTION, Special Volunteer Programs, Retired Senior Volunteer Program, Foster Grandparent Program, Service Corps of Retired Executives, and Active Corps of Executives. We will not exclude under this paragraph, volunteer work you perform in other programs or any nonvolunteer work you may perform, including nonvolunteer work under one of the specified programs. For civilians in certain government-sponsored job training and employment programs, we evaluate the work activity on a case-by-case basis under the substantial gainful activity earnings test. In programs such as these, subsidies often occur. We will subtract the value of any subsidy and use the remainder to determine if you have done substantial gainful activity. See paragraphs (a)(2)-(3) of this section.
(e) Work activity as a member or consultant of an advisory committee established under the Federal Advisory Committee Act (FACA), 5 U.S.C. App. 2. If you are serving as a member or consultant of an advisory committee, board, commission, council, or similar group established under FACA, we will not count any payments you receive from serving on such committees as earnings when we determine whether you are engaging in substantial gainful activity. These payments may include compensation, travel expenses, and special assistance. We also will exclude the services you perform as a member or consultant of an advisory committee established under FACA in applying any of the substantial gainful activity tests discussed in paragraph (b)(6) of this section. This exclusion from the substantial gainful activity provisions will apply only if you are a member or consultant of an advisory committee specifically authorized by statute, or by the President, or determined as a matter of formal record by the head of a federal government agency. This exclusion from the substantial gainful activity provisions will not apply if your service as a member or consultant of an advisory committee is part of your duties or is required as an employee of any governmental or non-governmental organization, agency, or business.
[46 FR 4869, Jan. 19, 1981, as amended at 48 FR 21936, May 16, 1983; 49 FR 22272, May 29, 1984; 54 FR 53605, Dec. 29, 1989; 64 FR 18570, Apr. 15, 1999; 64 FR 22903, Apr. 28, 1999; 65 FR 42783, July 11, 2000; 65 FR 82910, Dec. 29, 2000; 71 FR 3219, Jan. 20, 2006; 71 FR 66853, Nov. 17, 2006; 81 FR 71369, Oct. 17, 2016]
§ 404.1574a When and how we will average your earnings.
(a) If your work as an employee or as a self-employed person was continuous without significant change in work patterns or earnings, and there has been no change in the substantial gainful activity earnings levels, we will average your earnings over the entire period of work requiring evaluation to determine if you have done substantial gainful activity. See § 404.1592a for information on the reentitlement period.
(b) If you work over a period of time during which the substantial gainful activity earnings levels change, we will average your earnings separately for each period in which a different substantial gainful activity earnings level applies.
(c) If there is a significant change in your work pattern or earnings during the period of work requiring evaluation, we will average your earnings over each separate period of work to determine if any of your work efforts were substantial gainful activity.
(d) We will not average your earnings in determining whether benefits should be paid for any month(s) during or after the reentitlement period that occurs after the month disability has been determined to have ceased because of the performance of substantial gainful activity. See § 404.1592a for information on the reentitlement period. The following examples illustrate what we mean by a significant change in the work pattern of an employee and when we will average and will not average earnings.
Example 1:
Mrs. H. began receiving disability insurance benefits in March 1993. In January 1995 she began selling magazines by telephone solicitation, expending a minimum of time, for which she received $225 monthly. As a result, Mrs. H. used up her trial work period during the months of January 1995 through September 1995. After the trial work period ended, we determined that Mrs. H. had not engaged in substantial gainful activity during her trial work period. Her reentitlement period began October 1995. In December 1995, Mrs. H. discontinued her telephone solicitation work to take a course in secretarial skills. In January 1997, she began work as a part-time temporary secretary in a banking firm. Mrs. H. worked 20 hours a week, without any subsidy or impairment-related work expenses, at beginner rates. She earned $285 per month in January 1997 and February 1997. In March 1997 she had increased her secretarial skills to journeyman level and was assigned as a part-time private secretary to one of the vice presidents of the banking firm. Mrs. H.'s earnings increased to $525 per month effective March 1997. We determined that Mrs. H. was engaging in substantial gainful activity beginning March 1997 and that her disability ceased that month, the first month of substantial gainful activity after the end of the trial work period. Mrs. H. is due payment for March 1997, the month of cessation, and the following 2 months (April 1997 and May 1997) because disability benefits terminate the third month following the earliest month in which she performed substantial gainful activity. We did not average earnings for the period January 1997 and February 1997 with the period beginning March 1997 because there was a significant change in earnings and work activity beginning March 1997. Thus, the earnings of January 1997 and February 1997 could not be averaged with those of March 1997 to reduce March 1997 earnings below the substantial gainful activity level. After we determine that Mrs. H.'s disability had ceased because of her performance of substantial gainful activity, we cannot average her earnings to determine whether she is due payment for any month during or after the reentitlement period. Beginning June 1997, the third month following the cessation month, we would evaluate all of Mrs. H.'s work activity on a month-by-month basis (see § 404.1592a(a)).
Example 2:
Ms. M. began receiving disability insurance benefits in March 1992. In January 1995, she began selling cable television subscriptions by telephone solicitation, expending a minimum of time, for which she received $275 monthly. Ms. M. did not work in June 1995, and she resumed selling cable television subscriptions beginning July 1995. In this way, Ms. M. used up her 9-month trial work period during the months of January 1995 through May 1995 and July 1995 through October 1995. After Ms. M.'s trial work period ended, we determined that she had not engaged in substantial gainful activity during her trial work period. Ms. M.'s reentitlement period began November 1995. In December 1995, Ms. M. discontinued her telephone solicitation work to take a course in secretarial skills. In January 1997, she began work as a part-time temporary secretary in an accounting firm. Ms. M. worked, without any subsidy or impairment-related work expenses, at beginner rates. She earned $460 in January 1997, $420 in February 1997, and $510 in March 1997. In April 1997, she had increased her secretarial skills to journeyman level, and she was assigned as a part-time private secretary to one of the vice presidents of the firm. Ms. M.'s earnings increased to $860 per month effective April 1997. We determined that Ms. M. was engaging in substantial gainful activity beginning April 1997 and that her disability ceased that month, the first month of substantial gainful activity after the end of the trial work period. She is due payment for April 1997, May 1997 and June 1997, because disability benefits terminate the third month following the earliest month in which she performs substantial gainful activity (the month of cessation). We averaged her earnings for the period January 1997 through March 1997 and determined them to be about $467 per month for that period. We did not average earnings for the period January 1997 through March 1997 with earnings for the period beginning April 1997 because there was a significant change in work activity and earnings beginning April 1997. Therefore, we found that the earnings for January 1997 through March 1997 were under the substantial gainful activity level. After we determine that Ms. M.'s disability has ceased because she performed substantial gainful activity, we cannot average her earnings in determining whether she is due payment for any month during or after the reentitlement period. In this example, beginning July 1997, the third month following the month of cessation, we would evaluate all of Ms. M.'s work activity on a month-by-month basis (see § 404.1592a(a)).
[65 FR 42784, July 11, 2000]
§ 404.1575 Evaluation guides if you are self-employed.
(a) If you are a self-employed person. If you are working or have worked as a self-employed person, we will use the provisions in paragraphs (a) through (e) of this section that are relevant to your work activity. We will use these provisions whenever they are appropriate, whether in connection with your application for disability benefits (when we make an initial determination on your application and throughout any appeals you may request), after you have become entitled to a period of disability or to disability benefits, or both.
(1) How we evaluate the work you do after you have become entitled to disability benefits. If you are entitled to social security disability benefits and you work as a self-employed person, the way we will evaluate your work activity will depend on whether the work activity occurs before or after you have received such benefits for at least 24 months and on the purpose of the evaluation. For purposes of paragraphs (a) and (e) of this section, social security disability benefits means disability insurance benefits for a disabled worker, child's insurance benefits based on disability, or widow's or widower's insurance benefits based on disability. We will use the rules in paragraph (e)(2) of this section to determine if you have received such benefits for at least 24 months.
(i) We will use the guides in paragraph (a)(2) of this section to evaluate any work activity you do before you have received social security disability benefits for at least 24 months to determine whether you have engaged in substantial gainful activity, regardless of the purpose of the evaluation.
(ii) We will use the guides in paragraph (e) of this section to evaluate any work activity you do after you have received social security disability benefits for at least 24 months to determine whether you have engaged in substantial gainful activity for the purpose of determining whether your disability has ceased because of your work activity.
(iii) If we have determined under § 404.1592a(a)(1) that your disability ceased in a month during the reentitlement period because you performed substantial gainful activity, and we need to decide under § 404.1592a(a)(2)(i) or (a)(3)(i) whether you are doing substantial gainful activity in a subsequent month in or after your reentitlement period, we will use the guides in paragraph (a)(2) of this section (subject to the limitations described in § 404.1592a(a)(2)(i) and (a)(3)(i)) to determine whether your work activity in that month is substantial gainful activity. We will use the guides in paragraph (a)(2) of this section for these purposes, regardless of whether your work activity in that month occurs before or after you have received social security disability benefits for at least 24 months.
(2) General rules for evaluating your work activity if you are self-employed. We will consider your activities and their value to your business to decide whether you have engaged in substantial gainful activity if you are self-employed. We will not consider your income alone because the amount of income you actually receive may depend on a number of different factors, such as capital investment and profit-sharing agreements. We will generally consider work that you were forced to stop or reduce to below substantial gainful activity after 6 months or less because of your impairment as an unsuccessful work attempt. See paragraph (d) of this section. We will evaluate your work activity based on the value of your services to the business regardless of whether you receive an immediate income for your services. We determine whether you have engaged in substantial gainful activity by applying three tests. If you have not engaged in substantial gainful activity under test one, then we will consider tests two and three. The tests are as follows:
(i) Test one: You have engaged in substantial gainful activity if you render services that are significant to the operation of the business and receive a substantial income from the business. Paragraphs (b) and (c) of this section explain what we mean by significant services and substantial income for purposes of this test.
(ii) Test Two: You have engaged in substantial gainful activity if your work activity, in terms of factors such as hours, skills, energy output, efficiency, duties, and responsibilities, is comparable to that of unimpaired individuals in your community who are in the same or similar businesses as their means of livelihood.
(iii) Test Three: You have engaged in substantial gainful activity if your work activity, although not comparable to that of unimpaired individuals, is clearly worth the amount shown in § 404.1574(b)(2) when considered in terms of its value to the business, or when compared to the salary that an owner would pay to an employee to do the work you are doing.
(b) What we mean by significant services.
(1) If you are not a farm landlord and you operate a business entirely by yourself, any services that you render are significant to the business. If your business involves the services of more than one person, we will consider you to be rendering significant services if you contribute more than half the total time required for the management of the business, or you render management services for more than 45 hours a month regardless of the total management time required by the business.
(2) If you are a farm landlord, that is, you rent farm land to another, we will consider you to be rendering significant services if you materially participate in the production or the management of the production of the things raised on the rented farm. (See § 404.1082 of this chapter for an explanation of material participation.) If you were given social security earnings credits because you materially participated in the activities of the farm and you continue these same activities, we will consider you to be rendering significant services.
(c) What we mean by substantial income —
(1) Determining countable income. We deduct your normal business expenses from your gross income to determine net income. Once we determine your net income, we deduct the reasonable value of any significant amount of unpaid help furnished by your spouse, children, or others. Miscellaneous duties that ordinarily would not have commercial value would not be considered significant. We deduct impairment-related work expenses that have not already been deducted in determining your net income. Impairment-related work expenses are explained in § 404.1576. We deduct unincurred business expenses paid for you by another individual or agency. An unincurred business expense occurs when a sponsoring agency or another person incurs responsibility for the payment of certain business expenses, e.g., rent, utilities, or purchases and repair of equipment, or provides you with equipment, stock, or other material for the operation of your business. We deduct soil bank payments if they were included as farm income. That part of your income remaining after we have made all applicable deductions represents the actual value of work performed. The resulting amount is the amount we use to determine if you have done substantial gainful activity. For purposes of this section, we refer to this amount as your countable income. We will generally average your countable income for comparison with the earnings guidelines in § 404.1574(b)(2). See § 404.1574a for our rules on averaging of earnings.
(2) When countable income is considered substantial. We will consider your countable income to be substantial if—
(i) It averages more than the amounts described in § 404.1574(b)(2); or
(ii) It averages less than the amounts described in § 404.1574(b)(2) but it is either comparable to what it was before you became seriously impaired if we had not considered your earnings or is comparable to that of unimpaired self-employed persons in your community who are in the same or a similar business as their means of livelihood.
(d) The unsuccessful work attempt —
(1) General. Ordinarily, work you have done will not show that you are able to do substantial gainful activity if, after working for a period of 6 months or less, you were forced by your impairment to stop working or to reduce the amount of work you do so that you are no longer performing substantial gainful activity and you meet the conditions described in paragraphs (d)(2), (3), and (4) of this section. We will use the provisions of this paragraph when we make an initial determination on your application for disability benefits and throughout any appeal you may request. Except as set forth in § 404.1592a(a), we will also apply the provisions of this paragraph if you are already entitled to disability benefits, when you work and we consider whether the work you are doing is substantial gainful activity or demonstrates the ability to do substantial gainful activity.
(2) Event that must precede an unsuccessful work attempt. There must be a significant break in the continuity of your work before we will consider you to have begun a work attempt that later proved unsuccessful. You must have stopped working or reduced your work and earnings below substantial gainful activity because of your impairment or because of the removal of special conditions which took into account your impairment and permitted you to work. Examples of such special conditions may include any significant amount of unpaid help furnished by your spouse, children, or others, or unincurred business expenses, as described in paragraph (c) of this section, paid for you by another individual or agency. We will consider your prior work to be “discontinued” for a significant period if you were out of work at least 30 consecutive days. We will also consider your prior work to be “discontinued” if, because of your impairment, you were forced to change to another type of work.
(3) If you worked 6 months or less. We will consider work of 6 months or less to be an unsuccessful work attempt if you stopped working or you reduced your work and earnings below the substantial gainful activity earnings level because of your impairment or because of the removal of special conditions that took into account your impairment and permitted you to work.
(4) If you worked more than 6 months. We will not consider work you performed at the substantial gainful activity level for more than 6 months to be an unsuccessful work attempt regardless of why it ended or was reduced below the substantial gainful activity earnings level.
(e) Special rules for evaluating the work you do after you have received social security disability benefits for at least 24 months —
(1) General. We will apply the provisions of this paragraph to evaluate the work you are doing or have done if, at the time you do the work, you are entitled to social security disability benefits and you have received such benefits for at least 24 months. We will apply the provisions of this paragraph only when we are evaluating that work to consider whether you have engaged in substantial gainful activity or demonstrated the ability to engage in substantial gainful activity for the purpose of determining whether your disability has ceased because of your work activity (see §§ 404.1592a(a)(1) and (3)(ii) and 404.1594(d)(5) and (f)(1)). We will use the countable income test described in paragraph (e)(3) of this section to determine whether the work you do after you have received such benefits for at least 24 months is substantial gainful activity or demonstrates the ability to do substantial gainful activity. We will not consider the services you perform in that work to determine that the work you are doing shows that you are able to engage in substantial gainful activity and are, therefore, no longer disabled. However, we may consider the services you perform to determine that you are not doing substantial gainful activity. We will generally consider work that you were forced to stop or reduce below substantial gainful activity after 6 months or less because of your impairment as an unsuccessful work attempt. See paragraph (d) of this section.
(2) The 24-month requirement. For purposes of paragraphs (a)(1) and (e) of this section, we consider you to have received social security disability benefits for at least 24 months beginning with the first day of the first month following the 24th month for which you actually received social security disability benefits that you were due or constructively received such benefits. The 24 months do not have to be consecutive. We will consider you to have constructively received a benefit for a month for purposes of the 24-month requirement if you were otherwise due a social security disability benefit for that month and your monthly benefit was withheld to recover an overpayment. Any months for which you were entitled to benefits but for which you did not actually or constructively receive a benefit payment will not be counted for the 24-month requirement. If you also receive supplemental security income payments based on disability or blindness under title XVI of the Social Security Act, months for which you received only supplemental security income payments will not be counted for the 24-month requirement.
(3) Countable income test. We will compare your countable income to the earnings guidelines in § 404.1574(b)(2) to determine if you have engaged in substantial gainful activity. See paragraph (c)(1) of this section for an explanation of countable income. We will consider that you have engaged in substantial gainful activity if your monthly countable income averages more than the amounts described in § 404.1574(b)(2) for the month(s) in which you work, unless the evidence shows that you did not render significant services in the month(s). See paragraph (b) of this section for what we mean by significant services. If your average monthly countable income is equal to or less than the amounts in § 404.1574(b)(2) for the month(s) in which you work, or if the evidence shows that you did not render significant services in the month(s), we will consider that your work as a self-employed person shows that you have not engaged in substantial gainful activity.
[46 FR 4870, Jan. 19, 1981, as amended at 48 FR 21936, May 16, 1983; 49 FR 22272, May 29, 1984; 65 FR 42785, July 11, 2000; 71 FR 66854, Nov. 17, 2006; 81 FR 71369, Oct. 17, 2016]
§ 404.1576 Impairment-related work expenses.
(a) General. When we figure your earnings in deciding if you have done substantial gainful activity, we will subtract the reasonable costs to you of certain items and services which, because of your impairment(s), you need and use to enable you to work. The costs are deductible even though you also need or use the items and services to carry out daily living functions unrelated to your work. Paragraph (b) of this section explains the conditions for deducting work expenses. Paragraph (c) of this section describes the expenses we will deduct. Paragraph (d) of this section explains when expenses may be deducted. Paragraph (e) of this section describes how expenses may be allocated. Paragraph (f) of this section explains the limitations on deducting expenses. Paragraph (g) of this section explains our verification procedures.
(b) Conditions for deducting impairment-related work expenses. We will deduct impairment-related work expenses if—
(1) You are otherwise disabled as defined in §§ 404.1505, 404.1577 and 404.1581-404.1583;
(2) The severity of your impairment(s) requires you to purchase (or rent) certain items and services in order to work;
(3) You pay the cost of the item or service. No deduction will be allowed to the extent that payment has been or will be made by another source. No deduction will be allowed to the extent that you have been, could be, or will be reimbursed for such cost by any other source (such as through a private insurance plan, Medicare or Medicaid, or other plan or agency). For example, if you purchase crutches for $80 but you were, could be, or will be reimbursed $64 by some agency, plan, or program, we will deduct only $16;
(4) You pay for the item or service in a month you are working (in accordance with paragraph (d) of this section); and
(5) Your payment is in cash (including checks or other forms of money). Payment in kind is not deductible.
(c) What expenses may be deducted —
(1) Payments for attendant care services.
(i) If because of your impairment(s) you need assistance in traveling to and from work, or while at work you need assistance with personal functions (e.g., eating, toileting) or with work-related functions (e.g., reading, communicating), the payments you make for those services may be deducted.
(ii) If because of your impairment(s) you need assistance with personal functions (e.g., dressing, administering medications) at home in preparation for going to and assistance in returning from work, the payments you make for those services may be deducted.
(iii)
(A) We will deduct payments you make to a family member for attendant care services only if such person, in order to perform the services, suffers an economic loss by terminating his or her employment or by reducing the number of hours he or she worked.
(B) We consider a family member to be anyone who is related to you by blood, marriage or adoption, whether or not that person lives with you.
(iv) If only part of your payment to a person is for services that come under the provisions of paragraph (c)(1) of this section, we will only deduct that part of the payment which is attributable to those services. For example, an attendant gets you ready for work and helps you in returning from work, which takes about 2 hours a day. The rest of his or her 8 hour day is spent cleaning your house and doing your laundry, etc. We would only deduct one-fourth of the attendant's daily wages as an impairment-related work expense.
(2) Payments for medical devices. If your impairment(s) requires that you utilize medical devices in order to work, the payments you make for those devices may be deducted. As used in this subparagraph, medical devices include durable medical equipment which can withstand repeated use, is customarily used for medical purposes, and is generally not useful to a person in the absence of an illness or injury. Examples of durable medical equipment are wheelchairs, hemodialysis equipment, canes, crutches, inhalators and pacemakers.
(3) Payments for prosthetic devices. If your impairment(s) requires that you utilize a prosthetic device in order to work, the payments you make for that device may be deducted. A prosthetic device is that which replaces an internal body organ or external body part. Examples of prosthetic devices are artificial replacements of arms, legs and other parts of the body.
(4) Payments for equipment.
(i) Work-related equipment. If your impairment(s) requires that you utilize special equipment in order to do your job, the payments you make for that equipment may be deducted. Examples of work-related equipment are one-hand typewriters, vision aids, sensory aids for the blind, telecommunication devices for the deaf and tools specifically designed to accommodate a person's impairment(s).
(ii) Residential modifications. If your impairment(s) requires that you make modifications to your residence, the location of your place of work will determine if the cost of these modifications will be deducted. If you are employed away from home, only the cost of changes made outside of your home to permit you to get to your means of transportation (e.g., the installation of an exterior ramp for a wheelchair confined person or special exterior railings or pathways for someone who requires crutches) will be deducted. Costs relating to modifications of the inside of your home will not be deducted. If you work at home, the costs of modifying the inside of your home in order to create a working space to accommodate your impairment(s) will be deducted to the extent that the changes pertain specifically to the space in which you work. Examples of such changes are the enlargement of a doorway leading into the workspace or modification of the workspace to accommodate problems in dexterity. However, if you are self-employed at home, any cost deducted as a business expense cannot be deducted as an impairment-related work expense.
(iii) Nonmedical appliances and equipment. Expenses for appliances and equipment which you do not ordinarily use for medical purposes are generally not deductible. Examples of these items are portable room heaters, air conditioners, humidifiers, dehumidifiers, and electric air cleaners. However, expenses for such items may be deductible when unusual circumstances clearly establish an impairment-related and medically verified need for such an item because it is essential for the control of your disabling condition, thus enabling you to work. To be considered essential, the item must be of such a nature that if it were not available to you there would be an immediate adverse impact on your ability to function in your work activity. In this situation, the expense is deductible whether the item is used at home or in the working place. An example would be the need for an electric air cleaner by an individual with severe respiratory disease who cannot function in a non-purified air environment. An item such as an exercycle is not deductible if used for general physical fitness. If it is prescribed and used as necessary treatment of your impairment and necessary to enable you to work, we will deduct payments you make toward its cost.
(5) Payments for drugs and medical services.
(i) If you must use drugs or medical services (including diagnostic procedures) to control your impairment(s) the payments you make for them may be deducted. The drugs or services must be prescribed (or utilized) to reduce or eliminate symptoms of your impairment(s) or to slow down its progression. The diagnostic procedures must be performed to ascertain how the impairment(s) is progressing or to determine what type of treatment should be provided for the impairment(s).
(ii) Examples of deductible drugs and medical services are anticonvulsant drugs to control epilepsy or anticonvulsant blood level monitoring; antidepressant medication for mental disorders; medication used to allay the side effects of certain treatments; radiation treatment or chemotherapy for cancer patients; corrective surgery for spinal disorders; electroencephalograms and brain scans related to a disabling epileptic condition; tests to determine the efficacy of medication on a diabetic condition; and immunosuppressive medications that kidney transplant patients regularly take to protect against graft rejection.
(iii) We will only deduct the costs of drugs or services that are directly related to your impairment(s). Examples of non-deductible items are routine annual physical examinations, optician services (unrelated to a disabling visual impairment) and dental examinations.
(6) Payments for similar items and services —
(i) General. If you are required to utilize items and services not specified in paragraphs (c) (1) through (5) of this section but which are directly related to your impairment(s) and which you need to work, their costs are deductible. Examples of such items and services are medical supplies and services not discussed above, the purchase and maintenance of a dog guide which you need to work, and transportation.
(ii) Medical supplies and services not described above. We will deduct payments you make for expendable medical supplies, such as incontinence pads, catheters, bandages, elastic stockings, face masks, irrigating kits, and disposable sheets and bags. We will also deduct payments you make for physical therapy which you require because of your impairment(s) and which you need in order to work.
(iii) Payments for transportation costs. We will deduct transportation costs in these situations:
(A) Your impairment(s) requires that in order to get to work you need a vehicle that has structural or operational modifications. The modifications must be critical to your operation or use of the vehicle and directly related to your impairment(s). We will deduct the costs of the modifications, but not the cost of the vehicle. We will also deduct a mileage allowance for the trip to and from work. The allowance will be based on data compiled by the Federal Highway Administration relating to vehicle operating costs.
(B) Your impairment(s) requires you to use driver assistance, taxicabs or other hired vehicles in order to work. We will deduct amounts paid to the driver and, if your own vehicle is used, we will also deduct a mileage allowance, as provided in paragraph (c)(6)(iii)(A) of this section, for the trip to and from work.
(C) Your impairment(s) prevents your taking available public transportation to and from work and you must drive your (unmodified) vehicle to work. If we can verify through your physician or other sources that the need to drive is caused by your impairment(s) (and not due to the unavailability of public transportation), we will deduct a mileage allowance, as provided in paragraph (c)(6)(iii)(A) of this section, for the trip to and from work.
(7) Payments for installing, maintaining, and repairing deductible items. If the device, equipment, appliance, etc., that you utilize qualifies as a deductible item as described in paragraphs (c) (2), (3), (4) and (6) of this section, the costs directly related to installing, maintaining and repairing these items are also deductible. (The costs which are associated with modifications to a vehicle are deductible. Except for a mileage allowance, as provided for in paragraph (c)(6)(iii) of this section, the costs which are associated with the vehicle itself are not deductible.)
(d) When expenses may be deducted —
(1) Effective date. To be deductible an expense must be incurred after November 30, 1980. An expense may be considered incurred after that date if it is paid thereafter even though pursuant to a contract or other arrangement entered into before December 1, 1980.
(2) Payments for services. A payment you make for services may be deducted if the services are received while you are working and the payment is made in a month you are working. We consider you to be working even though you must leave work temporarily to receive the services.
(3) Payments for items. A payment you make toward the cost of a deductible item (regardless of when it is acquired) may be deducted if payment is made in a month you are working. See paragraph (e)(4) of this section when purchases are made in anticipation of work.
(e) How expenses are allocated —
(1) Recurring expenses. You may pay for services on a regular periodic basis, or you may purchase an item on credit and pay for it in regular periodic installments or you may rent an item. If so, each payment you make for the services and each payment you make toward the purchase or rental (including interest) is deductible in the month it is made.
Example:
B starts work in October 1981 at which time she purchases a medical device at a cost of $4,800 plus interest charges of $720. Her monthly payments begin in October. She earns and receives $400 a month. The term of the installment contract is 48 months. No downpayment is made. The monthly allowable deduction for the item would be $115 ($5520 divided by 48) for each month of work during the 48 months.
(2) Nonrecurring expenses. Part or all of your expenses may not be recurring. For example, you may make a one-time payment in full for an item or service or make a downpayment. If you are working when you make the payment we will either deduct the entire amount in the month you pay it or allocate the amount over a 12 consecutive month period beginning with the month of payment, whichever you select.
Example:
A begins working in October 1981 and earns $525 a month. In the same month he purchases and pays for a deductible item at a cost of $250. In this situation we could allow a $250 deduction for October 1981, reducing A's earnings below the SGA level for that month.
If A's earnings had been $15 above the SGA earnings amount, A probably would select the option of projecting the $250 payment over the 12-month period, October 1981-September 1982, giving A an allowable deduction of $20.83 a month for each month of work during that period. This deduction would reduce A's earnings below the SGA level for 12 months.
(3) Allocating downpayments. If you make a downpayment we will, if you choose, make a separate calculation for the downpayment in order to provide for uniform monthly deductions. In these situations we will determine the total payment that you will make over a 12 consecutive month period beginning with the month of the downpayment and allocate that amount over the 12 months. Beginning with the 13th month, the regular monthly payment will be deductible. This allocation process will be for a shorter period if your regular monthly payments will extend over a period of less than 12 months.
Example 1.
C starts working in October 1981, at which time he purchases special equipment at a cost of $4,800, paying $1,200 down. The balance of $3,600, plus interest of $540, is to be repaid in 36 installments of $115 a month beginning November 1981. C earns $500 a month. He chooses to have the downpayment allocated. In this situation we would allow a deduction of $205.42 a month for each month of work during the period October 1981 through September 1982. After September 1982, the deduction amount would be the regular monthly payment of $115 for each month of work during the remaining installment period.
| Explanation: | ||
| Downpayment in 10/81 | $1,200 | |
| Monthly payments 11/81 through 09/82 | 1,265 | |
| 12) 2,465 | = $205.42 |
Example 2.
D, while working, buys a deductible item in July 1981, paying $1,450 down. However, his first monthly payment of $125 is not due until September 1981. D chooses to have the downpayment allocated. In this situation we would allow a deduction of $225 a month for each month of work during the period July 1981 through June 1982. After June 1982, the deduction amount would be the regular monthly payment of $125 for each month of work.
| Explanation: | ||
| Downpayment in 07/81 | $1,450 | |
| Monthly payments 09/81 through 06/82 | 1,250 | |
| 12) 2,700 | = $225 |
(4) Payments made in anticipation of work. A payment toward the cost of a deductible item that you made in any of the 11 months preceding the month you started working will be taken into account in determining your impairment-related work expenses. When an item is paid for in full during the 11 months preceding the month you started working the payment will be allocated over the 12-consecutive month period beginning with the month of the payment. However, the only portion of the payment which may be deductible is the portion allocated to the month work begins and the following months. For example, if an item is purchased 3 months before the month work began and is paid for with a one-time payment of $600, the deductible amount would be $450 ($600 divided by 12, multiplied by 9). Installment payments (including a downpayment) that you made for a particular item during the 11 months preceding the month you started working will be totaled and considered to have been made in the month of your first payment for that item within this 11 month period. The sum of these payments will be allocated over the 12-consecutive month period beginning with the month of your first payment (but never earlier than 11 months before the month work began). However, the only portion of the total which may be deductible is the portion allocated to the month work begins and the following months. For example, if an item is purchased 3 months before the month work began and is paid for in 3 monthly installments of $200 each, the total payment of $600 will be considered to have been made in the month of the first payment, that is, 3 months before the month work began. The deductible amount would be $450 ($600 divided by 12, multiplied by 9). The amount, as determined by these formulas, will then be considered to have been paid in the first month of work. We will deduct either this entire amount in the first month of work or allocate it over a 12-consecutive month period beginning with the first month of work, whichever you select. In the above examples, the individual would have the choice of having the entire $450 deducted in the first month of work or of having $37.50 a month ($450 divided by 12) deducted for each month that he works over a 12-consecutive month period, beginning with the first month of work. To be deductible the payments must be for durable items such as medical devices, prostheses, work-related equipment, residential modifications, nonmedical appliances and vehicle modifications. Payments for services and expendable items such as drugs, oxygen, diagnostic procedures, medical supplies and vehicle operating costs are not deductible for purposes of this paragraph.
(f) Limits on deductions.
(1) We will deduct the actual amounts you pay towards your impairment-related work expenses unless the amounts are unreasonable. With respect to durable medical equipment, prosthetic devices, medical services, and similar medically-related items and services, we will apply the prevailing charges under Medicare (part B of title XVIII, Health Insurance for the Aged and Disabled) to the extent that this information is readily available. Where the Medicare guides are used, we will consider the amount that you pay to be reasonable if it is no more than the prevailing charge for the same item or service under the Medicare guidelines. If the amount you actually pay is more than the prevailing charge for the same item under the Medicare guidelines, we will deduct from your earnings the amount you paid to the extent you establish that the amount is consistent with the standard or normal charge for the same or similar item or service in your community. For items and services that are not listed in the Medicare guidelines, and for items and services that are listed in the Medicare guidelines but for which such guides cannot be used because the information is not readily available, we will consider the amount you pay to be reasonable if it does not exceed the standard or normal charge for the same or similar item(s) or service(s) in your community.
(2) Impairment-related work expenses are not deducted in computing your earnings for purposes of determining whether your work was “services” as described in § 404.1592(b).
(3) The decision as to whether you performed substantial gainful activity in a case involving impairment-related work expenses for items or services necessary for you to work generally will be based upon your “earnings” and not on the value of “services” you rendered. (See §§ 404.1574(b)(6) (i) and (ii), and 404.1575(a)). This is not necessarily so, however, if you are in a position to control or manipulate your earnings.
(4) The amount of the expenses to be deducted must be determined in a uniform manner in both the disability insurance and SSI programs.
(5) No deduction will be allowed to the extent that any other source has paid or will pay for an item or service. No deduction will be allowed to the extent that you have been, could be, or will be, reimbursed for payments you made. (See paragraph (b)(3) of this section.)
(6) The provisions described in the foregoing paragraphs of this section are effective with respect to expenses incurred on and after December 1, 1980, although expenses incurred after November 1980 as a result of contractual or other arrangements entered into before December 1980, are deductible. For months before December 1980 we will deduct impairment-related work expenses from your earnings only to the extent they exceeded the normal work-related expenses you would have had if you did not have your impairment(s). We will not deduct expenses, however, for those things which you needed even when you were not working.
(g) Verification. We will verify your need for items or services for which deductions are claimed, and the amount of the charges for those items or services. You will also be asked to provide proof that you paid for the items or services.
[48 FR 21936, May 16, 1983]
Widows, Widowers, and Surviving Divorced Spouses
§ 404.1577 Disability defined for widows, widowers, and surviving divorced spouses for monthly benefits payable for months prior to January 1991.
For monthly benefits payable for months prior to January 1991, the law provides that to be entitled to a widow's or widower's benefit as a disabled widow, widower, or surviving divorced spouse, you must have a medically determinable physical or mental impairment which can be expected to result in death or has lasted or can be expected to last for a continuous period of not less than 12 months. The impairment(s) must have been of a level of severity to prevent a person from doing any gainful activity. To determine whether you were disabled, we consider only your physical or mental impairment(s). We do not consider your age, education, and work experience. We also do not consider certain felony-related and prison-related impairments, as explained in § 404.1506. (For monthly benefits payable for months after December 1990, see § 404.1505(a).)
[57 FR 30120, July 8, 1992]
§ 404.1578 How we determine disability for widows, widowers, and surviving divorced spouses for monthly benefits payable for months prior to January 1991.
(a) For monthly benefits payable for months prior to January 1991, we will find that you were disabled and pay you widow's or widower's benefits as a widow, widower, or surviving divorced spouse if—
(1) Your impairment(s) had specific clinical findings that were the same as those for any impairment in the Listing of Impairments in appendix 1 of this subpart or were medically equivalent to those for any impairment shown there;
(2) Your impairment(s) met the duration requirement.
(b) However, even if you met the requirements in paragraphs (a) (1) and (2) of this section, we will not find you disabled if you were doing substantial gainful activity.
[57 FR 30121, July 8, 1992]
§ 404.1579 How we will determine whether your disability continues or ends.
(a) General.
(1) The rules for determining whether disability continues for widow's or widower's monthly benefits for months after December 1990 are discussed in §§ 404.1594 through 404.1598. The rules for determining whether disability continues for monthly benefits for months prior to January 1991 are discussed in paragraph (a)(2) of this section and paragraphs (b) through (h) of this section.
(2) If you are entitled to disability benefits as a disabled widow, widower, or surviving divorced spouse, and we must decide whether your disability continued or ended for monthly benefits for months prior to January 1991, there are a number of factors we consider in deciding whether your disability continued. We must determine if there has been any medical improvement in your impairment(s) and, if so, whether this medical improvement is related to your ability to work. If your impairment(s) has not so medically improved, we must address whether one or more exceptions applies. If medical improvement related to your ability to work has not occurred and no exception applies, your benefits will continue. Even where medical improvement related to your ability to work has occurred or an exception applies, in most cases (see paragraph (e) of this section for exceptions) before we can find that you are no longer disabled, we must also show that your impairment(s), as shown by current medical evidence, is no longer deemed, under appendix 1 of this subpart, sufficient to preclude you from engaging in gainful activity.
(b) Terms and definitions. There are several terms and definitions which are important to know in order to understand how we review your claim to determine whether your disability continues.
(1) Medical improvement. Medical improvement is any decrease in the medical severity of your impairment(s) which was present at the time of the most recent favorable medical decision that you were disabled or continued to be disabled. A determination that there has been a decrease in medical severity must be based on improvement in the symptoms, signs, and/or laboratory findings associated with your impairment(s).
Example 1:
You were awarded disability benefits due to a herniated nucleus pulposus which was determined to equal the level of severity contemplated by Listing 1.05.C. At the time of our prior favorable decision, you had had a laminectomy. Postoperatively, a myelogram still showed evidence of a persistent deficit in your lumbar spine. You had pain in your back, and pain and a burning sensation in your right foot and leg. There were no muscle weakness or neurological changes and a modest decrease in motion in your back and leg. When we reviewed your claim your treating physician reported that he had seen you regularly every 2 to 3 months for the past 2 years. No further myelograms had been done, complaints of pain in the back and right leg continued especially on sitting or standing for more than a short period of time. Your doctor further reported a moderately decreased range of motion in your back and right leg, but again no muscle atrophy or neurological changes were reported. Medical improvement has not occurred because there has been no decrease in the severity of your back impairment as shown by changes in symptoms, signs, or laboratory findings.
Example 2:
You were awarded disability benefits due to rheumatoid arthritis of a severity as described in Listing 1.02 of appendix 1 of this subpart. At the time, laboratory findings were positive for this condition. Your doctor reported persistent swelling and tenderness of your fingers and wrists and that you complained of joint pain. Current medical evidence shows that while laboratory tests are still positive for rheumatoid arthritis, your impairment has responded favorably to therapy so that for the last year your fingers and wrists have not been significantly swollen or painful. Medical improvement has occurred because there has been a decrease in the severity of your impairment as documented by the current symptoms and signs reported by your physician. Although your impairment is subject to temporary remissions and exacerbations the improvement that has occurred has been sustained long enough to permit a finding of medical improvement. We would then determine if this medical improvement is related to your ability to work.
(2) Determining whether medical improvement is related to your ability to work. If medical improvement has occurred and the severity of the prior impairment(s) no longer meets or equals the listing section which was used in making our most recent favorable decision, we will find that the medical improvement was related to your ability to work. We make this finding because the criteria in appendix 1 of this subpart are related to ability to work because they reflect impairments which are considered severe enough to prevent a person from doing any gainful work. We must, of course, also establish that, considering all of your current impairments not just those which existed at the time of the most recent prior favorable medical decision, your condition does not meet or equal the requirements of appendix 1 before we could find that your disability has ended. If there has been any medical improvement in your impairment(s), but it is not related to your ability to do work and none of the exceptions applies, your benefits will be continued.
(3) Determining whether your impairment(s) is deemed, under appendix 1 of this subpart, sufficient to preclude you from engaging in gainful activity. Even where medical improvement related to your ability to work has occurred or an exception applies, in most cases before we can find that you are no longer disabled, we must also show that your impairment(s) is no longer deemed, under appendix 1 of this subpart, sufficient to preclude you from engaging in gainful activity. All current impairments will be considered, not just the impairment(s) present at the time of our most recent favorable determination. Sections 404.1525, 404.1526, and 404.1578 set out how we will decide whether your impairment(s) meets or equals the requirements of appendix 1 of this subpart.
(4) Evidence and basis for our decision. Our decisions under this section will be made on a neutral basis without any initial inference as to the presence or absence of disability being drawn from the fact that you have previously been determined to be disabled. We will consider all evidence you submit and that we obtain from your medical sources and nonmedical sources. What constitutes “evidence” and our procedures for obtaining it are set out in §§ 404.1512 through 404.1518. Our determination regarding whether your disability continues will be made on the basis of the weight of the evidence.
(5) Point of comparison. For purposes of determining whether medical improvement has occurred, we will compare the current severity of that impairment(s) which was present at the time of the most recent favorable medical decision that you were disabled or continued to be disabled to the medical severity of that impairment(s) at that time. If medical improvement has occurred, we will determine whether the medical improvement is related to your ability to do work based on this previously existing impairment(s). The most recent favorable medical decision is the latest decision involving a consideration of the medical evidence and the issue of whether you were disabled or continued to be disabled which became final.
(c) Determining medical improvement and its relationship to your ability to do work. Paragraphs (b) (1) and (2) of this section discuss what we mean by medical improvement and how we determine whether medical improvement is related to your ability to work.
(1) Medical improvement. Medical improvement is any decrease in the medical severity of impairment(s) present at the time of the most recent favorable medical decision that you were disabled or continued to be disabled. Whether medical improvement has occurred is determined by a comparison of prior and current medical evidence which must show that there have been changes (improvement) in the symptoms, signs or laboratory findings associated with that impairment(s).
(2) Determining whether medical improvement is related to ability to work. If there is a decrease in medical severity as shown by the signs, symptoms and laboratory findings, we then must determine if it is related to your ability to do work, as explained in paragraph (b)(2) of this section. In determining if the medical improvement that has occurred is related to your ability to work, we will assess whether the previously existing impairments still meet or equal the level of severity contemplated by the same listing section in appendix 1 of this subpart which was used in making our most recent favorable decision. Appendix 1 of this subpart describes impairments which, if severe enough, affect a person's ability to work. If the appendix level of severity is met or equaled, the individual is deemed, in the absence of evidence of the contrary, to be unable to engage in gainful activity. If there has been medical improvement to the degree that the requirement of the listing section is no longer met or equaled, then the medical improvement is related to your ability to work. Unless an objective assessment shows that the listing requirement is no longer met or equaled based on actual changes shown by the medical evidence, the medical improvement that has occurred will not be considered to be related to your ability to work.
(3) Prior file cannot be located. If the prior file cannot be located, we will first determine whether your current impairment(s) is deemed, under appendix 1 of this subpart, sufficient to preclude you from engaging in gainful activity. (In this way, we will be able to determine that your disability continues at the earliest time without addressing the issue of reconstructing prior evidence which can be a lengthy process.) If so, your benefits will continue unless one of the second group of exceptions applies (see paragraph (e) of this section). If not, we will determine whether an attempt should be made to reconstruct those portions of the file that were relevant to our most recent favorable medical decision (e.g., medical evidence from treating sources and the results of consultative examinations). This determination will consider the potential availability of old records in light of their age, whether the source of the evidence is still in operation, etc.; and whether reconstruction efforts will yield a complete record of the basis for the most recent favorable medical decision. If relevant parts of the prior record are not reconstructed either because it is determined not to attempt reconstruction or because such efforts fail, medical improvement cannot be found. The documentation of your current impairments will provide a basis for any future reviews. If the missing file is later found, it may serve as a basis for reopening any decision under this section in accordance with the rules in § 404.988.
(4) Impairment(s) subject to temporary remission. In some cases the evidence shows that an individual's impairment is subject to temporary remission. In assessing whether medical improvement has occurred in persons with this type of impairment, we will be careful to consider the longitudinal history of the impairment(s), including the occurrence of prior remissions, and prospects for future worsening of the impairment(s). Improvement in such impairments that is only temporary will not warrant a finding of medical improvement.
(5) Applicable listing has been revised since the most recent favorable medical decision. When determining whether any medical improvement is related to your ability to work, we use the same listing section in appendix 1 of this subpart which was used to make our prior favorable decision. We will use the listing as it appeared at the time of the prior decision, even where the requirement(s) of the listing was subsequently changed. The current revised listing requirement will be used if we determine that you have medically improved and it is necessary to determine whether you are now considered unable to engage in gainful activity.
(d) First group of exceptions to medical improvement. The law provides for certain limited situations when your disability can be found to have ended even though medical improvement has not occurred, if your impairment(s) is no longer considered, under appendix 1 of this subpart, sufficient to preclude you from engaging in gainful activity. These exceptions to medical improvement are intended to provide a way of finding that a person is no longer disabled in those limited situations where, even though there has been no decrease in severity of the impairment(s), evidence shows that the person should no longer be considered disabled or never should have been considered disabled. If one of these exceptions applies, before we can find you are no longer disabled, we must also show that, taking all your current impairment(s) into account, not just those that existed at the time of our most recent favorable medical decision, your impairment(s) is no longer deemed, under appendix 1 of this subpart, sufficient to preclude you from engaging in gainful activity. As part of the review process, you will be asked about any medical therapy you received or are receiving. Your answers and the evidence gathered as a result as well as all other evidence, will serve as the basis for the finding that an exception does or does not apply.
(1) Substantial evidence shows that you are the beneficiary of advances in medical therapy or technology (related to your ability to work). Advances in medical therapy or technology are improvements in treatment or rehabilitative methods which have favorably affected the severity of your impairment(s). We will apply this exception when substantial evidence shows that you have been the beneficiary of services which reflect these advances and they have favorably affected the severity of your impairment(s). This decision will be based on new medical evidence. In many instances, an advanced medical therapy or technology will result in a decrease in severity as shown by symptoms, signs and laboratory findings which will meet the definition of medical improvement. This exception will, therefore, see very limited application.
(2) Substantial evidence shows that based on new or improved diagnostic or evaluative techniques your impairment(s) is not as disabling as it was considered to be at the time of the most recent favorable decision. Changing methodologies and advances in medical and other diagnostic or evaluative techniques have given, and will continue to give, rise to improved methods for measuring and documenting the effect of various impairments on the ability to do work. Where, by such new or improved methods, substantial evidence shows that your impairment(s) is not as severe as was determined at the time of our most recent favorable medical decision, such evidence may serve as a basis for finding that you are no longer disabled, if your impairment(s) is no longer deemed, under appendix 1 of this subpart, sufficient to preclude you from engaging in gainful activity. In order to be used under this exception, however, the new or improved techniques must have become generally available after the date of our most recent favorable medical decision.
(i) How we will determine which methods are new or improved techniques and when they become generally available. New or improved diagnostic techniques or evaluations will come to our attention by several methods. In reviewing cases, we often become aware of new techniques when their results are presented as evidence. Such techniques and evaluations are also discussed and acknowledged in medical literature by medical professional groups and other governmental entities. Through these sources, we develop listings of new techniques and when they become generally available. For example, we will consult the Health Care Financing Administration for its experience regarding when a technique is recognized for payment under Medicare and when they began paying for the technique.
(ii) How you will know which methods are new or improved techniques and when they become generally available. We will let you know which methods we consider to be new or improved techniques and when they become available through two vehicles.
(A) Some of the future changes in the Listing of Impairments in appendix 1 of this subpart will be based on new or improved diagnostic or evaluative techniques. Such listing changes will clearly state this fact as they are published as Notices of Proposed Rulemaking and the new or improved technique will be considered generally available as of the date of the final publication of that particular listing in the Federal Register.
(B) A cumulative list since 1970 of new or improved diagnostic techniques or evaluations, how they changed the evaluation of the applicable impairment and the month and year they became generally available, will be published in the Notices section of the Federal Register. Included will be any changes in the Listing of Impairments published in the Code of Federal Regulations since 1970 which are reflective of new or improved techniques. No cases will be processed under this exception until this cumulative listing is so published. Subsequent changes to the list will be published periodically. The period will be determined by the volume of changes needed.
Example:
The electrocardiographic exercise test has replaced the Master's 2-step test as a measurement of heart function since the time of your last favorable medical decision. Current evidence could show that your condition, which was previously evaluated based on the Master's 2-step test, is not now as disabling as was previously thought. If, taking all your current impairments into account, you are now able to engage in gainful activity, this exception would be used to find that you are no longer disabled even if medical improvement has not occurred.
(3) Substantial evidence demonstrates that any prior disability decision was in error. We will apply the exception to medical improvement based on error if substantial evidence (which may be evidence on the record at the time any prior determination of the entitlement to benefits based on disability was made, or newly obtained evidence which relates to that determination) demonstrates that a prior determination was in error. A prior determination will be found in error only if:
(i) Substantial evidence shows on its face that the decision in question should not have been made (e.g., the evidence in your file such as pulmonary function study values was misread or an adjudicative standard such as a listing in appendix 1 of this subpart was misapplied).
Example:
You were granted benefits when it was determined that your epilepsy met Listing 11.02. This listing calls for a finding of major motor seizures more frequently than once a month as documented by EEG evidence and by a detailed description of a typical seizure pattern. A history of either diurnal episodes or nocturnal episodes with residuals interfering with daily activities is also required. On review, it is found that a history of the frequency of your seizures showed that they occurred only once or twice a year. The prior decision would be found to be in error, and whether you were still considered to be disabled would be based on whether your current impairment(s) meets or equals the requirements of appendix 1 of this subpart.
(ii) At the time of the prior evaluation, required and material evidence of the severity of your impairment(s) was missing. That evidence becomes available upon review, and substantial evidence demonstrates that had such evidence been present at the time of the prior determination, disability would not have been found.
(iii) Substantial evidence which is new evidence which relates to the prior determination (of allowance or continuance) refutes the conclusions that were based upon the prior evidence (e.g., a tumor thought to be malignant was later shown to have actually been benign). Substantial evidence must show that had the new evidence (which relates to the prior determination) been considered at the time of the prior decision, the claim would not have been allowed or continued. A substitution of current judgment for that used in the prior favorable decision will not be the basis for applying this exception.
Example:
You were previously granted disability benefits on the basis of diabetes mellitus which the prior adjudicator believed was equivalent to the level of severity contemplated in the Listing of Impairments. The prior record shows that you had “brittle” diabetes for which you were taking insulin. Your urine was 3 + for sugar, and you alleged occasional hypoglycemic attacks caused by exertion. On review, symptoms, signs and laboratory findings are unchanged. The current adjudicator believes, however, that your impairment does not equal the severity contemplated by the listings. Error cannot be found because it would represent a substitution of current judgment for that of the prior adjudicator that your impairment equaled a listing.
(iv) The exception for error will not be applied retroactively under the conditions set out above unless the conditions for reopening the prior decision (see § 404.988) are met.
(4) You are currently engaging in substantial gainful activity. If you are currently engaging in substantial gainful activity before we determine whether you are no longer disabled because of your work activity, we will consider whether you are entitled to a trial work period as set out in § 404.1592. We will find that your disability has ended in the month in which you demonstrated your ability to engage in substantial gainful activity (following completion of a trial work period, where it applies). This exception does not apply in determining whether you continue to have a disabling impairment(§ 404.1511) for purposes of deciding your eligibility for a reentitlement period (§ 404.1592a).
(e) Second group of exceptions to medical improvement. In addition to the first group of exceptions to medical improvement, the following exceptions may result in a determination that you are no longer disabled. In these situations the decision will be made without a determination that you have medically improved or can engage in gainful activity.
(1) A prior determination or decision was fraudulently obtained. If we find that any prior favorable determination or decision was obtained by fraud, we may find that you are not disabled. In addition, we may reopen your claim under the rules in § 404.988. In determining whether a prior favorable determination or decision was fraudulently obtained, we will take into account any physical, mental, educational, or linguistic limitations (including any lack of facility with the English language) which you may have had at the time.
(2) You do not cooperate with us. If there is a question about whether you continue to be disabled and we ask you to give us medical or other evidence or to go for a physical or mental examination by a certain date, we will find that your disability has ended if you fail, without good cause, to do what we ask. Section 404.911 explains the factors we consider and how we will determine generally whether you have good cause for failure to cooperate. In addition, § 404.1518 discusses how we determine whether you have good cause for failing to attend a consultative examination. The month in which your disability ends will be the first month in which you failed to do what we asked.
(3) We are unable to find you. If there is a question about whether you continue to be disabled and we are unable to find you to resolve the question, we will determine that your disability has ended. The month your disability ends will be the first month in which the question arose and we could not find you.
(4) You fail to follow prescribed treatment which would be expected to restore your ability to engage in gainful activity. If treatment has been prescribed for you which would be expected to restore your ability to work, you must follow that treatment in order to be paid benefits. If you are not following that treatment and you do not have good cause for failing to follow that treatment, we will find that your disability has ended (see § 404.1530(c)). The month your disability ends will be the first month in which you failed to follow the prescribed treatment.
(f) Evaluation steps. To assure that disability reviews are carried out in a uniform manner, that decisions of continuing disability can be made in the most expeditious and administratively efficient way, and that any decisions to stop disability benefits are made objectively, neutrally and are fully documented, we will follow specific steps in reviewing the question of whether your disability continues. Our review may stop and benefits may be continued at any point if we determine there is sufficient evidence to find that you are still unable to engage in gainful activity. The steps are:
(1) Are you engaging in substantial gainful activity? If you are (and any applicable trial work period has been completed), we will find disability to have ended.
(2) If you are not, has there been medical improvement as defined in paragraph (b)(1) of this section? If there has been medical improvement as shown by a decrease in medical severity, see step (3). If there has been no decrease in medical severity, there has been no medical improvement. (see step (4).)
(3) If there has been medical improvement, we must determine (in accordance with paragraph (b)(2) of this section) whether it is related to your ability to work. If medical improvement is not related to your ability to do work, see step (4). If medical improvement is related to your ability to do work, see step (5).
(4) If we found at step (2) that there has been no medical improvement or if we found at step (3) that the medical improvement is not related to your ability to work, we consider whether any of the exceptions in paragraphs (d) and (e) of this section apply. If none of them apply, your disability will be found to continue. If one of the first group of exceptions to medical improvement (see paragraph (d) of this section) applies, we will proceed to step (5). If an exception from the second group of exceptions to medical improvement applies, your disability will be found to have ended. The second group of exceptions to medical improvement may be considered at any point in this process.
(5) If medical improvement is related to your ability to work or if one of the first group of exceptions to medical improvement applies, we will determine (considering all your impairments) whether the requirements of appendix 1 of this subpart are met or equaled. If your impairment(s) meets or equals the requirements of appendix 1 of this subpart, your disability will be found to continue. If not, your disability will be found to have ended.
(g) The month in which we will find you are no longer disabled. If the evidence shows that you are no longer disabled, we will find that your disability ended in the earliest of the following months—
(1) The month the evidence shows you are no longer disabled under the rules set out in this section, and you were disabled only for a specified period of time in the past;
(2) The month the evidence shows you are no longer disabled under the rules set out in this section, but not earlier than the month in which we mail you a notice saying that the information we have shows that you are not disabled;
(3) The month in which you demonstrated your ability to engage in substantial gainful activity (following completion of a trial work period); however, we may pay you benefits for certain months in and after the reentitlement period which follows the trial work period. (See § 404.1592 for a discussion of the trial work period, § 404.1592a for a discussion of the reentitlement period, and § 404.337 for when your benefits will end.);
(4) The month in which you return to full-time work, with no significant medical restrictions and acknowledge that medical improvement has occurred, as long as we expected your impairment(s) to improve (see § 404.1591);
(5) The first month in which you failed to do what we asked, without good cause when the rule set out in paragraph (e)(2) of this section applies;
(6) The first month in which the question of continuing disability arose and we could not find you, when the rule set out in paragraph (e)(3) of this section applies;
(7) The first month in which you failed to follow prescribed treatment without good cause, when the rule set out in paragraph (e)(4) of this section applies; or
(8) The first month you were told by your physician that you could return to work provided there is no substantial conflict between your physician's and your statements regarding your awareness of your capacity for work and the earlier date is supported by medical evidence.
(h) Before we stop your benefits. Before we determine you are no longer disabled, we will give you a chance to explain why we should not do so. Sections 404.1595 and 404.1597 describe your rights (including appeal rights) and the procedures we will follow.
[50 FR 50126, Dec. 6, 1985; 51 FR 7063, Feb. 28, 1986; 51 FR 16015, Apr. 30, 1986, as amended at 57 FR 30121, July 8, 1992; 59 FR 1635, Jan. 12, 1994; 82 FR 5871, Jan. 18, 2017]
Blindness
§ 404.1581 Meaning of blindness as defined in the law.
We will consider you blind under the law for a period of disability and for payment of disability insurance benefits if we determine that you are statutorily blind. Statutory blindness is defined in the law as central visual acuity of 20/200 or less in the better eye with the use of correcting lens. An eye which has a limitation in the field of vision so that the widest diameter of the visual field subtends an angle no greater than 20 degrees is considered to have a central visual acuity of 20/200 or less. Your blindness must meet the duration requirement in § 404.1509. We do not consider certain felony-related and prison-related impairments, as explained in § 404.1506.
[45 FR 55584, Aug. 20, 1980, as amended at 48 FR 5715, Feb. 8, 1983]
§ 404.1582 A period of disability based on blindness.
If we find that you are blind and you meet the insured status requirement, we may establish a period of disability for you regardless of whether you can do substantial gainful activity. A period of disability protects your earnings record under Social Security so that the time you are disabled will not count against you in determining whether you will have worked long enough to qualify for benefits and the amount of your benefits. However, you will not necessarily be entitled to receive disability insurance cash benefits even though you are blind. If you are a blind person under age 55, you must be unable to do any substantial gainful activity in order to be paid disability insurance cash benefits.
§ 404.1583 How we determine disability for blind persons who are age 55 or older.
We will find that you are eligible for disability insurance benefits even though you are still engaging in substantial gainful activity, if—
(a) You are blind;
(b) You are age 55 or older; and
(c) You are unable to use the skills or abilities like the ones you used in any substantial gainful activity which you did regularly and for a substantial period of time. (However, you will not be paid any cash benefits for any month in which you are doing substantial gainful activity.)
§ 404.1584 Evaluation of work activity of blind people.
(a) General. If you are blind (as explained in § 404.1581), we will consider the earnings from the work you are doing to determine whether or not you should be paid cash benefits.
(b) Under Age 55. If you are under age 55, we will evaluate the work you are doing using the guides in paragraph (d) of this section to determine whether or not your work shows that you are doing substantial gainful activity. If you are not doing substantial gainful activity, we will pay you cash benefits. If you are doing substantial gainful activity, we will not pay you cash benefits. However, you will be given a period of disability as described in subpart D of this part.
(c) Age 55 or older. If you are age 55 or older, we will evaluate your work using the guides in paragraph (d) of this section to determine whether or not your work shows that you are doing substantial gainful activity. If you have not shown this ability, we will pay you cash benefits. If you have shown an ability to do substantial gainful activity, we will evaluate your work activity to find out how your work compares with the work you did before. If the skills and abilities of your new work are about the same as those you used in the work you did before, we will not pay you cash benefits. However, if your new work requires skills and abilities which are less than or different than those you used in the work you did before, we will pay you cash benefits, but not for any month in which you actually perform substantial gainful activity.
(d) Evaluation of earnings —
(1) Earnings that will ordinarily show that you have engaged in substantial gainful activity. We will ordinarily consider that your earnings from your work activities show that you have engaged in substantial gainful activity if your monthly earnings average more than the amount(s) shown in paragraphs (d)(2) and (3) of this section. We will apply §§ 404.1574(a)(2), 404.1575(c), and 404.1576 in determining the amount of your average earnings.
(2) Substantial gainful activity guidelines for taxable years before 1978. For work activity performed in taxable years before 1978, the average earnings per month that we ordinarily consider enough to show that you have done substantial gainful activity are the same for blind people as for others. See § 404.1574(b)(2) for the earnings guidelines for other than blind individuals.
(3) Substantial gainful activity guidelines for taxable years beginning 1978. For taxable years beginning 1978, if you are blind, the law provides different earnings guidelines for determining if your earnings from your work activities are substantial gainful activity. Ordinarily, we consider your work to be substantial gainful activity, if your average monthly earnings are more than those shown in Table I. For years after 1977 and before 1996, increases in the substantial gainful activity guideline were linked to increases in the monthly exempt amount under the retirement earnings test for individuals aged 65 to 69. Beginning with 1996, increases in the substantial gainful activity amount have depended only on increases in the national average wage index.
Table I
| Over | In year(s) |
|---|---|
| $334 | 1978 |
| $375 | 1979 |
| $417 | 1980 |
| $459 | 1981 |
| $500 | 1982 |
| $550 | 1983 |
| $580 | 1984 |
| $610 | 1985 |
| $650 | 1986 |
| $680 | 1987 |
| $700 | 1988 |
| $740 | 1989 |
| $780 | 1990 |
| $810 | 1991 |
| $850 | 1992 |
| $880 | 1993 |
| $930 | 1994 |
| $940 | 1995 |
| $960 | 1996 |
| $1,000 | 1997 |
| $1,050 | 1998 |
| $1,110 | 1999 |
| $1,170 | 2000 |
[45 FR 55584, Aug. 20, 1980, as amended at 48 FR 21939, May 16, 1983; 65 FR 42786, July 11, 2000]
§ 404.1585 Trial work period for persons age 55 or older who are blind.
If you become eligible for disability benefits even though you were doing substantial gainful activity because you are blind and age 55 or older, you are entitled to a trial work period if—
(a) You later return to substantial gainful activity that requires skills or abilities comparable to those required in the work you regularly did before you became blind or became 55 years old, whichever is later; or
(b) Your last previous work ended because of an impairment and the current work requires a significant vocational adjustment.
§ 404.1586 Why and when we will stop your cash benefits.
(a) When you are not entitled to benefits. If you become entitled to disability cash benefits as a statutorily blind person, we will find that you are no longer entitled to benefits beginning with the earliest of—
(1) The month your vision, based on current medical evidence, does not meet the definition of blindness and your disability does not continue under the rules in § 404.1594 and you were disabled only for a specified period of time in the past;
(2) The month your vision, based on current medical evidence, does not meet the definition of blindness and your disability does not continue under the rules in § 404.1594, but not earlier than the month in which we mail you a notice saying that the information we have shows that you are not disabled;
(3) If you are under age 55, the month in which you demonstrated your ability to engage in substantial gainful activity (following completion of a trial work period); however, we may pay you benefits for certain months in and after the reentitlement period which follows the trial work period. (See § 404.1592a for a discussion of the reentitlement period, and § 404.316 on when your benefits will end.); or
(4) If you are age 55 or older, the month (following completion of a trial work period) when your work activity shows you are able to use, in substantial gainful activity, skills and abilities comparable to those of some gainful activity which you did with some regularity and over a substantial period of time. The skills and abilities are compared to the activity you did prior to age 55 or prior to becoming blind, whichever is later.
(b) If we find that you are not entitled to disability cash benefits. If we find that you are not entitled to disability cash benefits on the basis of your work activity but your visual impairment is sufficiently severe to meet the definition of blindness, the period of disability that we established for you will continue.
(c) If you do not follow prescribed treatment. If treatment has been prescribed for you that can restore your ability to work, you must follow that treatment in order to be paid benefits. If you are not following that treatment and you do not have a good reason for failing to follow that treatment (see § 404.1530(c)), we will find that your disability has ended. The month in which your disability will be found to have ended will be the first month in which you failed to follow the prescribed treatment.
(d) If you do not cooperate with us. If we ask you to give us medical or other evidence or to go for a medical examination by a certain date, we will find that your disability has ended if you fail, without good cause, to do what we ask. Section 404.911 explains the factors we consider and how we will determine generally whether you have good cause for failure to cooperate. In addition, § 404.1518 discusses how we determine whether you have good cause for failing to attend a consultative examination. The month in which your disability will be found to have ended will be the month in which you failed to do what we asked.
(e) If we are unable to find you. If there is a question about whether you continue to be disabled by blindness and we are unable to find you to resolve the question, we will find that your disability, has ended. The month it ends will be the first month in which the question arose and we could not find you.
(f) Before we stop your benefits. Before we stop your benefits or period of disability, we will give you a chance to give us your reasons why we should not stop your benefits or your period of disability. Section 404.1595 describes your rights and the procedures we will follow.
(g) If you are in an appropriate program of vocational rehabilitation services, employment services, or other support services.
(1) Your benefits, and those of your dependents, may be continued after your impairment is no longer disabling if—
(i) You are participating in an appropriate program of vocational rehabilitation services, employment services, or other support services, as described in § 404.327(a) and (b);
(ii) You began participating in the program before the date your disability ended; and
(iii) We have determined under § 404.328 that your completion of the program, or your continuation in the program for a specified period of time, will increase the likelihood that you will not have to return to the disability benefit rolls.
(2) We generally will stop your benefits with the earliest of these months—
(i) The month in which you complete the program; or
(ii) The month in which you stop participating in the program for any reason (see § 404.327(b) for what we mean by “participating” in the program); or
(iii) The month in which we determine under § 404.328 that your continuing participation in the program will no longer increase the likelihood that you will not have to return to the disability benefit rolls.
Exception to paragraph (d): In no case will we stop your benefits with a month earlier than the second month after the month your disability ends, provided that you meet all other requirements for entitlement to and payment of benefits through such month.
[45 FR 55584, Aug. 20, 1980, as amended at 47 FR 31543, July 21, 1982; 47 FR 52693, Nov. 23, 1982; 49 FR 22272, May 29, 1984; 50 FR 50130, Dec. 6, 1985; 51 FR 17617, May 14, 1986; 59 FR 1635, Jan. 12, 1994; 70 FR 36507, June 24, 2005]
§ 404.1587 Circumstances under which we may suspend and terminate your benefits before we make a determination.
(a) We will suspend your benefits if you are not disabled. We will suspend your benefits if all of the information we have clearly shows that you are not disabled and we will be unable to complete a determination soon enough to prevent us from paying you more monthly benefits than you are entitled to. This may occur when you are blind as defined in the law and age 55 or older and you have returned to work similar to work you previously performed.
(b) We will suspend your benefits if you fail to comply with our request for necessary information. We will suspend your benefits effective with the month in which it is determined in accordance with § 404.1596(b)(2)(i) that your disability benefits should stop due to your failure, without good cause (see § 404.911), to comply with our request for necessary information. When we have received the information, we will reinstate your benefits for any previous month for which they are otherwise payable, and continue with the CDR process.
(c) We will terminate your benefits. We will terminate your benefits following 12 consecutive months of benefit suspension because you did not comply with our request for information in accordance with § 404.1596(b)(2)(i). We will count the 12-month suspension period from the start of the first month that you stopped receiving benefits (see paragraph (b) of this section). This termination is effective with the start of the 13th month after the suspension began because you failed to cooperate.
[71 FR 60822, Oct. 17, 2006]
Continuing or Stopping Disability
§ 404.1588 Your responsibility to tell us of events that may change your disability status.
(a) Your responsibility to report changes to us. If you are entitled to cash benefits or to a period of disability because you are disabled, you should promptly tell us if—
(1) Your condition improves;
(2) You return to work;
(3) You increase the amount of your work; or
(4) Your earnings increase.
(b) Our responsibility when you report your work to us. When you or your representative report changes in your work activity to us under paragraphs (a)(2), (a)(3), and (a)(4) of this section, we will issue a receipt to you or your representative at least until a centralized computer file that records the information that you give us and the date that you make your report is in place. Once the centralized computer file is in place, we will continue to issue receipts to you or your representative if you request us to do so.
[71 FR 66866, Nov. 17, 2006]
§ 404.1589 We may conduct a review to find out whether you continue to be disabled.
After we find that you are disabled, we must evaluate your impairment(s) from time to time to determine if you are still eligible for disability cash benefits. We call this evaluation a continuing disability review. We may begin a continuing disability review for any number of reasons including your failure to follow the provisions of the Social Security Act or these regulations. When we begin such a review, we will notify you that we are reviewing your eligibility for disability benefits, why we are reviewing your eligibility, that in medical reviews the medical improvement review standard will apply, that our review could result in the termination of your benefits, and that you have the right to submit medical and other evidence for our consideration during the continuing disability review. In doing a medical review, we will develop a complete medical history of at least the preceding 12 months in any case in which a determination is made that you are no longer under a disability. If this review shows that we should stop payment of your benefits, we will notify you in writing and give you an opportunity to appeal. In § 404.1590 we describe those events that may prompt us to review whether you continue to be disabled.
[51 FR 16825, May 7, 1986]
§ 404.1590 When and how often we will conduct a continuing disability review.
(a) General. We conduct continuing disability reviews to determine whether or not you continue to meet the disability requirements of the law. Payment of cash benefits or a period of disability ends if the medical or other evidence shows that you are not disabled as determined under the standards set out in section 223(f) of the Social Security Act. In paragraphs (b) through (g) of this section, we explain when and how often we conduct continuing disability reviews for most individuals. In paragraph (h) of this section, we explain special rules for some individuals who are participating in the Ticket to Work program. In paragraph (i) of this section, we explain special rules for some individuals who work.
(b) When we will conduct a continuing disability review. Except as provided in paragraphs (h) and (i) of this section, we will start a continuing disability review if—
(1) You have been scheduled for a medical improvement expected diary review;
(2) You have been scheduled for a periodic review (medical improvement possible or medical improvement not expected) in accordance with the provisions of paragraph (d) of this section;
(3) We need a current medical or other report to see if your disability continues. (This could happen when, for example, an advance in medical technology, such as improved treatment for Alzheimer's disease or a change in vocational therapy or technology raises a disability issue.);
(4) You return to work and successfully complete a period of trial work;
(5) Substantial earnings are reported to your wage record;
(6) You tell us that—
(i) You have recovered from your disability; or
(ii) You have returned to work;
(7) Your State Vocational Rehabilitation Agency tells us that—
(i) The services have been completed; or
(ii) You are now working; or
(iii) You are able to work;
(8) Someone in a position to know of your physical or mental condition tells us any of the following, and it appears that the report could be substantially correct:
(i) You are not disabled; or
(ii) You are not following prescribed treatment; or
(iii) You have returned to work; or
(iv) You are failing to follow the provisions of the Social Security Act or these regulations;
(9) Evidence we receive raises a question as to whether your disability continues; or
(10) You have been scheduled for a vocational reexamination diary review.
(c) Definitions. As used in this section—
Medical improvement expected diary —refers to a case which is scheduled for review at a later date because the individual's impairment(s) is expected to improve. Generally, the diary period is set for not less than 6 months or for not more than 18 months. Examples of cases likely to be scheduled for medical improvement expected diary are fractures and cases in which corrective surgery is planned and recovery can be anticipated.
Permanent impairment —medical improvement not expected—refers to a case in which any medical improvement in the person's impairment(s) is not expected. This means an extremely severe condition determined on the basis of our experience in administering the disability programs to be at least static, but more likely to be progressively disabling either by itself or by reason of impairment complications, and unlikely to improve so as to permit the individual to engage in substantial gainful activity. The interaction of the individual's age, impairment consequences and lack of recent attachment to the labor market may also be considered in determining whether an impairment is permanent. Improvement which is considered temporary under § 404.1579(c)(4) or § 404.1594(c)(3)(iv), as appropriate, will not be considered in deciding if an impairment is permanent. Examples of permanent impairments taken from the list contained in our other written guidelines which are available for public review are as follows and are not intended to be all inclusive:
(1) Parkinsonian Syndrome which has reached the level of severity necessary to meet the Listing in appendix 1.
(2) Amyotrophic Lateral Sclerosis which has reached the level of severity necessary to meet the Listing in appendix 1.
(3) Diffuse pulmonary fibrosis in an individual age 55 or over which has reached the level of severity necessary to meet the Listing in appendix 1.
(4) Amputation of leg at hip.
Nonpermanent impairment —refers to a case in which any medical improvement in the person's impairment(s) is possible. This means an impairment for which improvement cannot be predicted based on current experience and the facts of the particular case but which is not at the level of severity of an impairment that is considered permanent. Examples of nonpermanent impairments are: regional enteritis, hyperthyroidism, and chronic ulcerative colitis.
Vocational reexamination diary —refers to a case which is scheduled for review at a later date because the individual is undergoing vocational therapy, training or an educational program which may improve his or her ability to work so that the disability requirement of the law is no longer met. Generally, the diary period will be set for the length of the training, therapy, or program of education.
(d) Frequency of review. If your impairment is expected to improve, generally we will review your continuing eligibility for disability benefits at intervals from 6 months to 18 months following our most recent decision. Our notice to you about the review of your case will tell you more precisely when the review will be conducted. If your disability is not considered permanent but is such that any medical improvement in your impairment(s) cannot be accurately predicted, we will review your continuing eligibility for disability benefits at least once every 3 years. If your disability is considered permanent, we will review your continuing eligibility for benefits no less frequently than once every 7 years but no more frequently than once every 5 years. Regardless of your classification, we will conduct an immediate continuing disability review if a question of continuing disability is raised pursuant to paragraph (b) of this section.
(e) Change in classification of impairment. If the evidence developed during a continuing disability review demonstrates that your impairment has improved, is expected to improve, or has worsened since the last review, we may reclassify your impairment to reflect this change in severity. A change in the classification of your impairment will change the frequency with which we will review your case. We may also reclassify certain impairments because of improved tests, treatment, and other technical advances concerning those impairments.
(f) Review after administrative appeal. If you were found eligible to receive or to continue to receive disability benefits on the basis of a decision by an administrative law judge, the Appeals Council or a Federal court, we will not conduct a continuing disability review earlier than 3 years after that decision unless your case should be scheduled for a medical improvement expected or vocational reexamination diary review or a question of continuing disability is raised pursuant to paragraph (b) of this section.
(g) Waiver of timeframes. All cases involving a nonpermanent impairment will be reviewed by us at least once every 3 years unless we, after consultation with the State agency, determine that the requirement should be waived to ensure that only the appropriate number of cases are reviewed. The appropriate number of cases to be reviewed is to be based on such considerations as the backlog of pending reviews, the projected number of new applications, and projected staffing levels. Such waiver shall be given only after good faith effort on the part of the State to meet staffing requirements and to process the reviews on a timely basis. Availability of independent medical resources may also be a factor. A waiver in this context refers to our administrative discretion to determine the appropriate number of cases to be reviewed on a State by State basis. Therefore, your continuing disability review may be delayed longer than 3 years following our original decision or other review under certain circumstances. Such a delay would be based on our need to ensure that backlogs, reviews required to be performed by the Social Security Disability Benefits Reform Act of 1984 (Pub. L. 98-460), and new disability claims workloads are accomplished within available medical and other resources in the State agency and that such reviews are done carefully and accurately.
(h) If you are participating in the Ticket to Work program. If you are participating in the Ticket to Work program, we will not start a continuing disability review during the period in which you are using a ticket. However, this provision does not apply to reviews we conduct using the rules in §§ 404.1571-404.1576 to determine whether the work you have done shows that you are able to do substantial gainful activity and are, therefore, no longer disabled. See subpart C of part 411 of this chapter.
(i) If you are working and have received social security disability benefits for at least 24 months —
(1) General. Notwithstanding the provisions in paragraphs (b)(4), (b)(5), (b)(6)(ii), (b)(7)(ii), and (b)(8)(iii) of this section, we will not start a continuing disability review based solely on your work activity if—
(i) You are currently entitled to disability insurance benefits as a disabled worker, child's insurance benefits based on disability, or widow's or widower's insurance benefits based on disability; and
(ii) You have received such benefits for at least 24 months (see paragraph (i)(2) of this section).
(2) The 24-month requirement.
(i) The months for which you have actually received disability insurance benefits as a disabled worker, child's insurance benefits based on disability, or widow's or widower's insurance benefits based on disability that you were due, or for which you have constructively received such benefits, will count for the 24-month requirement under paragraph (i)(1)(ii) of this section, regardless of whether the months were consecutive. We will consider you to have constructively received a benefit for a month for purposes of the 24-month requirement if you were otherwise due a social security disability benefit for that month and your monthly benefit was withheld to recover an overpayment. Any month for which you were entitled to benefits but for which you did not actually or constructively receive a benefit payment will not be counted for the 24-month requirement. Months for which your social security disability benefits are continued under § 404.1597a pending reconsideration and/or a hearing before an administrative law judge on a medical cessation determination will not be counted for the 24-month requirement. If you also receive supplemental security income payments based on disability or blindness under title XVI of the Social Security Act, months for which you received only supplemental security income payments will not be counted for the 24-month requirement.
(ii) In determining whether paragraph (i)(1) of this section applies, we consider whether you have received disability insurance benefits as a disabled worker, child's insurance benefits based on disability, or widow's or widower's insurance benefits based on disability for at least 24 months as of the date on which we start a continuing disability review. For purposes of this provision, the date on which we start a continuing disability review is the date on the notice we send you that tells you that we are beginning to review your disability case.
(3) When we may start a continuing disability review even if you have received social security disability benefits for at least 24 months. Even if you meet the requirements of paragraph (i)(1) of this section, we may still start a continuing disability review for a reason(s) other than your work activity. We may start a continuing disability review if we have scheduled you for a periodic review of your continuing disability, we need a current medical or other report to see if your disability continues, we receive evidence which raises a question as to whether your disability continues, or you fail to follow the provisions of the Social Security Act or these regulations. For example, we will start a continuing disability review when you have been scheduled for a medical improvement expected diary review, and we may start a continuing disability review if you failed to report your work to us.
(4) Reviews to determine whether the work you have done shows that you are able to do substantial gainful activity. Paragraph (i)(1) of this section does not apply to reviews we conduct using the rules in §§ 404.1571-404.1576 to determine whether the work you have done shows that you are able to do substantial gainful activity and are, therefore, no longer disabled.
(5) Erroneous start of the continuing disability review. If we start a continuing disability review based solely on your work activity that results in a medical cessation determination, we will vacate the medical cessation determination if—
(i) You provide us evidence that establishes that you met the requirements of paragraph (i)(1) of this section as of the date of the start of your continuing disability review and that the start of the review was erroneous; and
(ii) We receive the evidence within 12 months of the date of the notice of the initial determination of medical cessation.
[51 FR 16825, May 7, 1986, as amended at 71 FR 66856, Nov. 17, 2006]
§ 404.1591 If your medical recovery was expected and you returned to work.
If your impairment was expected to improve and you returned to full-time work with no significant medical limitations and acknowledge that medical improvement has occurred, we may find that your disability ended in the month you returned to work. Unless there is evidence showing that your disability has not ended, we will use the medical and other evidence already in your file and the fact that you returned to full-time work without significant limitations to determine that you are no longer disabled. (If your impairment is not expected to improve, we will not ordinarily review your claim until the end of the trial work period, as described in § 404.1592.)
Example:
Evidence obtained during the processing of your claim showed that you had an impairment that was expected to improve about 18 months after your disability began. We, therefore, told you that your claim would be reviewed again at that time. However, before the time arrived for your scheduled medical re-examination, you told us that you had returned to work and your impairment had improved. We investigated immediately and found that, in the 16th month after your disability began, you returned to full-time work without any significant medical restrictions. Therefore, we would find that your disability ended in the first month you returned to full-time work.
[50 FR 50130, Dec. 6, 1985]
§ 404.1592 The trial work period.
(a) Definition of the trial work period. The trial work period is a period during which you may test your ability to work and still be considered disabled. It begins and ends as described in paragraph (e) of this section. During this period, you may perform services (see paragraph (b) of this section) in as many as 9 months, but these months do not have to be consecutive. We will not consider those services as showing that your disability has ended until you have performed services in at least 9 months. However, after the trial work period has ended we will consider the work you did during the trial work period in determining whether your disability ended at any time after the trial work period.
(b) What we mean by services. When used in this section, services means any activity (whether legal or illegal), even though it is not substantial gainful activity, which is done in employment or self-employment for pay or profit, or is the kind normally done for pay or profit. We generally do not consider work done without remuneration to be services if it is done merely as therapy or training or if it is work usually done in a daily routine around the house or in self-care. We will not consider work you have done as a volunteer in the federal programs described in section 404.1574(d) in determining whether you have performed services in the trial work period.
(1) If you are an employee. We will consider your work as an employee to be services if:
(i) Before January 1, 2002, your earnings in a month were more than the amount(s) indicated in Table 1 for the year(s) in which you worked.
(ii) Beginning January 1, 2002, your earnings in a month are more than an amount determined for each calendar year to be the larger of:
(A) Such amount for the previous year, or
(B) An amount adjusted for national wage growth, calculated by multiplying $530 by the ratio of the national average wage index for the year 2 calendar years before the year for which the amount is being calculated to the national average wage index for 1999. We will then round the resulting amount to the next higher multiple of $10 where such amount is a multiple of $5 but not of $10 and to the nearest multiple of $10 in any other case.
(2) If you are self-employed. We will consider your activities as a self-employed person to be services if:
(i) Before January 1, 2002, your net earnings in a month were more than the amount(s) indicated in Table 2 of this section for the year(s) in which you worked, or the hours you worked in the business in a month are more than the number of hours per month indicated in Table 2 for the years in which you worked.
(ii) Beginning January 1, 2002, you work more than 80 hours a month in the business, or your net earnings in a month are more than an amount determined for each calendar year to be the larger of:
(A) Such amount for the previous year, or
(B) An amount adjusted for national wage growth, calculated by multiplying $530 by the ratio of the national average wage index for the year 2 calendar years before the year for which the amount is being calculated to the national average wage index for 1999. We will then round the resulting amount to the next higher multiple of $10 where such amount is a multiple of $5 but not of $10 and to the nearest multiple of $10 in any other case.
Table 1—For Employees
| For months | You earn more than |
|---|---|
| In calendar years before 1979 | $50 |
| In calendar years 1979-1989 | 75 |
| In calendar years 1990-2000 | 200 |
| In calendar year 2001 | 530 |
Table 2—For the Self-Employed
| For months | Your net earnings are more than | Or you work in the business more than |
|---|---|---|
| In calendar years before 1979 | $50 | 15 hours. |
| In calendar years 1979-1989 | 75 | 15 hours. |
| In calendar years 1990-2000 | 200 | 40 hours. |
| In calendar year 2001 | 530 | 80 hours. |
(c) Limitations on the number of trial work periods. You may have only one trial work period during a period of entitlement to cash benefits.
(d) Who is and is not entitled to a trial work period.
(1) You are generally entitled to a trial work period if you are entitled to disability insurance benefits, child's benefits based on disability, or widow's or widower's or surviving divorced spouse's benefits based on disability.
(2) You are not entitled to a trial work period—
(i) If you are entitled to a period of disability but not to disability insurance benefits, and you are not entitled to any other type of disability benefit under title II of the Social Security Act (i.e., child's benefits based on disability, or widow's or widower's benefits or surviving divorced spouse's benefits based on disability);
(ii) If you perform work demonstrating the ability to engage in substantial gainful activity during any required waiting period for benefits;
(iii) If you perform work demonstrating the ability to engage in substantial gainful activity within 12 months of the onset of the impairment(s) that prevented you from performing substantial gainful activity and before the date of any notice of determination or decision finding that you are disabled; or
(iv) For any month prior to the month of your application for disability benefits (see paragraph (e) of this section).
(e) When the trial work period begins and ends. The trial work period begins with the month in which you become entitled to disability insurance benefits, to child's benefits based on disability or to widow's, widower's, or surviving divorced spouse's benefits based on disability. It cannot begin before the month in which you file your application for benefits, and for widows, widowers, and surviving divorced spouses, it cannot begin before December 1, 1980. It ends with the close of whichever of the following calendar months is the earliest:
(1) The 9th month (whether or not the months have been consecutive) in which you have performed services if that 9th month is prior to January 1992;
(2) The 9th month (whether or not the months have been consecutive and whether or not the previous 8 months of services were prior to January 1992) in which you have performed services within a period of 60 consecutive months if that 9th month is after December 1991; or
(3) The month in which new evidence, other than evidence relating to any work you did during the trial work period, shows that you are not disabled, even though you have not worked a full 9 months. We may find that your disability has ended at any time during the trial work period if the medical or other evidence shows that you are no longer disabled. See § 404.1594 for information on how we decide whether your disability continues or ends.
(f) Nonpayment of benefits for trial work period service months. See § 404.471 for an explanation of when benefits for trial work period service months are not payable if you are convicted by a Federal court of fraudulently concealing your work activity.
[45 FR 55584, Aug. 20, 1980, as amended at 49 FR 22273, May 29, 1984; 50 FR 50130, Dec. 6, 1985; 54 FR 53605, Dec. 29, 1989; 65 FR 42787, July 11, 2000; 65 FR 82910, Dec. 29, 2000; 71 FR 66866, Nov. 17, 2006]
§ 404.1592a The reentitlement period.
(a) General. The reentitlement period is an additional period after 9 months of trial work during which you may continue to test your ability to work if you have a disabling impairment, as defined in § 404.1511. If you work during the reentitlement period, we may decide that your disability has ceased because your work is substantial gainful activity and stop your benefits. However, if, after the month for which we found that your disability ceased because you performed substantial gainful activity, you stop engaging in substantial gainful activity, we will start paying you benefits again; you will not have to file a new application. The following rules apply if you complete a trial work period and continue to have a disabling impairment:
(1) The first time you work after the end of your trial work period and engage in substantial gainful activity, we will find that your disability ceased. When we decide whether this work is substantial gainful activity, we will apply all of the relevant provisions of §§ 404.1571-404.1576 including, but not limited to, the provisions for averaging earnings, unsuccessful work attempts, and deducting impairment-related work expenses, as well as the special rules for evaluating the work you do after you have received disability benefits for at least 24 months. We will find that your disability ceased in the first month after the end of your trial work period in which you do substantial gainful activity, applying all the relevant provisions in §§ 404.1571-404.1576.
(2)
(i) If we determine under paragraph (a)(1) of this section that your disability ceased during the reentitlement period because you perform substantial gainful activity, you will be paid benefits for the first month after the trial work period in which you do substantial gainful activity (i.e., the month your disability ceased) and the two succeeding months, whether or not you do substantial gainful activity in those succeeding months. After those three months, we will stop your benefits for any month in which you do substantial gainful activity. (See §§ 404.316, 404.337, 404.352 and 404.401a.) If your benefits are stopped because you do substantial gainful activity, they may be started again without a new application and a new determination of disability if you stop doing substantial gainful activity in a month during the reentitlement period. In determining whether you do substantial gainful activity in a month for purposes of stopping or starting benefits during the reentitlement period, we will consider only your work in, or earnings for, that month. Once we have determined that your disability has ceased during the reentitlement period because of the performance of substantial gainful activity as explained in paragraph (a)(1) of this section, we will not apply the provisions of §§ 404.1574(c) and 404.1575(d) regarding unsuccessful work attempts, the provisions of § 404.1574a regarding averaging of earnings, or the special rules in §§ 404.1574(b)(3)(iii) and 404.1575(e) for evaluating the work you do after you have received disability benefits for at least 24 months, to determine whether benefits should be paid for any particular month in the reentitlement period that occurs after the month your disability ceased.
(ii) If anyone else is receiving monthly benefits based on your earnings record, that individual will not be paid benefits for any month for which you cannot be paid benefits during the reentitlement period.
(3) The way we will consider your work activity after your reentitlement period ends (see paragraph (b)(2) of this section) will depend on whether you worked during the reentitlement period and if you did substantial gainful activity.
(i) If you worked during the reentitlement period and we decided that your disability ceased during the reentitlement period because of your work under paragraph (a)(1) of this section, we will find that your entitlement to disability benefits terminates in the first month in which you engaged in substantial gainful activity after the end of the reentitlement period (see § 404.325). (See § 404.321 for when entitlement to a period of disability ends.) When we make this determination, we will consider only your work in, or earnings for, that month; we will not apply the provisions of §§ 404.1574(c) and 404.1575(d) regarding unsuccessful work attempts, the provisions of § 404.1574a regarding averaging of earnings, or the special rules in §§ 404.1574(b)(3)(iii) and 404.1575(e) for evaluating the work you do after you have received disability benefits for at least 24 months.
(ii) If we did not find that your disability ceased because of work activity during the reentitlement period, we will apply all of the relevant provisions of §§ 404.1571-404.1576 including, but not limited to, the provisions for averaging earnings, unsuccessful work attempts, and deducting impairment-related work expenses, as well as the special rules for evaluating the work you do after you have received disability benefits for at least 24 months, to determine whether your disability ceased because you performed substantial gainful activity after the reentitlement period. If we find that your disability ceased because you performed substantial gainful activity in a month after your reentitlement period ended, you will be paid benefits for the month in which your disability ceased and the two succeeding months. After those three months, your entitlement to a period of disability or to disability benefits terminates (see §§ 404.321 and 404.325).
(b) When the reentitlement period begins and ends. The reentitlement period begins with the first month following completion of 9 months of trial work but cannot begin earlier than December 1, 1980. It ends with whichever is earlier—
(1) The month before the first month in which your impairment no longer exists or is not medically disabling; or
(2)
(i) The last day of the 15th month following the end of your trial work period if you were not entitled to benefits after December 1987; or
(ii) The last day of the 36th month following the end of your trial work period if you were entitled to benefits after December 1987 or if the 15-month period described in paragraph (b)(2)(i) of this section had not ended as of January 1988. (See §§ 404.316, 404.337, and 404.352 for when your benefits end.)
(c) When you are not entitled to a reentitlement period. You are not entitled to a reentitlement period if:
(1) You are entitled to a period of disability, but not to disability insurance cash benefits;
(2) You are not entitled to a trial work period;
(3) Your entitlement to disability insurance benefits ended before you completed 9 months of trial work in that period of disability.
[49 FR 22273, May 29, 1984, as amended at 58 FR 64883, Dec. 10, 1993; 65 FR 42787, July 11, 2000; 71 FR 66856, Nov. 17, 2006]
§ 404.1592b What is expedited reinstatement?
The expedited reinstatement provision provides you another option for regaining entitlement to benefits when we previously terminated your entitlement to disability benefits due to your work activity. The expedited reinstatement provision provides you the option of requesting that your prior entitlement to disability benefits be reinstated, rather than filing a new application for a new period of entitlement. Since January 1, 2001, you can request to be reinstated to benefits if you stop doing substantial gainful activity within 60 months of your prior termination. You must not be able to do substantial gainful activity because of your medical condition. Your current impairment must be the same as or related to your prior impairment and you must be disabled. To determine if you are disabled, we will use our medical improvement review standard that we use in our continuing disability review process. The advantage of using the medical improvement review standard is that we will generally find that you are disabled unless your impairment has improved so that you are able to work or unless an exception under the medical improvement review standard process applies. We explain the rules for expedited reinstatement in §§ 404.1592c through 404.1592f.
[70 FR 57142, Sept. 30, 2005]
§ 404.1592c Who is entitled to expedited reinstatement?
(a) You can have your entitlement to benefits reinstated under expedited reinstatement if—
(1) You were previously entitled to a disability benefit on your own record of earnings as indicated in § 404.315, or as a disabled widow or widower as indicated in § 404.335, or as a disabled child as indicated in § 404.350, or to Medicare entitlement based on disability and Medicare qualified government employment as indicated in 42 CFR 406.15;
(2) Your disability entitlement referred to in paragraph (a)(1) of this section was terminated because you did substantial gainful activity;
(3) You file your request for reinstatement timely under § 404.1592d; and
(4) In the month you file your request for reinstatement—
(i) You are not able or become unable to do substantial gainful activity because of your medical condition as determined under paragraph (c) of this section;
(ii) Your current impairment is the same as or related to the impairment that we used as the basis for your previous entitlement referred to in paragraph (a)(2) of this section; and
(iii) You are disabled, as determined under the medical improvement review standard in §§ 404.1594(a) through (e).
(b) You are entitled to reinstatement on the record of an insured person who is or has been reinstated if—
(1) You were previously entitled to one of the following benefits on the record of the insured person—
(i) A spouse or divorced spouse benefit under §§ 404.330 and 404.331;
(ii) A child's benefit under § 404.350; or
(iii) A parent's benefit under § 404.370;
(2) You were entitled to benefits on the record when we terminated the insured person's entitlement;
(3) You meet the requirements for entitlement to the benefit described in the applicable paragraph (b)(1)(i) through (b)(1)(iii) of this section; and
(4) You request to be reinstated.
(c) We will determine that you are not able to do substantial gainful activity because of your medical condition, under paragraph (a)(4)(i) of this section, when:
(1) You certify under § 404.1592d(d)(2) that you are unable to do substantial gainful activity because of your medical condition;
(2) You are not able or become unable to do substantial gainful activity in the month you file your request for reinstatement; and
(3) We determine that you are disabled under paragraph (a)(4)(iii) of this section.
[70 FR 57142, Sept. 30, 2005, as amended at 81 FR 71369, Oct. 17, 2016]
§ 404.1592d How do I request reinstatement?
(a) You must make your request for reinstatement in writing.
(b) You must have filed your request on or after January 1, 2001.
(c) You must provide the information we request so that we can determine whether you meet the requirements for reinstatement as indicated in § 404.1592c.
(d) If you request reinstatement under § 404.1592c(a)—
(1) We must receive your request within the consecutive 60-month period that begins with the month in which your entitlement terminated due to doing substantial gainful activity. If we receive your request after the 60-month period we can grant you an extension if we determine you had good cause under the standards explained in § 404.911 for not filing the request timely; and
(2) You must certify that you are disabled, that your current impairment(s) is the same as or related to the impairment(s) that we used as the basis for the benefit you are requesting to be reinstated, and that you are unable to do substantial gainful activity because of your medical condition.
[70 FR 57142, Sept. 30, 2005]
§ 404.1592e How do we determine provisional benefits?
(a) You may receive up to 6 consecutive months of provisional cash benefits and Medicare during the provisional benefit period, while we determine whether we can reinstate your disability benefit entitlement under § 404.1592c—
(1) We will pay you provisional benefits, and reinstate your Medicare if you are not already entitled to Medicare, beginning with the month you file your request for reinstatement under § 404.1592c(a) if you do not perform substantial gainful activity in that month. We will pay you provisional benefits, and reinstate your Medicare if you are not already entitled to Medicare, beginning with the month after you file your request for reinstatement under § 404.1592c(a) if you perform substantial gainful activity in the month in which you file your request for reinstatement.
(2) We will pay you a monthly provisional benefit amount equal to the last monthly benefit payable to you during your prior entitlement, increased by any cost of living increases that would have been applicable to the prior benefit amount under § 404.270. The last monthly benefit payable is the amount of the monthly insurance benefit we determined that was actually paid to you for the month before the month in which your entitlement was terminated, after we applied the reduction, deduction and nonpayment provisions in § 404.401 through § 404.480.
(3) If you are entitled to another monthly benefit payable under the provisions of title II of the Act for the same month you can be paid a provisional benefit, we will pay you an amount equal to the higher of the benefits payable.
(4) If you request reinstatement for more than one benefit entitlement, we will pay you an amount equal to the higher of the provisional benefits payable.
(5) If you are eligible for Supplemental Security Income payments, including provisional payments, we will reduce your provisional benefits under § 404.408b if applicable.
(6) We will not reduce your provisional benefit, or the payable benefit to other individuals entitled on an earnings record, under § 404.403, when your provisional benefit causes the total benefits payable on the earnings record to exceed the family maximum.
(b) You cannot receive provisional cash benefits or Medicare a second time under this section when—
(1) You request reinstatement under § 404.1592c(a);
(2) You previously received provisional cash benefits or Medicare under this section based upon a prior request for reinstatement filed under § 404.1592c(a); and
(3) Your requests under paragraphs (b)(1) and (b)(2) are for the same previous disability entitlement referred to in § 404.1592c(a)(2).
(4) Examples:
Example 1:
Mr. K files a request for reinstatement in April 2004. His disability benefit had previously terminated in January 2003. Since Mr. K meets other factors for possible reinstatement (i.e., his prior entitlement was terminated within the last 60 months because he was engaging in substantial gainful activity), we start paying him provisional benefits beginning April 2004 while we determine whether he is disabled and whether his current impairment(s) is the same as or related to the impairment(s) that we used as the basis for the benefit that was terminated in January 2003. In July 2004 we determine that Mr. K cannot be reinstated because he is not disabled under the medical improvement review standard; therefore we stop his provisional benefits. Mr. K does not request review of that determination. In January 2005 Mr. K again requests reinstatement on the entitlement that terminated in January 2003. Since this request meets all the factors for possible reinstatement, and his request is still within 60 months from January 2003, we will make a new determination on whether he is disabled and whether his current impairment(s) is the same as or related to the impairment(s) that we used as the basis for the benefit that was terminated in January 2003. Since the January 2005 request and the April 2004 request both request reinstatement on the same entitlement that terminated in January 2003, and since we already paid Mr. K provisional benefits based upon the April 2004 request, we will not pay additional provisional benefits on the January 2005 request for reinstatement.
Example 2:
Assume the same facts as shown in Example 1 of this section, with the addition of these facts. We approve Mr. K's January 2005 request for reinstatement and start his reinstated benefits beginning January 2005. Mr. K subsequently returns to work and his benefits are again terminated due to engaging in substantial gainful activity in January 2012. Mr. K must again stop work and requests reinstatement in January 2015. Since Mr. K meets other factors for possible reinstatement (i.e., his prior entitlement was terminated within the last 60 months because he was engaging in substantial gainful activity) we start paying him provisional benefits beginning January 2015 while we determine whether he is disabled and whether his current impairment(s) is the same as or related to the impairment(s) that we used as the basis for the benefit that was terminated in January 2012.
(c) We will not pay you a provisional benefit for a month when an applicable nonpayment rule applies. Examples of when we will not pay a benefit include, but are not limited to—
(1) If you are a prisoner under § 404.468;
(2) If you have been removed/deported under § 404.464; or
(3) If you are an alien outside the United States under § 404.460.
(d) We will not pay you a provisional benefit for any month that is after the earliest of the following months—
(1) The month we send you a notice of our determination on your request for reinstatement;
(2) The month you do substantial gainful activity;
(3) The month before the month you attain full retirement age; or
(4) The fifth month following the month you requested expedited reinstatement.
(e) You are not entitled to provisional benefits if—
(1) Prior to starting your provisional benefits, we determine that you do not meet the requirements for reinstatement under §§ 404.1592c(a); or
(2) We determine that your statements on your request for reinstatement, made under § 404.1592d(d)(2), are false.
(f) Determinations we make regarding your provisional benefits under paragraphs (a) through (e) of this section are final and are not subject to administrative and judicial review under subpart J of part 404.
(g) If you were previously overpaid benefits under title II or title XVI of the Act, we will not recover the overpayment from your provisional benefits unless you give us permission. We can recover Medicare premiums you owe from your provisional benefits.
(h) If we determine you are not entitled to reinstated benefits, provisional benefits we have already paid you under this section that were made prior to the termination month under paragraph (d) of this section will not be subject to recovery as an overpayment unless we determine that you knew, or should have known, you did not meet the requirements for reinstatement in § 404.1592c. If we inadvertently pay you provisional benefits when you are not entitled to them because we have already made a determination described in paragraph (e) of this section, they will be subject to recover as an overpayment under subpart F of part 404.
[70 FR 57142, Sept. 30, 2005, as amended at 81 FR 71369, Oct. 17, 2016]
§ 404.1592f How do we determine reinstated benefits?
(a) If you meet the requirements for reinstatement under § 404.1592c(a), we will then consider in which month to reinstate your entitlement. We will reinstate your entitlement with the earliest month, in the 12-month period that ends with the month before you filed your request for reinstatement, that you would have met all of the requirements under § 404.1592c(a) if you had filed your request for reinstatement in that month. Otherwise, you will be entitled to reinstated benefits beginning with the month in which you filed your request for such benefits if you did not perform substantial gainful activity in that month. If you performed substantial gainful activity in the month of filing, but are no longer able to perform substantial gainful activity, we will reinstate your benefits with the month after the month you filed your request for reinstatement. We cannot reinstate your entitlement for any month prior to January 2001.
(b) When your entitlement is reinstated, you are also entitled to Medicare benefits under the provisions of 42 CFR part 406.
(c) We will compute your reinstated benefit amount and determine benefits payable under the applicable paragraphs of §§ 404.201 through 404.480 with certain exceptions—
(1) We will reduce your reinstated benefit due in a month by the amount of the provisional benefit we already paid you for that month. If your provisional benefit paid for a month exceeds the reinstated benefit, we will treat the difference as an overpayment under §§ 404.501 through 404.527.
(2) If you are reinstated on your own earnings record, we will compute your primary insurance amount with the same date of onset we used in your most recent period of disability on your earnings record.
(d) We will not pay you reinstated benefits for any months of substantial gainful activity during your initial reinstatement period. During the initial reinstatement period, the trial work period provisions of § 404.1592 and the reentitlement period provisions of § 404.1592a do not apply. The initial reinstatement period begins with the month your reinstated benefits begin under paragraph (a) of this section and ends when you have had 24 payable months of reinstated benefits. We consider you to have a payable month for the purposes of this paragraph when you do not do substantial gainful activity in that month and when the non-payment provisions in subpart E of part 404 also do not apply. If the amount of the provisional benefit already paid you for a month equals or exceeds the amount of the reinstated benefit payable for that month so that no additional payment is due, we will consider that month a payable month. When we determine if you have done substantial gainful activity in a month during the initial reinstatement period, we will consider only your work in, or earnings for, that month. We will not apply the unsuccessful work attempt provisions of §§ 404.1574(c) and 404.1575(d) or the averaging of earnings provisions in § 404.1574a.
(e) After you complete the 24-month initial reinstatement period as indicated in paragraph (d) of this section, your subsequent work will be evaluated under the trial work provisions in § 404.1592 and then the reentitlement period in § 404.1592a.
(f) Your entitlement to reinstated benefits ends with the month before the earliest of the following months—
(2) The month in which you reach retirement age;
(3) The third month following the month in which your disability ceases; or
(4) The month in which you die.
(g) Determinations we make under §§ 404.1592f are initial determinations under § 404.902 and subject to review under subpart J of part 404.
(h) If we determine you are not entitled to reinstated benefits we will consider your request filed under § 404.1592c(a) your intent to claim benefits under § 404.630.
[70 FR 57142, Sept. 30, 2005, as amended at 82 FR 7648, Jan. 21, 2017]
§ 404.1593 Medical evidence in continuing disability review cases.
(a) General. If you are entitled to benefits or if a period of disability has been established for you because you are disabled, we will have your case file with the supporting medical evidence previously used to establish or continue your entitlement. Generally, therefore, the medical evidence we will need for a continuing disability review will be that required to make a current determination or decision as to whether you are still disabled, as defined under the medical improvement review standard. See §§ 404.1579 and 404.1594.
(b) Obtaining evidence from your medical sources. You must provide us with reports from your physician, psychologist, or others who have treated or evaluated you, as well as any other evidence that will help us determine if you are still disabled. See § 404.1512. You must have a good reason for not giving us this information or we may find that your disability has ended. See § 404.1594(e)(2). If we ask you, you must contact your medical sources to help us get the medical reports. We will make every reasonable effort to help you in getting medical reports when you give us permission to request them from your physician, psychologist, or other medical sources. See § 404.1512(d)(1) concerning what we mean by every reasonable effort. In some instances, such as when a source is known to be unable to provide certain tests or procedures or is known to be nonproductive or uncooperative, we may order a consultative examination while awaiting receipt of medical source evidence. Before deciding that your disability has ended, we will develop a complete medical history covering at least the 12 months preceding the date you sign a report about your continuing disability status. See § 404.1512(c).
(c) When we will purchase a consultative examination. A consultative examination may be purchased when we need additional evidence to determine whether or not your disability continues. As a result, we may ask you, upon our request and reasonable notice, to undergo consultative examinations and tests to help us determine if you are still disabled. See § 404.1517. We will decide whether or not to purchase a consultative examination in accordance with the standards in §§ 404.1519a through 404.1519b.
[56 FR 36962, Aug. 1, 1991]
§ 404.1594 How we will determine whether your disability continues or ends.
(a) General. There is a statutory requirement that, if you are entitled to disability benefits, your continued entitlement to such benefits must be reviewed periodically. If you are entitled to disability benefits as a disabled worker or as a person disabled since childhood, or, for monthly benefits payable for months after December 1990, as a disabled widow, widower, or surviving divorced spouse, there are a number of factors we consider in deciding whether your disability continues. We must determine if there has been any medical improvement in your impairment(s) and, if so, whether this medical improvement is related to your ability to work. If your impairment(s) has not medically improved we must consider whether one or more of the exceptions to medical improvement applies. If medical improvement related to your ability to work has not occurred and no exception applies, your benefits will continue. Even where medical improvement related to your ability to work has occurred or an exception applies, in most cases (see paragraph (e) of this section for exceptions), we must also show that you are currently able to engage in substantial gainful activity before we can find that you are no longer disabled.
(b) Terms and definitions. There are several terms and definitions which are important to know in order to understand how we review whether your disability continues. In addition, see paragraph (i) of this section if you work during your current period of entitlement based on disability or during certain other periods.
(1) Medical improvement. Medical improvement is any decrease in the medical severity of your impairment(s) which was present at the time of the most recent favorable medical decision that you were disabled or continued to be disabled. A determination that there has been a decrease in medical severity must be based on improvement in the symptoms, signs, and/or laboratory findings associated with your impairment(s).
Example 1:
You were awarded disability benefits due to a herniated nucleus pulposus. At the time of our prior decision granting you benefits you had had a laminectomy. Postoperatively, a myelogram still shows evidence of a persistent deficit in your lumbar spine. You had pain in your back, and pain and a burning sensation in your right foot and leg. There were no muscle weakness or neurological changes and a modest decrease in motion in your back and leg. When we reviewed your claim, your medical source, who has treated you, reported that he or she had seen you regularly every 2 to 3 months for the past 2 years. No further myelograms had been done, complaints of pain in the back and right leg continued especially on sitting or standing for more than a short period of time. Your doctor further reported a moderately decreased range of motion in your back and right leg, but again no muscle atrophy or neurological changes were reported. Medical improvement has not occurred because there has been no decrease in the severity of your back impairment as shown by changes in symptoms, signs or laboratory findings.
Example 2:
You were awarded disability benefits due to rheumatoid arthritis. At the time, laboratory findings were positive for this condition. Your doctor reported persistent swelling and tenderness of your fingers and wrists and that you complained of joint pain. Current medical evidence shows that while laboratory tests are still positive for rheumatoid arthritis, your impairment has responded favorably to therapy so that for the last year your fingers and wrists have not been significantly swollen or painful. Medical improvement has occurred because there has been a decrease in the severity of your impairment as documented by the current symptoms and signs reported by your physician. Although your impairment is subject to temporary remission and exacerbations, the improvement that has occurred has been sustained long enough to permit a finding of medical improvement. We would then determine if this medical improvement is related to your ability to work.
(2) Medical improvement not related to ability to do work. Medical improvement is not related to your ability to work if there has been a decrease in the severity of the impairment(s) as defined in paragraph (b)(1) of this section, present at the time of the most recent favorable medical decision, but no increase in your functional capacity to do basic work activities as defined in paragraph (b)(4) of this section. If there has been any medical improvement in your impairment(s), but it is not related to your ability to do work and none of the exceptions applies, your benefits will be continued.
Example:
You are 65 inches tall and weighed 246 pounds at the time your disability was established. You had venous insufficiency and persistent edema in your legs. At the time, your ability to do basic work activities was affected because you were able to sit for 6 hours, but were able to stand or walk only occasionally. At the time of our continuing disability review, you had undergone a vein stripping operation. You now weigh 220 pounds and have intermittent edema. You are still able to sit for 6 hours at a time and to stand or walk only occasionally although you report less discomfort on walking. Medical improvement has occurred because there has been a decrease in the severity of the existing impairment as shown by your weight loss and the improvement in your edema. This medical improvement is not related to your ability to work, however, because your functional capacity to do basic work activities (i.e., the ability to sit, stand and walk) has not increased.
(3) Medical improvement that is related to ability to do work. Medical improvement is related to your ability to work if there has been a decrease in the severity, as defined in paragraph (b)(1) of this section, of the impairment(s) present at the time of the most recent favorable medical decision and an increase in your functional capacity to do basic work activities as discussed in paragraph (b)(4) of this section. A determination that medical improvement related to your ability to do work has occurred does not, necessarily, mean that your disability will be found to have ended unless it is also shown that you are currently able to engage in substantial gainful activity as discussed in paragraph (b)(5) of this section.
Example 1:
You have a back impairment and had a laminectomy to relieve the nerve root impingement and weakness in your left leg. At the time of our prior decision, basic work activities were affected because you were able to stand less than 6 hours, and sit no more than 1⁄2 hour at a time. You had a successful fusion operation on your back about 1 year before our review of your entitlement. At the time of our review, the weakness in your leg has decreased. Your functional capacity to perform basic work activities now is unimpaired because you now have no limitation on your ability to sit, walk, or stand. Medical improvement has occurred because there has been a decrease in the severity of your impairment as demonstrated by the decreased weakness in your leg. This medical improvement is related to your ability to work because there has also been an increase in your functional capacity to perform basic work activities (or residual functional capacity) as shown by the absence of limitation on your ability to sit, walk, or stand. Whether or not your disability is found to have ended, however, will depend on our determination as to whether you can currently engage in substantial gainful activity.
Example 2:
You were injured in an automobile accident receiving a compound fracture to your right femur and a fractured pelvis. When you applied for disability benefits 10 months after the accident your doctor reported that neither fracture had yet achieved solid union based on his clinical examination. X-rays supported this finding. Your doctor estimated that solid union and a subsequent return to full weight bearing would not occur for at least 3 more months. At the time of our review 6 months later, solid union had occurred and you had been returned to full weight-bearing for over a month. Your doctor reported this and the fact that your prior fractures no longer placed any limitation on your ability to walk, stand, lift, etc., and, that in fact, you could return to fulltime work if you so desired.
Medical improvement has occurred because there has been a decrease in the severity of your impairments as shown by X-ray and clinical evidence of solid union and your return to full weight-bearing. This medical improvement is related to your ability to work because you no longer meet the same listed impairment in appendix 1 of this subpart (see paragraph (c)(3)(i) of this section). In fact, you no longer have an impairment which is severe (see § 404.1521) and your disability will be found to have ended.
(4) Functional capacity to do basic work activities. Under the law, disability is defined, in part, as the inability to do any substantial gainful activity by reason of any medically determinable physical or mental impairment(s). In determining whether you are disabled under the law, we must measure, therefore, how and to what extent your impairment(s) has affected your ability to do work. We do this by looking at how your functional capacity for doing basic work activities has been affected. Basic work activities means the abilities and aptitudes necessary to do most jobs. Included are exertional abilities such as walking, standing, pushing, pulling, reaching and carrying, and nonexertional abilities and aptitudes such as seeing, hearing, speaking, remembering, using judgment, dealing with changes and dealing with both supervisors and fellow workers. A person who has no impairment(s) would be able to do all basic work activities at normal levels; he or she would have an unlimited functional capacity to do basic work activities. Depending on its nature and severity, an impairment will result in some limitation to the functional capacity to do one or more of these basic work activities. Diabetes, for example, can result in circulatory problems which could limit the length of time a person could stand or walk and damage to his or her eyes as well, so that the person also had limited vision. What a person can still do despite an impairment, is called his or her residual functional capacity. How the residual functional capacity is assessed is discussed in more detail in § 404.1545. Unless an impairment is so severe that it is deemed to prevent you from doing substantial gainful activity (see §§ 404.1525 and 404.1526), it is this residual functional capacity that is used to determine whether you can still do your past work or, in conjunction with your age, education and work experience, any other work.
(i) A decrease in the severity of an impairment as measured by changes (improvement) in symptoms, signs or laboratory findings can, if great enough, result in an increase in the functional capacity to do work activities. Vascular surgery (e.g., femoropopliteal bypass) may sometimes reduce the severity of the circulatory complications of diabetes so that better circulation results and the person can stand or walk for longer periods. When new evidence showing a change in signs, symptoms and laboratory findings establishes that both medical improvement has occurred and your functional capacity to perform basic work activities, or residual functional capacity, has increased, we say that medical improvement which is related to your ability to do work has occurred. A residual functional capacity assessment is also used to determine whether you can engage in substantial gainful activity and, thus, whether you continue to be disabled (see paragraph (b)(5) of this section).
(ii) Many impairment-related factors must be considered in assessing your functional capacity for basic work activities. Age is one key factor. Medical literature shows that there is a gradual decrease in organ function with age; that major losses and deficits become irreversible over time and that maximum exercise performance diminishes with age. Other changes related to sustained periods of inactivity and the aging process include muscle atrophy, degenerative joint changes, decrease in range of motion, and changes in the cardiac and respiratory systems which limit the exertional range.
(iii) Studies have also shown that the longer an individual is away from the workplace and is inactive, the more difficult it becomes to return to ongoing gainful employment. In addition, a gradual change occurs in most jobs so that after about 15 years, it is no longer realistic to expect that skills and abilities acquired in these jobs will continue to apply to the current workplace. Thus, if you are age 50 or over and have been receiving disability benefits for a considerable period of time, we will consider this factor along with your age in assessing your residual functional capacity. This will ensure that the disadvantages resulting from inactivity and the aging process during a long period of disability will be considered. In some instances where available evidence does not resolve what you can or cannot do on a sustained basis, we will provide special work evaluations or other appropriate testing.
(5) Ability to engage in substantial gainful activity. In most instances, we must show that you are able to engage in substantial gainful activity before your benefits are stopped. When doing this, we will consider all your current impairments not just that impairment(s) present at the time of the most recent favorable determination. If we cannot determine that you are still disabled based on medical considerations alone (as discussed in §§ 404.1525 and 404.1526), we will use the new symptoms, signs and laboratory findings to make an objective assessment of your functional capacity to do basic work activities or residual functional capacity and we will consider your vocational factors. See §§ 404.1545 through 404.1569.
(6) Evidence and basis for our decision. Our decisions under this section will be made on a neutral basis without any initial inference as to the presence or absence of disability being drawn from the fact that you have previously been determined to be disabled. We will consider all evidence you submit and that we obtain from your medical sources and nonmedical sources. What constitutes evidence and our procedures for obtaining it are set out in §§ 404.1512 through 404.1518. Our determination regarding whether your disability continues will be made on the basis of the weight of the evidence.
(7) Point of comparison. For purposes of determining whether medical improvement has occurred, we will compare the current medical severity of that impairment(s) which was present at the time of the most recent favorable medical decision that you were disabled or continued to be disabled to the medical severity of that impairment(s) at that time. If medical improvement has occurred, we will compare your current functional capacity to do basic work activities (i.e., your residual functional capacity) based on this previously existing impairment(s) with your prior residual functional capacity in order to determine whether the medical improvement is related to your ability to do work. The most recent favorable medical decision is the latest decision involving a consideration of the medical evidence and the issue of whether you were disabled or continued to be disabled which became final.
(c) Determining medical improvement and its relationship to your abilities to do work. Paragraphs (b) (1) through (3) of this section discuss what we mean by medical improvement, medical improvement not related to your ability to work and medical improvement that is related to your ability to work. (In addition, see paragraph (i) of this section if you work during your current period of entitlement based on disability or during certain other periods.) How we will arrive at the decision that medical improvement has occurred and its relationship to the ability to do work, is discussed below.
(1) Medical improvement. Medical improvement is any decrease in the medical severity of impairment(s) present at the time of the most recent favorable medical decision that you were disabled or continued to be disabled and is determined by a comparison of prior and current medical evidence which must show that there have been changes (improvement) in the symptoms, signs or laboratory findings associated with that impairment(s).
(2) Determining if medical improvement is related to ability to work. If there is a decrease in medical severity as shown by the symptoms, signs and laboratory findings, we then must determine if it is related to your ability to do work. In paragraph (b)(4) of this section, we explain the relationship between medical severity and limitation on functional capacity to do basic work activities (or residual functional capacity) and how changes in medical severity can affect your residual functional capacity. In determining whether medical improvement that has occurred is related to your ability to do work, we will assess your residual functional capacity (in accordance with paragraph (b)(4) of this section) based on the current severity of the impairment(s) which was present at your last favorable medical decision. Your new residual functional capacity will then be compared to your residual functional capacity at the time of our most recent favorable medical decision. Unless an increase in the current residual functional capacity is based on changes in the signs, symptoms, or laboratory findings, any medical improvement that has occurred will not be considered to be related to your ability to do work.
(3) Following are some additional factors and considerations which we will apply in making these determinations.
(i) Previous impairment met or equaled listings. If our most recent favorable decision was based on the fact that your impairment(s) at the time met or equaled the severity contemplated by the Listing of Impairments in appendix 1 of this subpart, an assessment of your residual functional capacity would not have been made. If medical improvement has occurred and the severity of the prior impairment(s) no longer meets or equals the same listing section used to make our most recent favorable decision, we will find that the medical improvement was related to your ability to work. Appendix 1 of this subpart describes impairments which, if severe enough, affect a person's ability to work. If the appendix level of severity is met or equaled, the individual is deemed, in the absence of evidence to the contrary, to be unable to engage in substantial gainful activity. If there has been medical improvement to the degree that the requirement of the listing section is no longer met or equaled, then the medical improvement is related to your ability to work. We must, of course, also establish that you can currently engage in gainful activity before finding that your disability has ended.
(ii) Prior residual functional capacity assessment made. The residual functional capacity assessment used in making the most recent favorable medical decision will be compared to the residual functional capacity assessment based on current evidence in order to determine if your functional capacity for basic work activities has increased. There will be no attempt made to reassess the prior residual functional capacity.
(iii) Prior residual functional capacity assessment should have been made, but was not. If the most recent favorable medical decision should have contained an assessment of your residual functional capacity (i.e., your impairments did not meet or equal the level of severity contemplated by the Listing of Impairments in appendix 1 of this subpart) but does not, either because this assessment is missing from your file or because it was not done, we will reconstruct the residual functional capacity. This reconstructed residual functional capacity will accurately and objectively assess your functional capacity to do basic work activities. We will assign the maximum functional capacity consistent with an allowance.
Example:
You were previously found to be disabled on the basis that “while your impairment did not meet or equal a listing, it did prevent you from doing your past or any other work.” The prior adjudicator did not, however, include a residual functional capacity assessment in the rationale of this decision and a review of the prior evidence does not show that such an assessment was ever made. If a decrease in medical severity, i.e., medical improvement, has occurred, the residual functional capacity based on the current level of severity of your impairment will have to be compared with your residual functional capacity based on its prior severity in order to determine if the medical improvement is related to your ability to do work. In order to make this comparison, we will review the prior evidence and make an objective assessment of your residual functional capacity at the time of our most recent favorable medical determination, based on the symptoms, signs and laboratory findings as they then existed.
(iv) Impairment subject to temporary remission. In some cases the evidence shows that an individual's impairments are subject to temporary remission. In assessing whether medical improvement has occurred in persons with this type of impairment, we will be careful to consider the longitudinal history of the impairments, including the occurrence of prior remission, and prospects for future worsenings. Improvement in such impairments that is only temporary will not warrant a finding of medical improvement.
(v) Prior file cannot be located. If the prior file cannot be located, we will first determine whether you are able to now engage in substantial gainful activity based on all your current impairments. (In this way, we will be able to determine that your disability continues at the earliest point without addressing the often lengthy process of reconstructing prior evidence.) If you cannot engage in substantial gainful activity currently, your benefits will continue unless one of the second group of exceptions applies (see paragraph (e) of this section). If you are able to engage in substantial gainful activity, we will determine whether an attempt should be made to reconstruct those portions of the missing file that were relevant to our most recent favorable medical decision (e.g., work history, medical evidence, and the results of consultative examinations). This determination will consider the potential availability of old records in light of their age, whether the source of the evidence is still in operation; and whether reconstruction efforts will yield a complete record of the basis for the most recent favorable medical decision. If relevant parts of the prior record are not reconstructed either because it is determined not to attempt reconstruction or because such efforts fail, medical improvement cannot be found. The documentation of your current impairments will provide a basis for any future reviews. If the missing file is later found, it may serve as a basis for reopening any decision under this section in accordance with the rules in § 404.988.
(d) First group of exceptions to medical improvement. The law provides for certain limited situations when your disability can be found to have ended even though medical improvement has not occurred, if you can engage in substantial gainful activity. These exceptions to medical improvement are intended to provide a way of finding that a person is no longer disabled in those limited situations where, even though there has been no decrease in severity of the impairment(s), evidence shows that the person should no longer be considered disabled or never should have been considered disabled. If one of these exceptions applies, we must also show that, taking all your current impairment(s) into account, not just those that existed at the time of our most recent favorable medical decision, you are now able to engage in substantial gainful activity before your disability can be found to have ended. As part of the review process, you will be asked about any medical or vocational therapy you received or are receiving. Your answers and the evidence gathered as a result as well as all other evidence, will serve as the basis for the finding that an exception applies.
(1) Substantial evidence shows that you are the beneficiary of advances in medical or vocational therapy or technology (related to your ability to work). Advances in medical or vocational therapy or technology are improvements in treatment or rehabilitative methods which have increased your ability to do basic work activities. We will apply this exception when substantial evidence shows that you have been the beneficiary of services which reflect these advances and they have favorably affected the severity of your impairment or your ability to do basic work activities. This decision will be based on new medical evidence and a new residual functional capacity assessment. (See § 404.1545.) In many instances, an advanced medical therapy or technology will result in a decrease in severity as shown by symptoms, signs and laboratory findings which will meet the definition of medical improvement. This exception will, therefore, see very limited application.
(2) Substantial evidence shows that you have undergone vocational therapy (related to your ability to work). Vocational therapy (related to your ability to work) may include, but is not limited to, additional education, training, or work experience that improves your ability to meet the vocational requirements of more jobs. This decision will be based on substantial evidence which includes new medical evidence and a new residual functional capacity assessment. (See § 404.1545.) If, at the time of our review you have not completed vocational therapy which could affect the continuance of your disability, we will review your claim upon completion of the therapy.
Example 1:
You were found to be disabled because the limitations imposed on you by your impairment allowed you to only do work that was at a sedentary level of exertion. Your prior work experience was work that required a medium level of exertion. Your age and education at the time would not have qualified you for work that was below this medium level of exertion. You enrolled in and completed a specialized training course which qualifies you for a job in data processing as a computer programmer in the period since you were awarded benefits. On review of your claim, current evidence shows that there is no medical improvement and that you can still do only sedentary work. As the work of a computer programmer is sedentary in nature, you are now able to engage in substantial gainful activity when your new skills are considered.
Example 2:
You were previously entitled to benefits because the medical evidence and assessment of your residual functional capacity showed you could only do light work. Your prior work was considered to be heavy in nature and your age, education and the nature of your prior work qualified you for work which was no less than medium in exertion. The current evidence and residual functional capacity show there has been no medical improvement and that you can still do only light work. Since you were originally entitled to benefits, your vocational rehabilitation agency enrolled you in and you successfully completed a trade school course so that you are now qualified to do small appliance repair. This work is light in nature, so when your new skills are considered, you are now able to engage in substantial gainful activity even though there has been no change in your residual functional capacity.
(3) Substantial evidence shows that based on new or improved diagnostic or evaluative techniques your impairment(s) is not as disabling as it was considered to be at the time of the most recent favorable decision. Changing methodologies and advances in medical and other diagnostic or evaluative techniques have given, and will continue to give, rise to improved methods for measuring and documenting the effect of various impairments on the ability to do work. Where, by such new or improved methods, substantial evidence shows that your impairment(s) is not as severe as was determined at the time of our most recent favorable medical decision, such evidence may serve as a basis for finding that you are no longer disabled, if you can currently engage in substantial gainful activity. In order to be used under this exception, however, the new or improved techniques must have become generally available after the date of our most recent favorable medical decision.
(i) How we will determine which methods are new or improved techniques and when they become generally available. New or improved diagnostic techniques or evaluations will come to our attention by several methods. In reviewing cases, we often become aware of new techniques when their results are presented as evidence. Such techniques and evaluations are also discussed and acknowledged in medical literature by medical professional groups and other governmental entities. Through these sources, we develop listings of new techniques and when they become generally available. For example, we will consult the Health Care Financing Administration for its experience regarding when a technique is recognized for payment under Medicare and when they began paying for the technique.
(ii) How you will know which methods are new or improved techniques and when they become generally available. We will let you know which methods we consider to be new or improved techniques and when they become available through two vehicles.
(A) Some of the future changes in the Listing of Impairments in appendix 1 of this subpart will be based on new or improved diagnostic or evaluative techniques. Such listings changes will clearly state this fact as they are published as Notices of Proposed Rulemaking and the new or improved technique will be considered generally available as of the date of the final publication of that particular listing in the Federal Register.
(B) A cumulative list since 1970 of new or improved diagnostic techniques or evaluations, how they changed the evaluation of the applicable impairment and the month and year they became generally available, will be published in the Notices section of the Federal Register. Included will be any changes in the Listing of Impairments published in the Code of Federal Regulations since 1970 which are reflective of new or improved techniques. No cases will be processed under this exception until this cumulative listing is so published. Subsequent changes to the list will be published periodically. The period will be determined by the volume of changes needed.
Example:
The electrocardiographic exercise test has replaced the Master's 2-step test as a measurement of heart function since the time of your last favorable medical decision. Current evidence could show that your condition, which was previously evaluated based on the Master's 2-step test, is not now as disabling as was previously thought. If, taking all your current impairments into account, you are now able to engage in substantial gainful activity, this exception would be used to find that you are no longer disabled even if medical improvement has not occurred.
(4) Substantial evidence demonstrates that any prior disability decision was in error. We will apply the exception to medical improvement based on error if substantial evidence (which may be evidence on the record at the time any prior determination of the entitlement to benefits based on disability was made, or newly obtained evidence which relates to that determination) demonstrates that a prior determination was in error. A prior determination will be found in error only if:
(i) Substantial evidence shows on its face that the decision in question should not have been made (e.g., the evidence in your file such as pulmonary function study values was misread or an adjudicative standard such as a listing in appendix 1 or a medical/vocational rule in appendix 2 of this subpart was misapplied).
Example 1:
You were granted benefits when it was determined that your epilepsy met Listing 11.02. This listing calls for a finding of major motor seizures more frequently than once a month as documented by EEG evidence and by a detailed description of a typical seizure pattern. A history of either diurnal episodes or nocturnal episodes with residuals interfering with daily activities is also required. On review, it is found that a history of the frequency of your seizures showed that they occurred only once or twice a year. The prior decision would be found to be in error, and whether you were still considered to be disabled would be based on whether you could currently engage in substantial gainful activity.
Example 2:
Your prior award of benefits was based on vocational rule 201.12 in appendix 2 of this subpart. This rule applies to a person age 50-54 who has at least a high school education, whose previous work was entirely at a semiskilled level, and who can do only sedentary work. On review, it is found that at the time of the prior determination you were actually only age 46 and vocational rule 201.21 should have been used. This rule would have called for a denial of your claim and the prior decision is found to have been in error. Continuation of your disability would depend on a finding of your current ability to engage in substantial gainful activity.
(ii) At the time of the prior evaluation, required and material evidence of the severity of your impairment(s) was missing. That evidence becomes available upon review, and substantial evidence demonstrates that had such evidence been present at the time of the prior determination, disability would not have been found.
Example:
You were found disabled on the basis of chronic obstructive pulmonary disease. The severity of your impairment was documented primarily by pulmonary function testing results. The evidence showed that you could do only light work. Spirometric tracings of this testing, although required, were not obtained, however. On review, the original report is resubmitted by the consultative examining physician along with the corresponding spirometric tracings. A review of the tracings shows that the test was invalid. Current pulmonary function testing supported by spirometric tracings reveals that your impairment does not limit your ability to perform basic work activities in any way. Error is found based on the fact that required, material evidence which was originally missing now becomes available and shows that if it had been available at the time of the prior determination, disability would not have been found.
(iii) Substantial evidence which is new evidence which relates to the prior determination (of allowance or continuance) refutes the conclusions that were based upon the prior evidence (e.g., a tumor thought to be malignant was later shown to have actually been benign). Substantial evidence must show that had the new evidence (which relates to the prior determination) been considered at the time of the prior decision, the claim would not have been allowed or continued. A substitution of current judgment for that used in the prior favorable decision will not be the basis for applying this exception.
Example:
You were previously found entitled to benefits on the basis of diabetes mellitus which the prior adjudicator believed was equivalent to the level of severity contemplated in the Listing of Impairments. The prior record shows that you had “brittle” diabetes for which you were taking insulin. Your urine was 3 + for sugar, and you alleged occasional hypoglycemic attacks caused by exertion. On review, symptoms, signs and laboratory findings are unchanged. The current adjudicator feels, however, that your impairment clearly does not equal the severity contemplated by the listings. Error cannot be found because it would represent a substitution of current judgment for that of the prior adjudicator that your impairment equaled a listing.
(iv) The exception for error will not be applied retroactively under the conditions set out above unless the conditions for reopening the prior decision (see § 404.988) are met.
(5) You are currently engaging in substantial gainful activity. If you are currently engaging in substantial gainful activity before we determine whether you are no longer disabled because of your work activity, we will consider whether you are entitled to a trial work period as set out in § 404.1592. We will find that your disability has ended in the month in which you demonstrated your ability to engage in substantial gainful activity (following completion of a trial work period, where it applies). This exception does not apply in determining whether you continue to have a disabling impairment(s) (§ 404.1511) for purposes of deciding your eligibility for a reentitlement period (§ 404.1592a).
(e) Second group of exceptions to medical improvement. In addition to the first group of exceptions to medical improvement, the following exceptions may result in a determination that you are no longer disabled. In these situations the decision will be made without a determination that you have medically improved or can engage in substantial gainful activity.
(1) A prior determination or decision was fraudulently obtained. If we find that any prior favorable determination or decision was obtained by fraud, we may find that you are not disabled. In addition, we may reopen your claim under the rules in § 404.988. In determining whether a prior favorable determination or decision was fraudulently obtained, we will take into account any physical, mental, educational, or linguistic limitations (including any lack of facility with the English language) which you may have had at the time.
(2) You do not cooperate with us. If there is a question about whether you continue to be disabled and we ask you to give us medical or other evidence or to go for a physical or mental examination by a certain date, we will find that your disability has ended if you fail, without good cause, to do what we ask. Section 404.911 explains the factors we consider and how we will determine generally whether you have good cause for failure to cooperate. In addition, § 404.1518 discusses how we determine whether you have good cause for failing to attend a consultative examination. The month in which your disability ends will be the first month in which you failed to do what we asked.
(3) We are unable to find you. If there is a question about whether you continue to be disabled and we are unable to find you to resolve the question, we will determine that your disability has ended. The month your disability ends will be the first month in which the question arose and we could not find you.
(4) You fail to follow prescribed treatment which would be expected to restore your ability to engage in substantial gainful activity. If treatment has been prescribed for you which would be expected to restore your ability to work, you must follow that treatment in order to be paid benefits. If you are not following that treatment and you do not have good cause for failing to follow that treatment, we will find that your disability has ended (see § 404.1530(c)). The month your disability ends will be the first month in which you failed to follow the prescribed treatment.
(f) Evaluation steps. To assure that disability reviews are carried out in a uniform manner, that decisions of continuing disability can be made in the most expeditious and administratively efficient way, and that any decisions to stop disability benefits are made objectively, neutrally and are fully documented, we will follow specific steps in reviewing the question of whether your disability continues. Our review may cease and benefits may be continued at any point if we determine there is sufficient evidence to find that you are still unable to engage in substantial gainful activity. The steps are as follows. (See paragraph (i) of this section if you work during your current period of entitlement based on disability or during certain other periods.)
(1) Are you engaging in substantial gainful activity? If you are (and any applicable trial work period has been completed), we will find disability to have ended (see paragraph (d)(5) of this section).
(2) If you are not, do you have an impairment or combination of impairments which meets or equals the severity of an impairment listed in appendix 1 of this subpart? If you do, your disability will be found to continue.
(3) If you do not, has there been medical improvement as defined in paragraph (b)(1) of this section? If there has been medical improvement as shown by a decrease in medical severity, see step (4). If there has been no decrease in medical severity, there has been no medical improvement. (See step (5).)
(4) If there has been medical improvement, we must determine whether it is related to your ability to do work in accordance with paragraphs (b) (1) through (4) of this section; i.e., whether or not there has been an increase in the residual functional capacity based on the impairment(s) that was present at the time of the most recent favorable medical determination. If medical improvement is not related to your ability to do work, see step (5). If medical improvement is related to your ability to do work, see step (6).
(5) If we found at step (3) that there has been no medical improvement or if we found at step (4) that the medical improvement is not related to your ability to work, we consider whether any of the exceptions in paragraphs (d) and (e) of this section apply. If none of them apply, your disability will be found to continue. If one of the first group of exceptions to medical improvement applies, see step (6). If an exception from the second group of exceptions to medical improvement applies, your disability will be found to have ended. The second group of exceptions to medical improvement may be considered at any point in this process.
(6) If medical improvement is shown to be related to your ability to do work or if one of the first group of exceptions to medical improvement applies, we will determine whether all your current impairments in combination are severe (see § 404.1521). This determination will consider all your current impairments and the impact of the combination of those impairments on your ability to function. If the residual functional capacity assessment in step (4) above shows significant limitation of your ability to do basic work activities, see step (7). When the evidence shows that all your current impairments in combination do not significantly limit your physical or mental abilities to do basic work activities, these impairments will not be considered severe in nature. If so, you will no longer be considered to be disabled.
(7) If your impairment(s) is severe, we will assess your current ability to do substantial gainful activity in accordance with § 404.1560. That is, we will assess your residual functional capacity based on all your current impairments and consider whether you can still do work you have done in the past. If you can do such work, disability will be found to have ended.
(8) If you are not able to do work you have done in the past, we will consider whether you can do other work given the residual functional capacity assessment made under paragraph (f)(7) of this section and your age, education, and past work experience (see paragraph (f)(9) of this section for an exception to this rule). If you can, we will find that your disability has ended. If you cannot, we will find that your disability continues.
(9) We may proceed to the final step, described in paragraph (f)(8) of this section, if the evidence in your file about your past relevant work is not sufficient for us to make a finding under paragraph (f)(7) of this section about whether you can perform your past relevant work. If we find that you can adjust to other work based solely on your age, education, and residual functional capacity, we will find that you are no longer disabled, and we will not make a finding about whether you can do your past relevant work under paragraph (f)(7) of this section. If we find that you may be unable to adjust to other work or if § 404.1562 may apply, we will assess your claim under paragraph (f)(7) of this section and make a finding about whether you can perform your past relevant work.
(g) The month in which we will find you are no longer disabled. If the evidence shows that you are no longer disabled, we will find that your disability ended in the earliest of the following months.
(1) The month the evidence shows you are no longer disabled under the rules set out in this section, and you were disabled only for a specified period of time in the past;
(2) The month the evidence shows you are no longer disabled under the rules set out in this section, but not earlier than the month in which we mail you a notice saying that the information we have shows that you are not disabled;
(3) The month in which you demonstrated your ability to engage in substantial gainful activity (following completion of a trial work period); however, we may pay you benefits for certain months in and after the reentitlement period which follows the trial work period. (See § 404.1592a for a discussion of the reentitlement period. If you are receiving benefits on your own earnings record, see § 404.316 for when your benefits will end. See § 404.352 if you are receiving benefits on a parent's earnings as a disabled adult child.);
(4) The month in which you actually do substantial gainful activity (where you are not entitled to a trial work period);
(5) The month in which you return to full-time work, with no significant medical restrictions and acknowledge that medical improvement has occurred, and we expected your impairment(s) to improve (see § 404.1591);
(6) The first month in which you failed without good cause to do what we asked, when the rule set out in paragraph (e)(2) of this section applies;
(7) The first month in which the question of continuing disability arose and we could not find you, when the rule set out in paragraph (e)(3) of this section applies;
(8) The first month in which you failed without good cause to follow prescribed treatment, when the rule set out in paragraph (e)(4) of this section applies; or
(9) The first month you were told by your physician that you could return to work, provided there is no substantial conflict between your physician's and your statements regarding your awareness of your capacity for work and the earlier date is supported by substantial evidence.
(h) Before we stop your benefits. Before we stop your benefits or a period of disability, we will give you a chance to explain why we should not do so. Sections 404.1595 and 404.1597 describe your rights (including appeal rights) and the procedures we will follow.
(i) If you work during your current period of entitlement based on disability or during certain other periods.
(1) We will not consider the work you are doing or have done during your current period of entitlement based on disability (or, when determining whether you are entitled to expedited reinstatement of benefits under section 223(i) of the Act, the work you are doing or have done during or after the previously terminated period of entitlement referred to in section 223(i)(1)(B) of the Act) to be past relevant work under paragraph (f)(7) of this section or past work experience under paragraph (f)(8) of this section. In addition, if you are currently entitled to disability benefits under title II of the Social Security Act, we may or may not consider the physical and mental activities that you perform in the work you are doing or have done during your current period of entitlement based on disability, as explained in paragraphs (i)(2) and (3) of this section.
(2) If you are currently entitled to disability insurance benefits as a disabled worker, child's insurance benefits based on disability, or widow's or widower's insurance benefits based on disability under title II of the Social Security Act, and at the time we are making a determination on your case you have received such benefits for at least 24 months, we will not consider the activities you perform in the work you are doing or have done during your current period of entitlement based on disability if they support a finding that your disability has ended. (We will use the rules in § 404.1590(i)(2) to determine whether the 24-month requirement is met.) However, we will consider the activities you do in that work if they support a finding that your disability continues or they do not conflict with a finding that your disability continues. We will not presume that you are still disabled if you stop working.
(3) If you are not a person described in paragraph (i)(2) of this section, we will consider the activities you perform in your work at any of the evaluation steps in paragraph (f) of this section at which we need to assess your ability to function.
[50 FR 50130, Dec. 6, 1985; 51 FR 7063, Feb. 28, 1986; 51 FR 16015, Apr. 30, 1986, as amended at 52 FR 44971, Nov. 24, 1987; 57 FR 30121, July 8, 1992; 59 FR 1635, Jan. 12, 1994; 65 FR 42788, July 11, 2000; 68 FR 51163, Aug. 26, 2003; 71 FR 66857, Nov. 17, 2006; 77 FR 43495, July 25, 2012; 82 FR 5871, Jan. 18, 2017]
§ 404.1595 When we determine that you are not now disabled.
(a) When we will give you advance notice. Except in those circumstances described in paragraph (d) of this section, we will give you advance notice when we have determined that you are not now disabled because the information we have conflicts with what you have told us about your disability. If your dependents are receiving benefits on your Social Security number and do not live with you, we will also give them advance notice. To give you advance notice, we will contact you by mail, telephone or in person.
(b) What the advance notice will tell you. We will give you a summary of the information we have. We will also tell you why we have determined that you are not now disabled, and will give you a chance to reply. If it is because of—
(1) Medical reasons. The advance notice will tell you what the medical information in your file shows;
(2) Your work activity. The advance notice will tell you what information we have about the work you are doing or have done, and why this work shows that you are not disabled; or
(3) Your failure to give us information we need or do what we ask. The advance notice will tell you what information we need and why we need it or what you have to do and why.
(c) What you should do if you receive an advance notice. If you agree with the advance notice, you do not need to take any action. If you desire further information or disagree with what we have told you, you should immediately write or telephone the State agency or the social security office that gave you the advance notice or you may visit any social security office. If you believe you are now disabled, you should tell us why. You may give us any additional or new information, including reports from your doctors, hospitals, employers or others, that you believe we should have. You should send these as soon as possible to the local social security office or to the office that gave you the advance notice. We consider 10 days to be enough time for you to tell us, although we will allow you more time if you need it. You will have to ask for additional time beyond 10 days if you need it.
(d) When we will not give you advance notice. We will not give you advance notice when we determine that you are not disabled if—
(1) We recently told you that the information we have shows that you are not now disabled, that we were gathering more information, and that your benefits will stop; or
(2) We are stopping your benefits because you told us you are not now disabled; or
(3) We recently told you that continuing your benefits would probably cause us to overpay you and you asked us to stop your benefits.
§ 404.1596 Circumstances under which we may suspend and terminate your benefits before we make a determination.
(a) General. Under some circumstances, we may stop your benefits before we make a determination. Generally, we do this when the information we have clearly shows you are not now disabled but we cannot determine when your disability ended. These situations are described in paragraph (b)(1) and other reasons are given in paragraph (b)(2) of this section. We refer to this as a suspension of benefits. Your benefits, as well as those of your dependents (regardless of where they receive their benefits), may be suspended. When we do this we will give you advance notice. (See § 404.1595.) We will contact your spouse and children if they are receiving benefits on your Social Security number, and the benefits are being mailed to an address different from your own.
(b) When we will suspend your benefits —
(1) You are not now disabled. We will suspend your benefits if the information we have clearly shows that you are not disabled and we will be unable to complete a determination soon enough to prevent us from paying you more monthly benefits than you are entitled to. This may occur when—
(i) New medical or other information clearly shows that you are able to do substantial gainful activity and your benefits should have stopped more than 2 months ago;
(ii) You completed a 9-month period of trial work more than 2 months ago and you are still working;
(iii) At the time you filed for benefits your condition was expected to improve and you were expected to be able to return to work. You subsequently did return to work more than 2 months ago with no significant medical restrictions; or
(iv) You are not entitled to a trial work period and you are working.
(2) Other reasons. We will also suspend your benefits if—
(i) You have failed to respond to our request for additional medical or other evidence and we are satisfied that you received our request and our records show that you should be able to respond; or
(ii) We are unable to locate you and your checks have been returned by the Post Office as undeliverable.
(c) When we will not suspend your cash benefits. We will not suspend your cash benefits if—
(1) You have become disabled by another impairment; or
(2) Even though your impairment is no longer disabling,
(i) You are participating in an appropriate program of vocational rehabilitation services, employment services, or other support services, as described in § 404.327(a) and (b);
(ii) You began participating in the program before the date your disability ended; and
(iii) We have determined under § 404.328 that your completion of the program, or your continuation in the program for a specified period of time, will increase the likelihood that you will not have to return to the disability benefit rolls.
(d) When the suspension is effective. We will suspend your benefits effective with the month in which it is determined in accordance with paragraph (b)(2)(i) of this section that your disability benefits should stop due to your failure, without good cause (see § 404.911), to comply with our request for necessary information for your continuing disability review. This review is to determine whether or not you continue to meet the disability requirements of the law. When we have received the information, we will reinstate your benefits for any previous month for which they are otherwise payable, and continue with the CDR process.
(e) When we will terminate your benefits. We will terminate your benefits following 12 consecutive months of benefit suspension because you did not comply with our request for information in accordance with paragraph (b)(2)(i) of this section. We will count the 12-month suspension period from the start of the first month that you stopped receiving benefits (see paragraph (d) of this section). This termination is effective with the start of the 13th month after the suspension began because you failed to cooperate.
[45 FR 55584, Aug. 20, 1980, as amended at 47 FR 31543, July 21, 1982; 47 FR 52693, Nov. 23, 1982; 51 FR 17617, May 14, 1986; 68 FR 40123, July 7, 2003; 70 FR 36507, June 24, 2005; 71 FR 60822, Oct. 17, 2006]
§ 404.1597 After we make a determination that you are not now disabled.
(a) General. If we determine that you do not meet the disability requirements of the law, your benefits generally will stop. We will send you a formal written notice telling you why we believe you are not disabled and when your benefits should stop. If your spouse and children are receiving benefits on your social security number, we will also stop their benefits and tell them why. The notices will explain your right to reconsideration if you disagree with our determination. However, your benefits may continue even though your impairment is no longer disabling, if you are participating in an appropriate program of vocational rehabilitation services, employment services, or other support services (see § 404.327). You must have started participating in the program before the date your disability ended. In addition, we must have determined that your completion of the program, or your continuation in the program for a specified period of time, will increase the likelihood that you will not have to return to the disability benefit rolls. (See §§ 404.316(c), 404.328, 404.337(c), 404.352(d), and 404.1586(g).) You may still appeal our determination that you are not disabled even though your benefits are continuing because of your participation in an appropriate program of vocational rehabilitation services, employment services, or other support services. You may also appeal a determination that your completion of the program, or your continuation in the program for a specified period of time, will not increase the likelihood that you will not have to return to the disability benefit rolls and, therefore, you are not entitled to continue to receive benefits.
(b) If we make a determination that your physical or mental impairment(s) has ceased, did not exist, or is no longer disabling (Medical Cessation Determination). If we make a determination that the physical or mental impairment(s) on the basis of which benefits were payable has ceased, did not exist, or is no longer disabling (a medical cessation determination), your benefits will stop. As described in paragraph (a) of this section, you will receive a written notice explaining this determination and the month your benefits will stop. The written notice will also explain your right to appeal if you disagree with our determination and your right to request that your benefits and the benefits, if any, of your spouse or children, be continued under § 404.1597a. For the purpose of this section, benefits means disability cash payments and/or Medicare, if applicable. The continued benefit provisions of this section do not apply to an initial determination on an application for disability benefits, or to a determination that you were disabled only for a specified period of time.
[47 FR 31544, July 21, 1982, as amended at 51 FR 17618, May 14, 1986; 53 FR 29020, Aug. 2, 1988; 53 FR 39015, Oct. 4, 1988; 70 FR 36507, June 24, 2005]
§ 404.1597a Continued benefits pending appeal of a medical cessation determination.
(a) General. If we determine that you are not entitled to benefits because the physical or mental impairment(s) on the basis of which such benefits were payable is found to have ceased, not to have existed, or to no longer be disabling, and you appeal that determination, you may choose to have your benefits continued pending reconsideration and/or a hearing before an administrative law judge on the disability cessation determination. For the purpose of this entire section, the election of continued benefits means the election of disability cash payments and/or Medicare, if applicable. You can also choose to have the benefits continued for anyone else receiving benefits based on your wages and self-employment income (and anyone else receiving benefits because of your entitlement to benefits based on disability). If you appeal a medical cessation under both title II and title XVI (a concurrent case), the title II claim will be handled in accordance with title II regulations while the title XVI claim will be handled in accordance with the title XVI regulations.
(b) When the provisions of this section are available.
(1) Benefits may be continued under this section only if the determination that your physical or mental impairment(s) has ceased, has never existed, or is no longer disabling is made on or after January 12, 1983 (or before January 12, 1983, and a timely request for reconsideration or a hearing before an administrative law judge is pending on that date).
(2) Benefits may be continued under this section only for months beginning with January 1983, or the first month for which benefits are no longer otherwise payable following our determination that your physical or mental impairment(s) has ceased, has never existed, or is no longer disabling, whichever is later.
(3) Continued payment of benefits under this section will stop effective with the earlier of:
(i) The month before the month in which an administrative law judge's hearing decision finds that your physical or mental impairment(s) has ceased, has never existed, or is no longer disabling or the month before the month of a new administrative law judge decision (or final action by the Appeals Council on the administrative law judge's recommended decision) if your case was sent back to an administrative law judge for further action; or
(ii) The month before the month no timely request for a reconsideration or a hearing before an administrative law judge is pending. These continued benefits may be stopped or adjusted because of certain events (such as work and earnings or receipt of worker's compensation) which occur while you are receiving these continued benefits and affect your right to receive continued benefits.
(c) Continuation of benefits for anyone else pending your appeal.
(1) When you file a request for reconsideration or hearing before an administrative law judge on our determination that your physical or mental impairment(s) has ceased, has never existed, or is no longer disabling, or your case has been sent back (remanded) to an administrative law judge for further action, you may also choose to have benefits continue for anyone else who is receiving benefits based on your wages and self-employment income (and for anyone else receiving benefits because of your entitlement to benefits based on disability), pending the outcome of your appeal.
(2) If anyone else is receiving benefits based on your wages and self-employment income, we will notify him or her of the right to choose to have his or her benefits continue pending the outcome of your appeal. Such benefits can be continued for the time period in paragraph (b) of this section only if he or she chooses to have benefits continued and you also choose to have his or her benefits continued.
(d) Statement of choice. When you or another party request reconsideration under § 404.908(a) or a hearing before an administrative law judge under § 404.932(a) on our determination that your physical or mental impairment(s) has ceased, has never existed, or is no longer disabling, or if your case is sent back (remanded) to an administrative law judge for further action, we will explain your right to receive continued benefits and ask you to complete a statement specifying which benefits you wish to have continued pending the outcome of the reconsideration or hearing before an administrative law judge. You may elect to receive only Medicare benefits during appeal even if you do not want to receive continued disability benefits. If anyone else is receiving benefits based on your wages and self-employment income (or because of your entitlement to benefits based on disability), we will ask you to complete a statement specifying which benefits you wish to have continued for them, pending the outcome of the request for reconsideration or hearing before an administrative law judge. If you request appeal but you do not want to receive continued benefits, we will ask you to complete a statement declining continued benefits indicating that you do not want to have your benefits and those of your family, if any, continued during the appeal.
(e) Your spouse's or children's statement of choice. If you request, in accordance with paragraph (d) of this section, that benefits also be continued for anyone who had been receiving benefits based on your wages and self-employment, we will send them a written notice. The notice will explain their rights and ask them to complete a statement either declining continued benefits, or specifying which benefits they wish to have continued, pending the outcome of the request for reconsideration or a hearing before an administrative law judge.
(f) What you must do to receive continued benefits pending notice of our reconsideration determination.
(1) If you want to receive continued benefits pending the outcome of your request for reconsideration, you must request reconsideration and continuation of benefits no later than 10 days after the date you receive the notice of our initial determination that your physical or mental impairment(s) has ceased, has never existed, or is no longer disabling. Reconsideration must be requested as provided in § 404.909, and you must request continued benefits using a statement in accordance with paragraph (d) of this section.
(2) If you fail to request reconsideration and continued benefits within the 10-day period required by paragraph (f)(1) of this section, but later ask that we continue your benefits pending a reconsidered determination, we will use the rules in § 404.911 to determine whether good cause exists for your failing to request benefit continuation within 10 days after receipt of the notice of the initial cessation determination. If you request continued benefits after the 10-day period, we will consider the request to be timely and will pay continued benefits only if good cause for delay is established.
(g) What you must do to receive continued benefits pending an administrative law judge's decision.
(1) To receive continued benefits pending an administrative law judge's decision on our reconsideration determination, you must request a hearing and continuation of benefits no later than 10 days after the date you receive the notice of our reconsideration determination that your physical or mental impairment(s) has ceased, has never existed, or is no longer disabling. A hearing must be requested as provided in § 404.933, and you must request continued benefits using a statement in accordance with paragraph (d) of this section.
(2) If you request continued benefits pending an administrative law judge's decision but did not request continued benefits while we were reconsidering the initial cessation determination, your benefits will begin effective the month of the reconsideration determination.
(3) If you fail to request continued payment of benefits within the 10-day period required by paragraph (g)(1) of this section, but you later ask that we continue your benefits pending an administrative law judge's decision on our reconsidered determination, we will use the rules as provided in § 404.911 to determine whether good cause exists for your failing to request benefit continuation within 10 days after receipt of the reconsideration determination. If you request continued benefits after the 10-day period, we will consider the request to be timely and will pay continued benefits only if good cause for delay is established.
(h) What anyone else must do to receive continued benefits pending our reconsideration determination or an administrative law judge's decision.
(1) When you or another party (see §§ 404.908(a) and 404.932(a)) request a reconsideration or a hearing before an administrative law judge on our medical cessation determination or when your case is sent back (remanded) to an administrative law judge for further action, you may choose to have benefits continue for anyone else who is receiving benefits based on your wages and self-employment income. An eligible individual must also choose whether or not to have his or her benefits continue pending your appeal by completing a separate statement of election as described in paragraph (e) of this section.
(2) He or she must request continuation of benefits no later than 10 days after the date he or she receives notice of termination of benefits. He or she will then receive continued benefits beginning with the later of January 1983, or the first month for which benefits are no longer otherwise payable following our initial or reconsideration determination that your physical or mental impairment(s) has ceased, has never existed, or is no longer disabling. Continued benefits will continue until the earlier of:
(i) The month before the month in which an administrative law judge's hearing decision finds that your physical or mental impairment(s) has ceased, has never existed, or is no longer disabling or the month before the month of the new administrative law judge decision (or final action is taken by the Appeals Council on the administrative law judge's recommended decision) if your case was sent back to an administrative law judge for further action; or
(ii) The month before the month no timely request for a reconsideration or a hearing before an administrative law judge is pending. These continued benefits may be stopped or adjusted because of certain events (such as work and earnings or payment of worker's compensation) which occur while an eligible individual is receiving continued benefits and affect his or her right to receive continued benefits.
(3) If he or she fails to request continuation of benefits within the 10-day period required by this paragraph, but requests continuation of benefits at a later date, we will use the rules as provided in § 404.911 to determine whether good cause exists for his or her failure to request continuation of benefits within 10 days after receipt of the notice of termination of his or her benefits. His or her late request will be considered to be timely and we will pay him or her continued benefits only if good cause for delay is established.
(4) If you choose not to have benefits continued for anyone else who is receiving benefits based on your wages and self-employment income, pending the appeal on our determination, we will not continue benefits to him or her.
(i) What you must do when your case is remanded to an administrative law judge. If we send back (remand) your case to an administrative law judge for further action under the rules provided in § 404.977, and the administrative law judge's decision or dismissal order issued on your medical cessation appeal is vacated and is no longer in effect, continued benefits are payable pending a new decision by the administrative law judge or final action is taken by the Appeals Council on the administrative law judge's recommended decision.
(1) If you (and anyone else receiving benefits based on your wages and self-employment income or because of your disability) previously elected to receive continued benefits pending the administrative law judge's decision, we will automatically start these same continued benefits again. We will send you a notice telling you this, and that you do not have to do anything to have these same benefits continued until the month before the month the new decision of order of dismissal is issued by the administrative law judge or until the month before the month the Appeals Council takes final action on the administrative law judge's recommended decision. These benefits will begin again with the first month of nonpayment based on the prior administrative law judge hearing decision or dismissal order. Our notice explaining reinstatement of continued benefits will also tell you to report to us any changes or events that affect your receipt of benefits.
(2) After we automatically reinstate your continued benefits as described in paragraph (h)(1) of this section, we will contact you to determine if any adjustment is required to the amount of continued benefits payable due to events that affect the right to receive benefits involving you, your spouse and/or children. If you have returned to work, we will request additional information about this work activity. If you are working, your continued benefits will not be stopped while your appeal of the medical cessation of disability is still pending unless you have completed a trial work period and are engaging in substantial gainful activity. In this event, we will suspend your continued benefits. If any other changes have occurred which would require a reduction in benefit amounts, or nonpayment of benefits, we will send an advance notice to advise of any adverse change before the adjustment action is taken. The notice will also advise you of the right to explain why these benefits should not be adjusted or stopped. You will also receive a written notice of our determination. The notice will also explain your right to reconsideration if you disagree with this determination.
(3) If the final decision on your appeal of your medical cessation is a favorable one, we will send you a written notice in which we will advise you of your right to benefits, if any, before you engaged in substantial gainful activity and to reentitlement should you stop performing substantial gainful activity. If you disagree with our determination, you will have the right to appeal this decision.
(4) If the final decision on your appeal of your medical cessation is an unfavorable one (the cessation is affirmed), you will also be sent a written notice advising you of our determination, and your right to appeal if you think we are wrong.
(5) If you (or the others receiving benefits based on your wages and self-employment income or because of your disability) did not previously elect to have benefits continued pending an administrative law judge decision, and you now want to elect continued benefits, you must request to do so no later than 10 days after you receive our notice telling you about continued benefits. If you fail to request continued benefits within the 10-day period required by paragraph (f)(1) of this section, but later ask that we continue your benefits pending an administrative law judge remand decision, we will use the rules in § 404.911 to determine whether good cause exists for your failing to request benefit continuation within 10 days after receipt of the notice telling you about benefit continuation. We will consider the request to be timely and will pay continued benefits only if good cause for delay is established. If you make this new election, benefits may begin with the month of the order sending (remanding) your case back to the administrative law judge. Before we begin to pay you continued benefits as described in paragraph (h)(1) of this section we will contact you to determine if any adjustment is required to the amount of continued benefits payable due to events which may affect your right to benefits. If you have returned to work, we will request additional information about this work activity. If you are working, continued benefits may be started and will not be stopped because of your work while your appeal of the medical cessation of your disability is still pending unless you have completed a trial work period and are engaging in substantial gainful activity. If any changes have occurred which establish a basis for not paying continued benefits or a reduction in benefit amount, we will send you a notice explaining the adjustment or the reason why we cannot pay continued benefits. The notice will also explain your right to reconsideration if you disagree with this determination. If the final decision on your appeal of your medical cessation is a favorable one, we will send you a written notice in which we will advise you of your right to benefits, if any, before you engaged in substantial gainful activity and to reentitlement should you stop performing substantial gainful activity. If you disagree with our determination, you will have the right to appeal this decision. If the final decision on your appeal of your medical cessation is an unfavorable one (the cessation is affirmed), you will also be sent a written notice advising you of our determination, and your right to appeal if you think we are wrong.
(6) If a court orders that your case be sent back to us (remanded) and your case is sent to an administrative law judge for further action under the rules provided in § 404.983, the administrative law judge's decision or dismissal order on your medical cessation appeal is vacated and is no longer in effect. Continued benefits are payable to you and anyone else receiving benefits based on your wages and self-employment income or because of your disability pending a new decision by the administrative law judge or final action is taken by the Appeals Council on the administrative law judge's recommended decision. In these court-remanded cases reaching the administrative law judge, we will follow the same rules provided in paragraphs (i) (1), (2), (3), (4) and (5) of this section.
(j) Responsibility to pay back continued benefits.
(1) If the final decision of the Commissioner affirms the determination that you are not entitled to benefits, you will be asked to pay back any continued benefits you receive. However, as described in the overpayment recovery and waiver provisions of subpart F of this part, you will have the right to ask that you not be required to pay back the benefits. You will not be asked to pay back any Medicare benefits you received during the appeal.
(2) Anyone else receiving benefits based on your wages and self-employment income (or because of your disability) will be asked to pay back any continued benefits he or she received if the determination that your physical or mental impairment(s) has ceased, has never existed, or is no longer disabling, is not changed by the final decision of the Commissioner. However, he or she will have the right to ask that he or she not be required to pay them back, as described in the overpayment recovery and waiver provisions of subpart F of this part. He or she will not be asked to pay back any Medicare benefits he or she received during the appeal.
(3) Waiver of recovery of an overpayment resulting from the continued benefits paid to you or anyone else receiving benefits based on your wages and self-employment income (or because of your disability) may be considered as long as the determination was appealed in good faith. It will be assumed that such appeal is made in good faith and, therefore, any overpaid individual has the right to waiver consideration unless such individual fails to cooperate in connection with the appeal, e.g., if the individual fails (without good reason) to give us medical or other evidence we request, or to go for a physical or mental examination when requested by us, in connection with the appeal. In determining whether an individual has good cause for failure to cooperate and, thus, whether an appeal was made in good faith, we will take into account any physical, mental, educational, or linguistic limitations (including any lack of facility with the English language) the individual may have which may have caused the individual's failure to cooperate.
[53 FR 29020, Aug. 2, 1988; 53 FR 39015, Oct. 4, 1988, as amended at 57 FR 1383, Jan. 14, 1992; 59 FR 1635, Jan. 12, 1994; 62 FR 38451, July 18, 1997; 65 FR 16814, Mar. 30, 2000]
§ 404.1598 If you become disabled by another impairment(s).
If a new severe impairment(s) begins in or before the month in which your last impairment(s) ends, we will find that your disability is continuing. The new impairment(s) need not be expected to last 12 months or to result in death, but it must be severe enough to keep you from doing substantial gainful activity, or severe enough so that you are still disabled under § 404.1594.
[50 FR 50136, Dec. 6, 1985]
§ 404.1599 Work incentive experiments and rehabilitation demonstration projects in the disability program.
(a) Authority and purpose. Section 505(a) of the Social Security Disability Amendments of 1980, Pub. L. 96-265, directs the Commissioner to develop and conduct experiments and demonstration projects designed to provide more cost-effective ways of encouraging disabled beneficiaries to return to work and leave benefit rolls. These experiments and demonstration projects will test the advantages and disadvantages of altering certain limitations and conditions that apply to title II disabled beneficiaries. The objective of all work incentive experiments or rehabilitation demonstrations is to determine whether the alternative requirements will save Trust Fund monies or otherwise improve the administration of the disability program established under title II of the Act.
(b) Altering benefit requirements, limitations or conditions. Notwithstanding any other provision of this part, the Commissioner may waive compliance with the entitlement and payment requirements for disabled beneficiaries to carry our experiments and demonstration projects in the title II disability program. The projects involve altering certain limitations and conditions that currently apply to applicants and beneficiaries to test their effect on the program.
(c) Applicability and scope —
(1) Participants and nonparticipants. If you are selected to participate in an experiment or demonstration project, we may temporarily set aside one or more of the current benefit entitlement or payment requirements, limitations or conditions and apply alternative provisions to you. We may also modify current methods of administering the Act as part of a project and apply alternative procedures or policies to you. The alternative provisions or methods of administration used in the projects will not disadvantage you in contrast to current provisions, procedures or policies. If you are not selected to participate in the experiments or demonstration projects (or if you are placed in a control group which is not subject to alternative requirements and methods) we will continue to apply to you the current benefit entitlement and payment requirements, limitations and conditions and methods of administration in the title II disability program.
(2) Alternative provisions or methods of administration. The alternative provisions or methods of administration that apply to you in an experiment or demonstration project may include (but are not limited to) one or more of the following:
(i) Reducing your benefits (instead of not paying) on the basis of the amount of your earnings in excess of the SGA amount;
(ii) Extending your benefit eligibility period that follows 9 months of trial work, perhaps coupled with benefit reductions related to your earnings;
(iii) Extending your Medicare benefits if you are severely impaired and return to work even though you may not be entitled to monthly cash benefits;
(iv) Altering the 24-month waiting period for Medicare entitlement; and
(v) Stimulating new forms of rehabilitation.
(d) Selection of participants. We will select a probability sample of participants for the work incentive experiments and demonstration projects from newly awarded beneficiaries who meet certain pre-selection criteria (for example, individuals who are likely to be able to do substantial work despite continuing severe impairments). These criteria are designed to provide larger subsamples of beneficiaries who are not likely either to recover medically or die. Participants may also be selected from persons who have been receiving DI benefits for 6 months or more at the time of selection.
(e) Duration of experiments and demonstration projects. A notice describing each experiment or demonstration project will be published in the Federal Register before each experiment or project is placed in operation. The work incentive experiments and rehabilitation demonstrations will be activated in 1982. A final report on the results of the experiments and projects is to be completed and transmitted to Congress by June 9, 1993. However, the authority for the experiments and demonstration projects will not terminate at that time. Some of the alternative provisions or methods of administration may continue to apply to participants in an experiment or demonstration project beyond that date in order to assure the validity of the research. Each experiment and demonstration project will have a termination date (up to 10 years from the start of the experiment or demonstration project).
[48 FR 7575, Feb. 23, 1983, as amended at 52 FR 37605, Oct. 8, 1987; 55 FR 51687, Dec. 17, 1990; 62 FR 38451, July 18, 1997]
Appendix 1 to Subpart P of Part 404 - Listing of Impairments
The body system listings in parts A and B of the Listing of Impairments will no longer be effective on the following dates unless extended by the Commissioner or revised and promulgated again.
1. Low Birth Weight and Failure to Thrive (100.00): August 12, 2022.
2. Musculoskeletal Disorders (1.00 and 101.00): April 2, 2026.
3. Special Senses and Speech (2.00 and 102.00): June 3, 2022.
4. Respiratory Disorders (3.00 and 103.00): December 10, 2021
5. Cardiovascular System (4.00 and 104.00): February 4, 2022.
6. Digestive System (5.00 and 105.00): February 4, 2022.
7. Genitourinary Disorders (6.00 and 106.00): December 10, 2021.
8. Hematological Disorders (7.00 and 107.00): June 3, 2022.
9. Skin Disorders (8.00 and 108.00): February 4, 2022.
10. Endocrine Disorders (9.00 and 109.00): August 12, 2022.
11. Congenital Disorders That Affect Multiple Body Systems (10.00 and 110.00): June 3, 2022.
12. Neurological Disorders (11.00 and 111.00): September 29, 2025.
13. Mental Disorders (12.00 and 112.00): January 17, 2022.
14. Cancer (Malignant Neoplastic Diseases) (13.00 and 113.00): August 12, 2022.
15. Immune System Disorders (14.00 and 114.00): February 4, 2022.
Part A
Criteria applicable to individuals age 18 and over and to children under age 18 where criteria are appropriate.
Sec.
1.00 Musculoskeletal Disorders
2.00 Special Senses and Speech.
3.00 Respiratory Disorders.
4.00 Cardiovascular System.
5.00 Digestive System.
6.00 Genitourinary Disorders.
7.00 Hematological Disorders.
8.00 Skin Disorders.
9.00 Endocrine Disorders.
10.00 Congenital Disorders That Affect Multiple Body Systems
11.00 Neurological Disorders.
12.00 Mental Disorders.
13.00 Cancer (Malignant Neoplastic Diseases).
14.00 Immune System Disorders.
1.00 Musculoskeletal Disorders
A. Which musculoskeletal disorders do we evaluate under these listings?
1. We evaluate disorders of the skeletal spine (vertebral column) or of the upper or lower extremities that affect musculoskeletal functioning under these listings. We use the term “skeletal” when we are referring to the structure of the bony skeleton. The skeletal spine refers to the bony structures, ligaments, and discs making up the spine. We refer to the skeletal spine in some musculoskeletal listings to differentiate it from the neurological spine (see 1.00B1). Musculoskeletal disorders may be congenital or acquired, and may include deformities, amputations, or other abnormalities. These disorders may involve the bones or major joints; or the tendons, ligaments, muscles, or other soft tissues.
2. We evaluate soft tissue injuries (including burns) or abnormalities that are under continuing surgical management (see 1.00O1). The injuries or abnormalities may affect any part of the body, including the face and skull.
3. We evaluate curvatures of the skeletal spine that affect musculoskeletal functioning under 1.15. If a curvature of the skeletal spine is under continuing surgical management (see 1.00O1), we will evaluate it under 1.21 using our rules for determining medical equivalence. See §§ 404.1526 and 416.926 of this chapter.
B. Which related disorders do we evaluate under other listings?
1. We evaluate a disorder or injury of the skeletal spine that results in damage to, and neurological dysfunction of, the spinal cord and its associated nerves (for example, paraplegia or quadriplegia) under the listings in 11.00.
2. We evaluate inflammatory arthritis (for example, rheumatoid arthritis) under the listings in 14.00.
3. We evaluate curvatures of the skeletal spine that interfere with your ability to breathe under the listings in 3.00, impair myocardial function under the listings in 4.00, or result in social withdrawal or depression under the listings in 12.00.
4. We evaluate non-healing or pathological fractures due to cancer, whether it is a primary site or metastases, under the listings in 13.00.
5. We evaluate the leg pain associated with peripheral vascular claudication and foot ulceration associated with peripheral arterial disease under the listings in 4.00.
6. We evaluate burns that do not require continuing surgical management under the listings in 8.00.
C. What evidence do we need to evaluate your musculoskeletal disorder?
1. General. We need objective medical evidence from an acceptable medical source to establish that you have a medically determinable musculoskeletal disorder. We also need evidence from both medical and nonmedical sources, who can describe how you function, to assess the severity and duration of your musculoskeletal disorder. We will determine the extent and kinds of evidence we need from medical and nonmedical sources based on the individual facts about your disorder. For our basic rules on evidence, see §§ 404.1512, 404.1513, 404.1520b, 416.912, 416.913, and 416.920b of this chapter. For our rules on evidence about your symptoms, see §§ 404.1529 and 416.929 of this chapter.
2. Physical examination report(s). In the report(s) of your physical examination, we require a medical source's detailed description of the orthopedic, neurologic, or other objective clinical findings appropriate to your specific musculoskeletal disorder from his or her direct observations during your physical examination. We will not accept a report of your statements about your symptoms and limitations in place of the medical source's report of objective clinical findings. We will not use findings on imaging or other diagnostic tests (see 1.00C3) as a substitute for findings on physical examination.
a. When the medical source reports that a clinical test sign(s) is positive, unless we have evidence to the contrary, we will assume that he or she performed the test properly and accept the medical source's interpretation of the test. For example, we will assume a straight-leg raising test was conducted properly (that is, in sitting and supine positions), even if the medical source does not specify the positions in which the test was performed.
b. If you use an assistive device (see 1.00C6), the report must support the medical need for the device.
c. If your musculoskeletal disorder causes a reduction in muscle strength, the report must document measurement of the strength of the muscle(s) in question. The measurement should be based on a muscle strength grading system that is considered medically acceptable based on your age and impairments. For example, a grading system of 0 to 5, with 0 indicating complete loss of strength and 5 indicating maximum strength or equivalent medically acceptable scale (see Table 1). Reduction in muscle strength is demonstrated by evidence that your muscle strength is less than active range of motion (ROM) against gravity with maximum resistance. If the reduction in muscle strength involves one or both of your hands, the report must also document measurements of grip and pinch strength.
Table 1 - Grading System of Muscle Function
| Grade | Function of the muscle |
|---|---|
| 0 - None | No visible or palpable contraction. |
| 1 - Trace | Visible or palpable contraction with no motion. |
| 2 - Poor | Active ROM with gravity eliminated. |
| 3 - Fair | Active ROM against gravity only, without resistance. |
| 4 - Good | Active ROM against gravity, moderate resistance. |
| 5 - Normal | Active ROM against gravity, maximum resistance. |
3. Imaging and other diagnostic tests.
a. Imaging refers to medical imaging techniques, such as x-ray, computed tomography (CT), magnetic resonance imaging (MRI), and radionuclide scanning. For the purpose of these listings, the imaging must be consistent with the prevailing state of medical knowledge and clinical practice as the proper technique to support the evaluation of the disorder.
b. Findings on imaging must have lasted, or be expected to last, for a continuous period of at least 12 months.
c. Imaging and other diagnostic tests can provide evidence of physical abnormalities; however, these abnormalities may correlate poorly with your symptoms, including pain, or with your musculoskeletal functioning. Accordingly, we will not use findings on imaging or other diagnostic tests as a substitute for findings on physical examination about your ability to function, nor can we infer severity or functional limitations based solely on such tests.
d. For our rules on purchasing imaging and other diagnostic tests, see §§ 404.1519k, 404.1519m, 416.919k, and 416.919m of this chapter.
4. Operative reports. If you have had a surgical procedure, we need a copy of the operative report, including details of the findings at surgery and information about any medical complications that may have occurred. If we do not have the operative report, we need confirmatory evidence of the surgical procedure from a medical source (for example, detailed follow-up reports or notations in the medical records concerning the surgical procedure in your medical history).
5. Effects of treatment.
a. General. Treatments for musculoskeletal disorders may have beneficial or adverse effects, and responses to treatment vary from person to person. We will evaluate all of the effects of treatment (including surgical treatment, medications, and therapy) on the symptoms, signs, and laboratory findings of your musculoskeletal disorder, and on your musculoskeletal functioning.
b. Response to treatment. To evaluate your musculoskeletal functioning in response to treatment, we need the following: A description, including the frequency of the administration, of your medications; the type and frequency of therapy you receive; and a description of your response to treatment and any complications you experience related to your musculoskeletal disorder. The effects of treatment may be temporary or long-term. We need information over a sufficient period to determine the effects of treatment on your current musculoskeletal functioning and permit reasonable projections about your future functioning. We will determine the amount of time that constitutes a sufficient period in consultation with a medical consultant on a case-by-case basis. In some cases, we will need additional evidence to make an assessment about your response to treatment. Your musculoskeletal disorder may meet or medically equal one of these listings regardless of whether you were prescribed opioid medication, or whether you were prescribed opioid medication and did not follow this prescribed treatment.
6. Assistive devices.
a. General. An assistive device, for the purposes of these listings, is any device that you use to improve your stability, dexterity, or mobility. An assistive device can be worn (see 1.00C6b and 1.00C6c), hand-held (see 1.00C6d), or used in a seated position (see 1.00C6e). When we use the phrase “documented medical need,” we mean that there is evidence from a medical source that supports your medical need for an assistive device (see 1.00C2b) for a continuous period of at least 12 months (see 1.00C6a). This evidence must describe any limitation(s) in your upper or lower extremity functioning and the circumstances for which you need to use the assistive device. We do not require that you have a specific prescription for the assistive device.
b. Prosthesis(es). A prosthesis is a wearable device, such as an artificial limb, that takes the place of an absent body part. If you have a prosthesis(es), we need evidence from a medical source documenting your ability to walk, or perform fine and gross movements (see 1.00E4), with the prosthesis(es) in place. When amputation(s) involves one or both lower extremities, it is not necessary for the medical source to evaluate your ability to walk without the prosthesis(es) in place. If you cannot use your prosthesis(es) due to complications affecting your residual limb(s), we need evidence from a medical source documenting the condition of your residual limb(s) and the medical basis for your inability to use the device(s).
c. Orthosis(es). An orthosis is a wearable device, such as a brace, that prevents or corrects a dysfunction or deformity by aligning or supporting the affected body part. If you have an orthosis(es), we need evidence from a medical source documenting your ability to walk, or perform fine and gross movements (see 1.00E4), with the orthosis(es) in place. If you cannot use your orthosis(es), we need evidence from a medical source documenting the medical basis for your inability to use the device(s).
d. Hand-held assistive devices. Hand-held assistive devices include walkers, canes, or crutches, which you hold onto with your hand(s) to support or aid you in walking. When you use a one-handed, hand-held assistive device (such as a cane) with one upper extremity to walk and you cannot use your other upper extremity for fine or gross movements (see 1.00E4), the need for the assistive device limits the use of both upper extremities. If you use a hand-held assistive device, we need evidence from a medical source describing how you walk with the device.
e. Wheeled and seated mobility devices. Wheeled and seated mobility devices are assistive devices that you use in a seated position, such as manual wheelchairs, motorized wheelchairs, rollators, and power operated vehicles. If you use a wheeled and seated mobility device, we need evidence from a medical source describing the type of wheeled and seated mobility device that you use and how you use the assistive device including any customizations or modifications to the assistive device itself or for your use of the assistive device. For example, if you use a wheelchair that typically requires the use of both hands but has been customized for your use with one hand, then we will evaluate your use of the assistive device using the criteria in 1.00E3b and not 1.00E3a.
(i) Wheeled and seated mobility devices involving the use of both hands. Some wheeled and seated mobility devices involve the use of both hands to use the assistive device (for example, most manual wheelchairs). If you use a wheeled and seated mobility device that involves the use of both hands, then the need for the assistive device limits the use of both upper extremities.
(ii) Wheeled and seated devices involving the use of one hand. Some wheeled and seated mobility devices involve the use of one hand to use the assistive device (for example, most motorized wheelchairs). If you use a wheeled and seated mobility device that involves the use of one upper extremity and you cannot use your other upper extremity for fine or gross movements (see 1.00E4), then the need for the assistive device limits the use of both upper extremities.
7. Longitudinal evidence.
a. The term pandemic period as used in 1.00C7c means the period beginning on April 2, 2021, and ending on the date that is 6 months after the effective date of a determination by the Secretary of Health and Human Services under section 319 of the Public Health Service Act, 42 U.S.C. 247d, that the national public health emergency resulting from the COVID-19 pandemic no longer exists.
b. We generally need a longitudinal medical record to assess the severity and duration of your musculoskeletal disorder because the severity of symptoms, signs, and laboratory findings related to most musculoskeletal disorders may improve over time or respond to treatment. Evidence over an extended period will show whether your musculoskeletal functioning is improving, worsening, or unchanging.
c. For 1.15, 1.16, 1.17, 1.18, 1.20C, 1.20D, 1.22, and 1.23, all of the required criteria must be present simultaneously, or within a close proximity of time, to satisfy the level of severity needed to meet the listing. The phrase “within a close proximity of time” means that all of the relevant criteria must appear in the medical record within a consecutive 4-month period, except for claims determined or decided during the pandemic period. For claims determined or decided during the pandemic period, all of the relevant criteria must appear in the medical record within a consecutive 12-month period. When the criterion is imaging, we mean that we could reasonably expect the findings on imaging to have been present at the date of impairment or date of onset. For listings that use the word “and” to link the elements of the required criteria, the medical record must establish the simultaneous presence, or presence within a close proximity of time, of all the required medical criteria. Once this level of severity is established, the medical record must also show that this level of severity has continued, or is expected to continue, for a continuous period of at least 12 months.
8. Surgical treatment and physical therapy. For some musculoskeletal disorders, a medical source may recommend surgery or physical therapy (PT). If you have not yet had the recommended surgery or PT, we will not assume that these interventions will resolve your disorder or improve your functioning. We will assess each case on an individual basis. Depending on your response to treatment, or your medical sources' treatment plans, we may defer our findings regarding the effect of surgery or PT, until a sufficient period has passed to permit proper consideration or judgment about your future functioning. When necessary, we will follow the rules on following prescribed treatment in §§ 404.1530 and 416.930 of this chapter, including consideration of your reasons for failure to follow prescribed treatment.
D. How do we consider symptoms, including pain, under these listings?
1. Musculoskeletal disorders may cause pain or other symptoms; however, your statements about your pain or other symptoms will not alone establish that you are disabled. We will not substitute an alleged or a reported increase in the intensity of a symptom, such as pain, no matter how severe, for a medical sign or diagnostic finding present in the listing criteria. Pain is included as just one consideration in 1.15A, 1.16A, and 1.18A, but it is not required to satisfy the criteria in 1.15, 1.16, and 1.18.
2. To consider your symptom(s), we require objective medical evidence from an acceptable medical source showing the existence of a medically determinable musculoskeletal impairment that we could reasonably expect to produce the symptom(s). See §§ 404.1529 and 416.929 of this chapter for how we evaluate symptoms, including pain, related to your musculoskeletal disorder.
E. How do we use the functional criteria to evaluate your musculoskeletal disorder under these listings?
1. General. The functional criteria are based on impairment-related physical limitations in your ability to use both upper extremities, one or both lower extremities, or a combination of one upper and one lower extremity. The required impairment-related physical limitation of musculoskeletal functioning must have lasted, or be expected to last, for a continuous period of at least 12 months. We do not use the functional criteria in 1.20A, 1.20B, or 1.21.
2. Work environment. We use the relevant evidence that we have to evaluate your musculoskeletal functioning with respect to the work environment rather than the home environment. For example, an ability to walk independently at home without an assistive device does not, in and of itself, indicate an ability to walk without an assistive device in a work environment.
3. Functional criteria. A musculoskeletal disorder satisfies the functional criteria of a listing when the medical documentation shows the presence of at least one of the impairment-related limitations cited in the listing. The required impairment-related limitation of musculoskeletal functioning must be medically documented by one of the following:
a. A documented medical need (see 1.00C6a) for a walker, bilateral canes, or bilateral crutches (see 1.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 1.00C6e(i));
b. An inability to use one upper extremity to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 1.00E4), and a documented medical need (see 1.00C6a) for a one-handed, hand-held assistive device (see 1.00C6d) that requires the use of your other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 1.00C6e(ii));
c. An inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 1.00E4).
4. Fine and gross movements. Fine movements, for the purposes of these listings, involve use of your wrists, hands, and fingers; such movements include picking, pinching, manipulating, and fingering. Gross movements involve use of your shoulders, upper arms, forearms, and hands; such movements include handling, gripping, grasping, holding, turning, and reaching. Gross movements also include exertional abilities such as lifting, carrying, pushing, and pulling. Examples of performing fine and gross movements include, but are not limited to, taking care of personal hygiene, sorting and handling papers or files, and placing files in a file cabinet at or above waist level.
F. What do we consider when we evaluate disorders of the skeletal spine resulting in compromise of a nerve root(s) (1.15)?
1. General. We consider musculoskeletal disorders such as herniated nucleus pulposus, spinal osteoarthritis (spondylosis), vertebral slippage (spondylolisthesis), degenerative disc disease, facet arthritis, and vertebral fracture or dislocation. Spinal disorders may cause cervical or lumbar spine dysfunction when abnormalities of the skeletal spine compromise nerve roots of the cervical spine, a nerve root of the lumbar spine, or a nerve root of both cervical and lumbar spines. We consider spinal nerve disorders that originate in the nervous system (for example, spinal arachnoiditis), under the neurological disorders body system, 11.00.
2. Compromise of a nerve root(s). Compromise of a nerve root, sometimes referred to as “nerve root impingement,” is a phrase used when a physical object, such as a tumor, herniated disc, foreign body, or arthritic spur, is pushing on the nerve root as seen on imaging or during surgery. It can occur when a musculoskeletal disorder produces irritation, inflammation, or compression of the nerve root(s) as it exits the skeletal spine between the vertebrae. Related symptoms must be associated with, or follow the path of, the affected nerve root(s).
a. Compromise of unilateral nerve root of the cervical spine. Compromise of a nerve root as it exits the cervical spine between the vertebrae may affect the functioning of the associated upper extremity. The physical examination reproduces the related symptoms based on radicular signs and clinical tests appropriate to the specific cervical nerve root (for example, a positive Spurling test).
b. Compromise of bilateral nerve roots of the cervical spine. Although uncommon, if compromise of a nerve root occurs on both sides of the cervical spinal column, functioning of both upper extremities may be limited.
c. Compromise of a nerve root(s) of the lumbar spine. Compromise of a nerve root as it exits the lumbar spine between the vertebrae may limit the functioning of the associated lower extremity. The physical examination reproduces the related symptoms based on radicular signs and clinical tests. When a nerve root of the lumbar spine is compromised, we require a positive straight-leg raising test (also known as a Lasègue test) in both supine and sitting positions appropriate to the specific lumbar nerve root that is compromised.
G. What do we consider when we evaluate lumbar spinal stenosis resulting in compromise of the cauda equina (1.16)?
1. General. We consider how pain, sensory changes, and muscle weakness caused by compromise of the cauda equina due to lumbar spinal stenosis affect your functioning. The cauda equina is a bundle of nerve roots that descends from the lower part of the spinal cord. Lumbar spinal stenosis can compress the nerves of the cauda equina, causing sensory changes and muscle weakness that may affect your ability to stand or walk. Pain related to compromise of the cauda equina is nonradicular because it is not typically associated with a specific nerve root (as is radicular pain in the cervical or lumbar spine).
2. Compromise of the cauda equina due to lumbar spinal stenosis can affect your ability to walk or stand because of neurogenic claudication (also known as pseudoclaudication), a condition usually causing nonradicular pain that starts in the low back and radiates bilaterally (or less commonly, unilaterally) into the buttocks and lower extremities (or extremity). Extension of the lumbar spine, which occurs when you walk or stand, may provoke the pain of neurogenic claudication. The pain may be relieved by forward flexion of the lumbar spine or by sitting. In contrast, the leg pain associated with peripheral vascular claudication results from inadequate arterial blood flow to a lower extremity. It occurs repeatedly and consistently when a person walks a certain distance and is relieved when the person rests.
H. What do we consider when we evaluate reconstructive surgery or surgical arthrodesis of a major weight-bearing joint (1.17)?
1. General. We consider reconstructive surgery or surgical arthrodesis when an acceptable medical source(s) documents the surgical procedure(s) and associated medical treatments to restore function of, or eliminate motion in, the affected major weight-bearing joint. Reconstructive surgery may be done in a single procedure or a series of procedures directed toward the salvage or restoration of functional use of the affected joint.
2. Major weight-bearing joints are the hip, knee, and ankle-foot. The ankle and foot are considered together as one major joint.
3. Surgical arthrodesis is the artificial fusion of the bones that form a joint, essentially eliminating the joint.
I. What do we consider when we evaluate abnormality of a major joint(s) in any extremity (1.18)?
1. General. We consider musculoskeletal disorders that produce anatomical abnormalities of major joints of the extremities, which result in functional abnormalities in the upper or lower extremities (for example, osteoarthritis, chronic infections of bones and joints, and surgical arthrodesis of a joint). Abnormalities of the joints include ligamentous laxity or rupture, soft tissue contracture, or tendon rupture, and can cause muscle weakness of the affected joint(s).
a. An anatomical abnormality is one that is readily observable by a medical source during a physical examination (for example, subluxation or contracture), or is present on imaging (for example, joint space narrowing, bony destruction, ankylosis, or deformity).
b. A functional abnormality is abnormal motion or instability of the affected joint(s), including limitation of motion, excessive motion (hypermobility), movement outside the normal plane of motion for the joint (for example, lateral deviation), or fixation of the affected joint(s).
2. Major joint of an upper extremity refers to the shoulder, elbow, and wrist-hand. We consider the wrist and hand together as one major joint.
3. Major joint of a lower extremity refers to the hip, knee, and ankle-foot. We consider the ankle and hindfoot together as one major joint.
J. What do we consider when we evaluate pathologic fractures due to any cause (1.19)? We consider pathologic fractures of the bones in the skeletal spine, extremities, or other parts of the skeletal system. Pathologic fractures result from disorders that weaken the bones, making them vulnerable to breakage. Pathologic fractures may occur with osteoporosis, osteogenesis imperfecta or any other skeletal dysplasias, side effects of medications, and disorders of the endocrine or other body systems. Under 1.19, the fractures must have occurred on separate, distinct occasions, rather than multiple fractures occurring at the same time, but the fractures may affect the same bone(s) multiple times. There is no required time that must elapse between the fractures, but all three must occur within a 12-month period; for example, separate incidents may occur within hours or days of each other. We evaluate non-healing or complex traumatic fractures without accompanying pathology under 1.22 or 1.23.
K. What do we consider when we evaluate amputation due to any cause (1.20)?
1. General. We consider amputation (the full or partial loss or absence of any extremity) due to any cause including trauma, congenital abnormality or absence, surgery for treatment of conditions such as cancer or infection, or complications of peripheral vascular disease or diabetes mellitus.
2. Amputation of both upper extremities (1.20A). Under 1.20A, we consider upper extremity amputations that occur at any level at or above the wrists (carpal joints), up to and including disarticulation of the shoulder (glenohumeral) joint. If you have had both upper extremities amputated at any level at or above the wrists up to and including the shoulder, your impairment satisfies the duration requirement in §§ 404.1509 and 416.909 of this chapter. For amputations below the wrist, we will follow the rules described in 1.00S. We do not evaluate amputations below the wrist under 1.20A because the resulting limitation of function of the thumb(s), finger(s), or hand(s) will vary, depending on the extent of loss and corresponding effect on fine and gross movements.
3. Hemipelvectomy or hip disarticulation (1.20B). Under 1.20B, we consider hemipelvectomy, which involves amputation of an entire lower extremity through the sacroiliac joint, and hip disarticulation, which involves amputation of an entire lower extremity through the hip joint capsule and closure of the remaining musculature over the exposed acetabular bone. If you have had a hemipelvectomy or hip disarticulation, your impairment satisfies the duration requirement in §§ 404.1509 and 416.909 of this chapter.
4. Amputation of one upper extremity and one lower extremity (1.20C). Under 1.20C, we consider the amputation of one upper extremity at any level at or above the wrist and one lower extremity at or above the ankle. If you have a documented medical need for a one-handed, hand-held assistive device (such as a cane) or a wheeled and seated mobility device involving the use of one hand (such as a motorized wheelchair), then you must use your remaining upper extremity to hold the device, making the extremity unavailable to perform other fine and gross movements (see 1.00E4).
5. Amputation of one lower extremity or both lower extremities with complications of the residual limb(s) (1.20D). Under 1.20D, we consider the amputation of one lower extremity or both lower extremities at or above the ankle. We also consider the condition of your residual limb(s), whether you can wear a prosthesis(es) (see 1.00C6b), and whether you have a documented medical need (see 1.00C6a) for a hand-held assistive device(s) (see 1.00C6d) or a wheeled and seated mobility device (see 1.00C6e). If you have a non-healing residual limb(s) and are receiving ongoing surgical treatment expected to re-establish or improve function, and that ongoing surgical treatment has not ended, or is not expected to end, within at least 12 months of the initiation of the surgical management (see 1.00L), we evaluate your musculoskeletal disorder under 1.21.
L. What do we consider when we evaluate soft tissue injuries or abnormalities under continuing surgical management (1.21)?
1. General.
a. We consider any soft tissue injury or abnormality involving the soft tissues of the body, whether congenital or acquired, when an acceptable medical source(s) documents the need for ongoing surgical procedures and associated medical treatments to restore function of the affected body part(s) (see 1.00O1). Surgical management includes the surgery(ies) itself, as well as various post-surgical procedures, surgical complications, infections or other medical complications, related illnesses, or related treatments that delay your attainment of maximum benefit from therapy (see 1.00O2).
b. Surgical procedures and associated treatments typically take place over extended periods, which may render you unable to perform work-related activity on a sustained basis. To document such inability, we must have evidence from an acceptable medical source(s) confirming that the surgical management has continued, or is expected to continue, for at least 12 months from the date of the first surgical intervention. These procedures and treatments must be directed toward saving, reconstructing, or replacing the affected part of the body to re-establish or improve its function, and not for cosmetic appearances alone.
c. Examples include malformations, third- and fourth-degree burns, crush injuries, craniofacial injuries, avulsive injuries, and amputations with complications of the residual limb(s).
d. We evaluate skeletal spine abnormalities or injuries under 1.15 or 1.16, as appropriate. We evaluate abnormalities or injuries of bones in the lower extremities under 1.17, 1.18, or 1.22. We evaluate abnormalities or injuries of bones in the upper extremities under 1.18 or 1.23.
2. Documentation. In addition to the objective medical evidence we need to establish your soft tissue injury or abnormality, we also need all of the following medically documented evidence about your continuing surgical management:
a. Operative reports and related laboratory findings;
b. Records of post-surgical procedures;
c. Records of any surgical or medical complications (for example, related infections or systemic illnesses);
d. Records of any prolonged post-operative recovery periods and related treatments (for example, surgeries and treatments for burns);
e. An acceptable medical source's plans for additional surgeries; and
f. Records detailing any other factors that have delayed, or that an acceptable medical source expects to delay, the saving, restoring, or replacing of the involved part for a continuous period of at least 12 months following the initiation of the surgical management.
3. Burns. Third- and fourth-degree burns damage or destroy nerve tissue, reducing or preventing transmission of signals through those nerves. Such burns frequently require multiple surgical procedures and related therapies to re-establish or improve function, which we evaluate under 1.21. When burns are no longer under continuing surgical management (see 1.00O1), we evaluate the residual impairment(s). When the residual impairment(s) affects the musculoskeletal system, as often occurs in third- and fourth-degree burns, it can result in permanent musculoskeletal tissue loss, joint contractures, or loss of extremities. We will evaluate such impairments under the relevant musculoskeletal disorders listing, for example, 1.18 or 1.20. When the residual impairment(s) involves another body system, we will evaluate the impairment(s) under the listings in the relevant body system(s).
4. Craniofacial injuries. Surgeons may treat craniofacial injuries with multiple surgical procedures. These injuries may affect vision, hearing, speech, and the initiation of the digestive process, including mastication. When the craniofacial injury-related residual impairment(s) involves another body system(s), we will evaluate the impairment(s) under the listings in the relevant body system(s).
M. What do we consider when we evaluate non-healing or complex fractures of the femur, tibia, pelvis, or one or more of the talocrural bones (1.22)?
1. Non-healing fracture. A non-healing (nonunion) fracture is a fracture that has failed to unite completely. Nonunion is usually established when a minimum of 9 months has elapsed since the injury and the fracture site has shown no, or minimal, progressive signs of healing for a minimum of 3 months.
2. Complex fracture. A complex fracture is a fracture with one or more of the following:
a. Comminuted (broken into many pieces) bone fragments;
b. Multiple fractures in a single bone;
c. Bone loss due to severe trauma;
d. Damage to the surrounding soft tissue;
e. Severe cartilage damage to the associated joint; or
f. Dislocation of the associated joint.
3. When a complex fracture involves soft tissue damage, the treatment may involve continuing surgical management to restore or improve functioning. In such cases, we may evaluate the fracture(s) under 1.21.
N. What do we consider when we evaluate non-healing or complex fracture of an upper extremity (1.23)?
1. Non-healing fracture. A non-healing (nonunion) fracture is a fracture that has failed to unite completely. Nonunion is usually established when a minimum of 9 months has elapsed since the injury and the fracture site has shown no, or minimal, progressive signs of healing for a minimum of 3 months.
2. Complex fracture. A complex fracture is a fracture with one or more of the following:
a. Comminuted (broken into many pieces) bone fragments;
b. Multiple fractures in a single bone;
c. Bone loss due to severe trauma;
d. Damage to the surrounding soft tissue;
e. Severe cartilage damage to the associated joint; or
f. Dislocation of the associated joint.
3. When a complex fracture involves soft tissue damage, the treatment may involve continuing surgical management to restore or improve functioning. In such cases, we may evaluate the fracture(s) under 1.21.
O. How will we determine whether your soft tissue injury or abnormality or your upper extremity fracture is no longer under continuing surgical management or you have received maximum benefit from therapy?
1. We will determine that your soft tissue injury or abnormality, or your upper extremity fracture, is no longer under continuing surgical management, as used in 1.21 and 1.23, when the last surgical procedure or medical treatment directed toward the re-establishment or improvement of function of the involved part has occurred.
2. We will determine that you have received maximum benefit from therapy, as used in 1.21, if there are no significant changes in physical findings or on appropriate imaging for any 6-month period after the last surgical procedure or medical treatment. We may also determine that you have received maximum benefit from therapy if your medical source(s) indicates that further improvement is not expected after the last surgical procedure or medical treatment.
3. When you have received maximum benefit from therapy, we will evaluate any impairment-related residual symptoms, signs, and laboratory findings (including those on imaging), any complications associated with your surgical procedures or medical treatments, and any residual limitations in your functioning (see 1.00S).
P. How do we evaluate your musculoskeletal disorder if there is no record of ongoing treatment?
1. Despite having a musculoskeletal disorder, you may not have received ongoing treatment, may have just begun treatment, may not have access to prescribed medical treatment, or may not have an ongoing relationship with the medical community. In any of these situations, you will not have a longitudinal medical record for us to review when we evaluate your disorder and we may ask you to attend a consultative examination to determine the severity and potential duration of your disorder. See §§ 404.1519a(b) and 416.919a(b) of this chapter.
2. In some instances, we may be able to assess the severity and duration of your musculoskeletal disorder based on your medical record and current evidence alone. If the information in your case record is not sufficient to show that you have a musculoskeletal disorder that meets the criteria of one of the musculoskeletal disorders listings, we will follow the rules described in 1.00S.
Q. How do we consider the effects of obesity when we evaluate your musculoskeletal disorder? Obesity is a medically determinable impairment that is often associated with musculoskeletal disorders. Obesity increases stress on weight-bearing joints and may contribute to limitation of the range of motion of the skeletal spine and extremities. The combined effects of obesity with a musculoskeletal disorder can be greater than the effects of each of the impairments considered separately. We consider the additional and cumulative effects of your obesity when we determine whether you have a severe musculoskeletal disorder, a listing-level musculoskeletal disorder, a combination of impairments that medically equals the severity of a listed impairment, and when we assess your residual functional capacity.
R. How do we evaluate your musculoskeletal disorder if there is evidence establishing a substance use disorder? If we find that you are disabled and there is medical evidence in your case record establishing that you have a substance use disorder, we will determine whether your substance use disorder is a contributing factor material to the determination of disability. See §§ 404.1535 and 416.935 of this chapter.
S. How do we evaluate musculoskeletal disorders that do not meet one of these listings?
1. These listings are only examples of musculoskeletal disorders that we consider severe enough to prevent you from doing any gainful activity. If your impairment(s) does not meet the criteria of any of these listings, we must also consider whether you have an impairment(s) that meets the criteria of a listing in another body system.
2. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. See §§ 404.1526 and 416.926 of this chapter. If your impairment(s) does not meet or medically equal a listing, you may or may not have the residual functional capacity to engage in substantial gainful activity. We proceed to the fourth step and, if necessary, the fifth step of the sequential evaluation process in §§ 404.1520 and 416.920 of this chapter.
3. We use the rules in §§ 404.1594 and 416.994 of this chapter, as appropriate, when we decide whether you continue to be disabled.
1.01 Category of Impairments, Musculoskeletal Disorders
1.15 Disorders of the skeletal spine resulting in compromise of a nerve root(s) (see 1.00F), documented by A, B, C, and D:
A. Neuro-anatomic (radicular) distribution of one or more of the following symptoms consistent with compromise of the affected nerve root(s):
1. Pain; or
2. Paresthesia; or
3. Muscle fatigue.
AND
B. Radicular distribution of neurological signs present during physical examination (see 1.00C2) or on a diagnostic test (see 1.00C3) and evidenced by 1, 2, and either 3 or 4:
1. Muscle weakness; and
2. Sign(s) of nerve root irritation, tension, or compression, consistent with compromise of the affected nerve root (see 1.00F2); and
3. Sensory changes evidenced by:
a. Decreased sensation; or
b. Sensory nerve deficit (abnormal sensory nerve latency) on electrodiagnostic testing; or
4. Decreased deep tendon reflexes.
AND
C. Findings on imaging (see 1.00C3) consistent with compromise of a nerve root(s) in the cervical or lumbosacral spine.
AND
D. Impairment-related physical limitation of musculoskeletal functioning that has lasted, or is expected to last, for a continuous period of at least 12 months, and medical documentation of at least one of the following:
1. A documented medical need (see 1.00C6a) for a walker, bilateral canes, or bilateral crutches (see 1.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 1.00C6e(i)); or
2. An inability to use one upper extremity to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 1.00E4), and a documented medical need (see 1.00C6a) for a one-handed, hand-held assistive device (see 1.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 1.00C6e(ii)); or
3. An inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 1.00E4).
1.16 Lumbar spinal stenosis resulting in compromise of the cauda equina (see 1.00G), documented by A, B, C, and D:
A. Symptom(s) of neurological compromise manifested as:
1. Nonradicular distribution of pain in one or both lower extremities; or
2. Nonradicular distribution of sensory loss in one or both lower extremities; or
3. Neurogenic claudication.
AND
B. Nonradicular neurological signs present during physical examination (see 1.00C2) or on a diagnostic test (see 1.00C3) and evidenced by 1 and either 2 or 3:
1. Muscle weakness.
2. Sensory changes evidenced by:
a. Decreased sensation; or
b. Sensory nerve deficit (abnormal sensory nerve latency) on electrodiagnostic testing; or
c. Areflexia, trophic ulceration, or bladder or bowel incontinence.
3. Decreased deep tendon reflexes in one or both lower extremities.
AND
C. Findings on imaging (see 1.00C3) or in an operative report (see 1.00C4) consistent with compromise of the cauda equina with lumbar spinal stenosis.
AND
D. Impairment-related physical limitation of musculoskeletal functioning that has lasted, or is expected to last, for a continuous period of at least 12 months, and medical documentation of at least one of the following:
1. A documented medical need (see 1.00C6a) for a walker, bilateral canes, or bilateral crutches (see 1.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 1.00C6e(i)); or
2. An inability to use one upper extremity to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 1.00E4), and a documented medical need (see 1.00C6a) for a one-handed, hand-held assistive device (see 1.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 1.00C6e(ii)).
1.17 Reconstructive surgery or surgical arthrodesis of a major weight-bearing joint (see 1.00H), documented by A, B, and C:
A. History of reconstructive surgery or surgical arthrodesis of a major weight-bearing joint.
AND
B. Impairment-related physical limitation of musculoskeletal functioning that has lasted, or is expected to last, for a continuous period of at least 12 months.
AND
C. A documented medical need (see 1.00C6a) for a walker, bilateral canes, or bilateral crutches (see 1.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 1.00C6e(i)).
1.18 Abnormality of a major joint(s) in any extremity (see 1.00I), documented by A, B, C, and D:
A. Chronic joint pain or stiffness.
AND
B. Abnormal motion, instability, or immobility of the affected joint(s).
AND
C. Anatomical abnormality of the affected joint(s) noted on:
1. Physical examination (for example, subluxation, contracture, or bony or fibrous ankylosis); or
2. Imaging (for example, joint space narrowing, bony destruction, or ankylosis or arthrodesis of the affected joint).
AND
D. Impairment-related physical limitation of musculoskeletal functioning that has lasted, or is expected to last, for a continuous period of at least 12 months, and medical documentation of at least one of the following:
1. A documented medical need (see 1.00C6a) for a walker, bilateral canes, or bilateral crutches (see 1.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 1.00C6e(i)); or
2. An inability to use one upper extremity to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 1.00E4), and a documented medical need (see 1.00C6a) for a one-handed, hand-held assistive device (see 1.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 1.00C6e(ii)); or
3. An inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 1.00E4).
1.19 Pathologic fractures due to any cause (see 1.00J), documented by A and B:
A. Pathologic fractures occurring on three separate occasions within a 12-month period.
AND
B. Impairment-related physical limitation of musculoskeletal functioning that has lasted, or is expected to last, for a continuous period of at least 12 months, and medical documentation of at least one of the following:
1. A documented medical need (see 1.00C6a) for a walker, bilateral canes, or bilateral crutches (see 1.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 1.00C6e(i)); or
2. An inability to use one upper extremity to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 1.00E4), and a documented medical need (see 1.00C6a) for a one-handed, hand-held assistive device (see 1.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 1.00C6e(ii)); or
3. An inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 1.00E4).
1.20 Amputation due to any cause (see 1.00K), documented by A, B, C, or D:
A. Amputation of both upper extremities, occurring at any level at or above the wrists (carpal joints), up to and including the shoulder (glenohumeral) joint.
OR
B. Hemipelvectomy or hip disarticulation.
OR
C. Amputation of one upper extremity, occurring at any level at or above the wrist (carpal joints), and amputation of one lower extremity, occurring at or above the ankle (talocrural joint), and medical documentation of at least one of the following:
1. A documented medical need (see 1.00C6a) for a walker, bilateral canes, or bilateral crutches (see 1.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 1.00C6e(i)); or
2. A documented medical need (see 1.00C6a) for a one-handed, hand-held assistive device (see 1.00C6d) requiring the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 1.00C6e(ii)); or
3. The inability to use the remaining upper extremity to independently initiate, sustain, and complete work-related activities involving fine and gross movements (1.00E4).
OR
D. Amputation of one or both lower extremities, occurring at or above the ankle (talocrural joint), with complications of the residual limb(s) that have lasted, or are expected to last, for a continuous period of at least 12 months, and medical documentation of 1 and 2:
1. The inability to use a prosthesis(es); and
2. A documented medical need (see 1.00C6a) for a walker, bilateral canes, or bilateral crutches (see 1.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 1.00C6e(i)).
1.21 Soft tissue injury or abnormality under continuing surgical management (see 1.00L), documented by A, B, and C:
A. Evidence confirms continuing surgical management (see 1.00O1) directed toward saving, reconstructing, or replacing the affected part of the body.
AND
B. The surgical management has been, or is expected to be, ongoing for a continuous period of at least 12 months.
AND
C. Maximum benefit from therapy (see 1.00O2) has not yet been achieved.
1.22 Non-healing or complex fracture of the femur, tibia, pelvis, or one or more of the talocrural bones (see 1.00M), documented by A, B, and C:
A. Solid union not evident on imaging (see 1.00C3) and not clinically solid.
AND
B. Impairment-related physical limitation of musculoskeletal functioning that has lasted, or is expected to last, for a continuous period of at least 12 months.
AND
C. A documented medical need (see 1.00C6a) for a walker, bilateral canes, or bilateral crutches (see 1.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 1.00C6e(i)).
1.23 Non-healing or complex fracture of an upper extremity (see 1.00N), documented by A and B:
A. Nonunion or complex fracture of the shaft of the humerus, radius, or ulna, under continuing surgical management (see 1.00O1) directed toward restoration of functional use of the extremity.
AND
B. Medical documentation of an inability to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 1.00E4) that has lasted, or is expected to last, for a continuous period of at least 12 months.
2.00 Special Senses and Speech
A. How do we evaluate visual disorders?
1. What are visual disorders? Visual disorders are abnormalities of the eye, the optic nerve, the optic tracts, or the brain that may cause a loss of visual acuity or visual fields. A loss of visual acuity limits your ability to distinguish detail, read, or do fine work. A loss of visual fields limits your ability to perceive visual stimuli in the peripheral extent of vision.
2. How do we define statutory blindness? Statutory blindness is blindness as defined in sections 216(i)(1) and 1614(a)(2) of the Social Security Act (Act).
a. The Act defines blindness as central visual acuity of 20/200 or less in the better eye with the use of a correcting lens. We use your best-corrected central visual acuity for distance in the better eye when we determine if this definition is met. (For visual acuity testing requirements, see 2.00A5.)
b. The Act also provides that an eye that has a visual field limitation such that the widest diameter of the visual field subtends an angle no greater than 20 degrees is considered as having a central visual acuity of 20/200 or less. (For visual field testing requirements, see 2.00A6.)
c. You have statutory blindness only if your visual disorder meets the criteria of 2.02 or 2.03A. You do not have statutory blindness if your visual disorder medically equals the criteria of 2.02 or 2.03A or meets or medically equals the criteria of 2.03B, 2.03C, 2.04A, or 2.04B because your disability is based on criteria other than those in the statutory definition of blindness.
3. What evidence do we need to establish statutory blindness under title XVI? To establish that you have statutory blindness under title XVI, we need evidence showing only that your central visual acuity in your better eye or your visual field in your better eye meets the criteria in 2.00A2, provided that those measurements are consistent with the other evidence in your case record. We do not need documentation of the cause of your blindness. Also, there is no duration requirement for statutory blindness under title XVI (see §§ 416.981 and 416.983 of this chapter).
4. What evidence do we need to evaluate visual disorders, including those that result in statutory blindness under title II? To evaluate your visual disorder, we usually need a report of an eye examination that includes measurements of your best-corrected central visual acuity (see 2.00A5) or the extent of your visual fields (see 2.00A6), as appropriate. If you have visual acuity or visual field loss, we need documentation of the cause of the loss. A standard eye examination will usually indicate the cause of any visual acuity loss. A standard eye examination can also indicate the cause of some types of visual field deficits. Some disorders, such as cortical visual disorders, may result in abnormalities that do not appear on a standard eye examination. If the standard eye examination does not indicate the cause of your vision loss, we will request the information used to establish the presence of your visual disorder. If your visual disorder does not satisfy the criteria in 2.02, 2.03, or 2.04, we will request a description of how your visual disorder affects your ability to function.
5. How do we measure your best-corrected central visual acuity?
a. Visual acuity testing. When we need to measure your best-corrected central visual acuity (your optimal visual acuity attainable with the use of a corrective lens), we use visual acuity testing for distance that was carried out using Snellen methodology or any other testing methodology that is comparable to Snellen methodology.
(i) Your best-corrected central visual acuity for distance is usually measured by determining what you can see from 20 feet. If your visual acuity is measured for a distance other than 20 feet, we will convert it to a 20-foot measurement. For example, if your visual acuity is measured at 10 feet and is reported as 10/40, we will convert this measurement to 20/80.
(ii) A visual acuity recorded as CF (counts fingers), HM (hand motion only), LP or LPO (light perception or light perception only), or NLP (no light perception) indicates that no optical correction will improve your visual acuity. If your central visual acuity in an eye is recorded as CF, HM, LP or LPO, or NLP, we will determine that your best-corrected central visual acuity is 20/200 or less in that eye.
(iii) We will not use the results of pinhole testing or automated refraction acuity to determine your best-corrected central visual acuity. These tests provide an estimate of potential visual acuity but not an actual measurement of your best-corrected central visual acuity.
b. Other test charts. Most test charts that use Snellen methodology do not have lines that measure visual acuity between 20/100 and 20/200. Some test charts, such as the Bailey-Lovie or the Early Treatment Diabetic Retinopathy Study (ETDRS), used mostly in research settings, have such lines. If your visual acuity is measured with one of these charts, and you cannot read any of the letters on the 20/100 line, we will determine that you have statutory blindness based on a visual acuity of 20/200 or less. For example, if your best-corrected central visual acuity for distance in the better eye is 20/160 using an ETDRS chart, we will find that you have statutory blindness. Regardless of the type of test chart used, you do not have statutory blindness if you can read at least one letter on the 20/100 line. For example, if your best-corrected central visual acuity for distance in the better eye is 20/125 + 1 using an ETDRS chart, we will find that you do not have statutory blindness because you are able to read one letter on the 20/100 line.
c. Testing using a specialized lens. In some instances, you may have visual acuity testing performed using specialized lens, such as a contact lens. We will use the visual acuity measurements obtained with a specialized lens only if you have demonstrated the ability to use the specialized lens on a sustained basis. We will not use visual acuity measurements obtained with telescopic lenses.
d. Cycloplegic refraction is an examination of the eye performed after administering cycloplegic eye drops capable of relaxing the ability of the pupil to become smaller and temporarily paralyzing the focusing muscles. If your case record contains the results of cycloplegic refraction, we may use the results to determine your best-corrected central visual acuity. We will not purchase cycloplegic refraction.
e. Visual evoked response (VER) testing measures your response to visual events and can often detect dysfunction that is undetectable through other types of examinations. If you have an absent response to VER testing in your better eye, we will determine that your best-corrected central visual acuity is 20/200 or less in that eye and that your visual acuity loss satisfies the criterion in 2.02 when these test results are consistent with the other evidence in your case record. If you have a positive response to VER testing in an eye, we will not use that result to determine your best-corrected central visual acuity in that eye.
6. How do we measure your visual fields?
a. General. We generally need visual field testing when you have a visual disorder that could result in visual field loss, such as glaucoma, retinitis pigmentosa, or optic neuropathy, or when you display behaviors that suggest a visual field loss. When we need to measure the extent of your visual field loss, we use visual field testing (also referred to as perimetry) carried out using automated static threshold perimetry performed on an acceptable perimeter. (For perimeter requirements, see 2.00A9.)
b. Automated static threshold perimetry requirements.
(i) The test must use a white size III Goldmann stimulus and a 31.5 apostilb (asb) white background (or a 10 candela per square meter (cd/m2) white background). The stimuli test locations must be no more than 6 degrees apart horizontally or vertically. Measurements must be reported on standard charts and include a description of the size and intensity of the test stimulus.
(ii) We measure the extent of your visual field loss by determining the portion of the visual field in which you can see a white III4e stimulus. The “III” refers to the standard Goldmann test stimulus size III (4 mm2), and the “4e” refers to the standard Goldmann intensity filter (0 decibel (dB) attenuation, which allows presentation of the maximum luminance) used to determine the intensity of the stimulus.
(iii) In automated static threshold perimetry, the intensity of the stimulus varies. The intensity of the stimulus is expressed in decibels (dB). A perimeter's maximum stimulus luminance is usually assigned the value 0 dB. We need to determine the dB level that corresponds to a 4e intensity for the particular perimeter being used. We will then use the dB printout to determine which points you see at a 4e intensity level (a “seeing point”). For example:
A. When the maximum stimulus luminance (0 dB stimulus) on an acceptable perimeter is 10,000 asb, a 10 dB stimulus is equivalent to a 4e stimulus. Any point you see at 10 dB or greater is a seeing point.
B. When the maximum stimulus luminance (0 dB stimulus) on an acceptable perimeter is 4,000 asb, a 6 dB stimulus is equivalent to a 4e stimulus. Any point you see at 6 dB or greater is a seeing point.
C. When the maximum stimulus luminance (0 dB stimulus) on an acceptable perimeter is 1,000 asb, a 0 dB stimulus is equivalent to a 4e stimulus. Any point you see at 0 dB or greater is a seeing point.
c. Evaluation under 2.03A. To determine statutory blindness based on visual field loss in your better eye (2.03A), we need the results of a visual field test that measures the central 24 to 30 degrees of your visual field; that is, the area measuring 24 to 30 degrees from the point of fixation. Acceptable tests include the Humphrey Field Analyzer (HFA) 30-2, HFA 24-2, and Octopus 32.
d. Evaluation under 2.03B. To determine whether your visual field loss meets listing 2.03B, we use the mean deviation or defect (MD) from acceptable automated static threshold perimetry that measures the central 30 degrees of the visual field. MD is the average sensitivity deviation from normal values for all measured visual field locations. When using results from HFA tests, which report the MD as a negative number, we use the absolute value of the MD to determine whether your visual field loss meets listing 2.03B. We cannot use tests that do not measure the central 30 degrees of the visual field, such as the HFA 24-2, to determine if your impairment meets or medically equals 2.03B.
e. Other types of perimetry. If the evidence in your case contains visual field measurements obtained using manual or automated kinetic perimetry, such as Goldmann perimetry or the HFA “SSA Test Kinetic,” we can generally use these results if the kinetic test was performed using a white III4e stimulus projected on a white 31.5 asb (10 cd/m2) background. Automated kinetic perimetry, such as the HFA “SSA Test Kinetic,” does not detect limitations in the central visual field because testing along a meridian stops when you see the stimulus. If your visual disorder has progressed to the point at which it is likely to result in a significant limitation in the central visual field, such as a scotoma (see 2.00A6h), we will not use automated kinetic perimetry to determine the extent of your visual field loss. Instead, we will determine the extent of your visual field loss using automated static threshold perimetry or manual kinetic perimetry.
f. Screening tests. We will not use the results of visual field screening tests, such as confrontation tests, tangent screen tests, or automated static screening tests, to determine that your impairment meets or medically equals a listing or to evaluate your residual functional capacity. We can consider normal results from visual field screening tests to determine whether your visual disorder is severe when these test results are consistent with the other evidence in your case record. (See §§ 404.1520(c), 404.1521, 416.920(c), and 416.921 of this chapter.) We will not consider normal test results to be consistent with the other evidence if the clinical findings indicate that your visual disorder has progressed to the point that it is likely to cause visual field loss, or you have a history of an operative procedure for retinal detachment.
g. Use of corrective lenses. You must not wear eyeglasses during visual field testing because they limit your field of vision. You may wear contact lenses to correct your visual acuity during the visual field test to obtain the most accurate visual field measurements. For this single purpose, you do not need to demonstrate that you have the ability to use the contact lenses on a sustained basis.
h. Scotoma. A scotoma is a field defect or non-seeing area (also referred to as a “blind spot”) in the visual field surrounded by a normal field or seeing area. When we measure your visual field, we subtract the length of any scotoma, other than the normal blind spot, from the overall length of any diameter on which it falls.
7. How do we determine your visual acuity efficiency, visual field efficiency, and visual efficiency?
a. General. Visual efficiency, a calculated value of your remaining visual function, is the combination of your visual acuity efficiency and your visual field efficiency expressed as a percentage.
b. Visual acuity efficiency. Visual acuity efficiency is a percentage that corresponds to the best-corrected central visual acuity for distance in your better eye. See Table 1.
Table 1 - Visual Acuity Efficiency
| Snellen best-corrected central visual acuity for distance | Visual acuity efficiency (%)
(2.04A) | |
|---|---|---|
| English | Metric | |
| 20/16 | 6/5 | 100 |
| 20/20 | 6/6 | 100 |
| 20/25 | 6/7.5 | 95 |
| 20/30 | 6/9 | 90 |
| 20/40 | 6/12 | 85 |
| 20/50 | 6/15 | 75 |
| 20/60 | 6/18 | 70 |
| 20/70 | 6/21 | 65 |
| 20/80 | 6/24 | 60 |
| 20/100 | 6/30 | 50 |
c. Visual field efficiency. Visual field efficiency is a percentage that corresponds to the visual field in your better eye. Under 2.03C, we require kinetic perimetry to determine your visual field efficiency percentage. We calculate the visual field efficiency percentage by adding the number of degrees you see along the eight principal meridians found on a visual field chart (0, 45, 90, 135, 180, 225, 270, and 315) in your better eye and dividing by 5. For example, in Figure 1:
A. The diagram of the left eye illustrates a visual field, as measured with a III4e stimulus, contracted to 30 degrees in two meridians (180 and 225) and to 20 degrees in the remaining six meridians. The visual efficiency percentage of this field is: ((2 × 30) + (6 × 20)) ÷ 5 = 36 percent.
B. The diagram of the right eye illustrates the extent of a normal visual field as measured with a III4e stimulus. The sum of the eight principal meridians of this field is 500 degrees. The visual efficiency percentage of this field is 500 ÷ 5 = 100 percent.
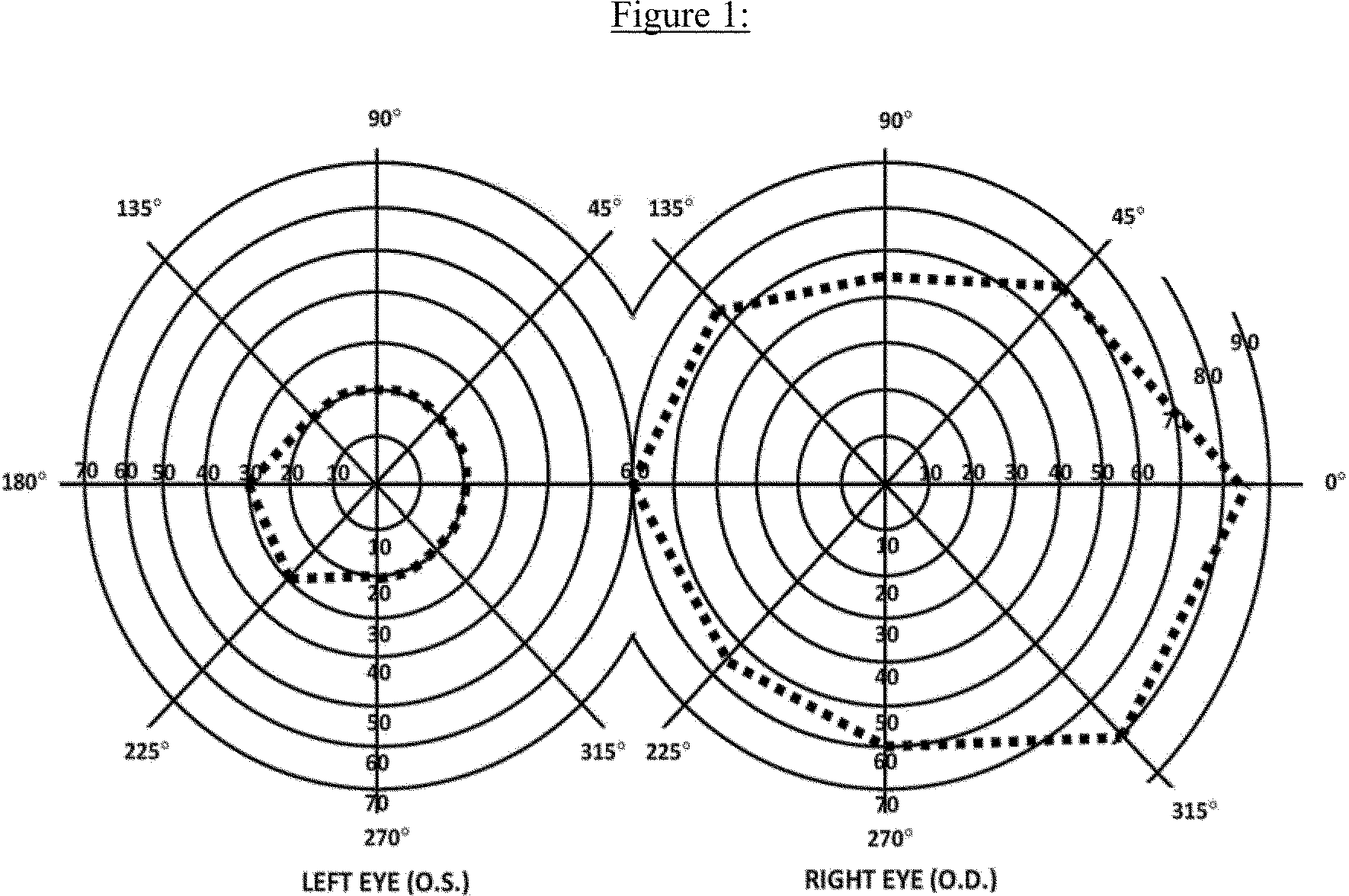
d. Visual efficiency. Under 2.04A, we calculate the visual efficiency percentage by multiplying your visual acuity efficiency percentage (see 2.00A7b) by your visual field efficiency percentage (see 2.00A7c) and dividing by 100. For example, if your visual acuity efficiency percentage is 75 and your visual field efficiency percentage is 36, your visual efficiency percentage is: (75 × 36) ÷ 100 = 27 percent.
8. How do we determine your visual acuity impairment value, visual field impairment value, and visual impairment value?
a. General. Visual impairment value, a calculated value of your loss of visual function, is the combination of your visual acuity impairment value and your visual field impairment value.
b. Visual acuity impairment value. Your visual acuity impairment value corresponds to the best-corrected central visual acuity for distance in your better eye. See Table 2.
Table 2 - Visual Acuity Impairment Value
| Snellen best-corrected central visual acuity for distance | Visual acuity
impairment value (2.04B) | |
| English | Metric | |
| 20/16 | 6/5 | 0.00 |
| 20/20 | 6/6 | 0.00 |
| 20/25 | 6/7.5 | 0.10 |
| 20/30 | 6/9 | 0.18 |
| 20/40 | 6/12 | 0.30 |
| 20/50 | 6/15 | 0.40 |
| 20/60 | 6/18 | 0.48 |
| 20/70 | 6/21 | 0.54 |
| 20/80 | 6/24 | 0.60 |
| 20/100 | 6/30 | 0.70 |
c. Visual field impairment value. Your visual field impairment value corresponds to the visual field in your better eye. Using the MD from acceptable automated static threshold perimetry, we calculate the visual field impairment value by dividing the absolute value of the MD by 22. For example, if your MD on an HFA 30-2 is −16, your visual field impairment value is: −16| ÷ 22 = 0.73.
d. Visual impairment value. Under 2.04B, we calculate the visual impairment value by adding your visual acuity impairment value (see 2.00A8b) and your visual field impairment value (see 2.00A8c). For example, if your visual acuity impairment value is 0.48 and your visual field impairment value is 0.73, your visual impairment value is: 0.48 + 0.73 = 1.21.
9. What are our requirements for an acceptable perimeter? We will use results from automated static threshold perimetry performed on a perimeter that:
a. Uses optical projection to generate the test stimuli.
b. Has an internal normative database for automatically comparing your performance with that of the general population.
c. Has a statistical analysis package that is able to calculate visual field indices, particularly MD.
d. Demonstrates the ability to correctly detect visual field loss and correctly identify normal visual fields.
e. Demonstrates good test-retest reliability.
f. Has undergone clinical validation studies by three or more independent laboratories with results published in peer-reviewed ophthalmic journals.
B. How do we evaluate hearing loss?
1. What evidence do we need?
a. We need evidence showing that you have a medically determinable impairment that causes your hearing loss and audiometric measurements of the severity of your hearing loss. We generally require both an otologic examination and audiometric testing to establish that you have a medically determinable impairment that causes your hearing loss. You should have this audiometric testing within 2 months of the otologic examination. Once we have evidence that you have a medically determinable impairment, we can use the results of later audiometric testing to assess the severity of your hearing loss without another otologic examination. We will consider your test scores together with any other relevant information we have about your hearing, including information from outside of the test setting.
b. The otologic examination must be performed by a licensed physician (medical or osteopathic doctor) or audiologist. It must include your medical history, your description of how your hearing loss affects you, and the physician's or audiologist's description of the appearance of the external ears (pinnae and external ear canals), evaluation of the tympanic membranes, and assessment of any middle ear abnormalities.
c. Audiometric testing must be performed by, or under the direct supervision of, a licensed audiologist or an otolaryngologist.
2. What audiometric testing do we need when you do not have a cochlear implant?
a. We generally need pure tone air conduction and bone conduction testing, speech reception threshold (SRT) testing (also referred to as “spondee threshold” or “ST” testing), and word recognition testing (also referred to as “word discrimination” or “speech discrimination” testing). This testing must be conducted in a sound-treated booth or room and must be in accordance with the most recently published standards of the American National Standards Institute (ANSI). Each ear must be tested separately.
b. You must not wear hearing aids during the testing. Additionally, a person described in 2.00B1c must perform an otoscopic examination immediately before the audiometric testing. (An otoscopic examination provides a description of the appearance of your external ear canals and an evaluation of the tympanic membranes. In these rules, we use the term to include otoscopic examinations performed by physicians and otoscopic inspections performed by audiologists and others.) The otoscopic examination must show that there are no conditions that would prevent valid audiometric testing, such as fluid in the ear, ear infection, or obstruction in an ear canal. The person performing the test should also report on any other factors, such as your cooperation with the test, that can affect the interpretation of the test results.
c. To determine whether your hearing loss meets the air and bone conduction criteria in 2.10A, we will average your air and bone conduction hearing thresholds at 500, 1000, and 2000 Hertz (Hz). If you do not have a response at a particular frequency, we will use a threshold of 5 decibels (dB) over the limit of the audiometer.
d. The SRT is the minimum dB level required for you to recognize 50 percent of the words on a standard list of spondee words. (Spondee words are two-syllable words that have equal stress on each syllable.) The SRT is usually within 10 dB of the average pure tone air conduction hearing thresholds at 500, 1000, and 2000 Hz. If the SRT is not within 10 dB of the average pure tone air conduction threshold, the reason for the discrepancy must be documented. If we cannot determine that there is a medical basis for the discrepancy, we will not use the results of the testing to determine whether your hearing loss meets a listing.
e. Word recognition testing determines your ability to recognize a standardized list of phonetically balanced monosyllabic words in the absence of any visual cues. This testing must be performed in quiet. The list may be recorded or presented live, but in either case the words should be presented at a level of amplification that will measure your maximum ability to discriminate words, usually 35 to 40 dB above your SRT. However, the amplification level used in the testing must be medically appropriate, and you must be able to tolerate it. If you cannot be tested at 35 to 40 dB above your SRT, the person who performs the test should report your word recognition testing score at your highest comfortable level of amplification.
3. What audiometric testing do we need when you have a cochlear implant?
a. If you have a cochlear implant, we will consider you to be disabled until 1 year after initial implantation.
b. After that period, we need word recognition testing performed with any version of the Hearing in Noise Test (HINT) to determine whether your impairment meets 2.11B. This testing must be conducted in quiet in a sound field. Your implant must be functioning properly and adjusted to your normal settings. The sentences should be presented at 60 dB HL (Hearing Level) and without any visual cues.
4. How do we evaluate your word recognition ability if you are not fluent in English?
If you are not fluent in English, you should have word recognition testing using an appropriate word list for the language in which you are most fluent. The person conducting the test should be fluent in the language used for the test. If there is no appropriate word list or no person who is fluent in the language and qualified to perform the test, it may not be possible to measure your word recognition ability. If your word recognition ability cannot be measured, your hearing loss cannot meet 2.10B or 2.11B. Instead, we will consider the facts of your case to determine whether you have difficulty understanding words in the language in which you are most fluent, and if so, whether that degree of difficulty medically equals 2.10B or 2.11B. For example, we will consider how you interact with family members, interpreters, and other persons who speak the language in which you are most fluent.
C. How do we evaluate vertigo associated with disturbances of labyrinthine-vestibular function, including Meniere's disease?
1. These disturbances of balance are characterized by an hallucination of motion or loss of position sense and a sensation of dizziness which may be constant or may occur in paroxysmal attacks. Nausea, vomiting, ataxia, and incapacitation are frequently observed, particularly during the acute attack. It is important to differentiate the report of rotary vertigo from that of “dizziness” which is described as lightheadedness, unsteadiness, confusion, or syncope.
2. Meniere's disease is characterized by paroxysmal attacks of vertigo, tinnitus, and fluctuating hearing loss. Remissions are unpredictable and irregular, but may be longlasting; hence, the severity of impairment is best determined after prolonged observation and serial reexaminations.
3. The diagnosis of a vestibular disorder requires a comprehensive neuro-otolaryngologic examination with a detailed description of the vertiginous episodes, including notation of frequency, severity, and duration of the attacks. Pure tone and speech audiometry with the appropriate special examinations, such as Bekesy audiometry, are necessary. Vestibular functions is assessed by positional and caloric testing, preferably by electronystagmography. When polytomograms, contrast radiography, or other special tests have been performed, copies of the reports of these tests should be obtained in addition to appropriate medically acceptable imaging reports of the skull and temporal bone. Medically acceptable imaging includes, but is not limited to, x-ray imaging, computerized axial tomography (CAT scan) or magnetic resonance imaging (MRI), with or without contrast material, myelography, and radionuclear bone scans. “Appropriate” means that the technique used is the proper one to support the evaluation and diagnosis of the impairment.
D. Loss of speech. In evaluating the loss of speech, the ability to produce speech by any means includes the use of mechanical or electronic devices that improve voice or articulation. Impairments of speech may also be evaluated under the body system for the underlying disorder, such as neurological disorders, 11.00ff.
E. How do we evaluate impairments that do not meet one of the special senses and speech listings?
1. These listings are only examples of common special senses and speech disorders that we consider severe enough to prevent an individual from doing any gainful activity. If your impairment(s) does not meet the criteria of any of these listings, we must also consider whether you have an impairment(s) that satisfies the criteria of a listing in another body system.
2. If you have a medically determinable impairment(s) that does not meet a listing, we will determine whether the impairment(s) medically equals a listing. (See §§ 404.1526 and 416.926.) If you have an impairment(s) that does not meet or medically equal a listing, you may or may not have the residual functional capacity to engage in substantial gainful activity. Therefore, we proceed to the fourth, and if necessary, the fifth steps of the sequential evaluation process in §§ 404.1520 and 416.920. When we decide whether you continue to be disabled, we use the rules in §§ 404.1594, 416.994, or 416.994a, as appropriate.
2.01 Category of Impairments, Special Senses and Speech
2.02 Loss of central visual acuity. Remaining vision in the better eye after best correction is 20/200 or less.
2.03 Contraction of the visual field in the better eye, with:
A. The widest diameter subtending an angle around the point of fixation no greater than 20 degrees.
OR
B. An MD of 22 decibels or greater, determined by automated static threshold perimetry that measures the central 30 degrees of the visual field (see 2.00A6d).
OR
C. A visual field efficiency of 20 percent or less, determined by kinetic perimetry (see 2.00A7c).
2.04 Loss of visual efficiency, or visual impairment, in the better eye:
A. A visual efficiency percentage of 20 or less after best correction (see 2.00A7d).
OR
B. A visual impairment value of 1.00 or greater after best correction (see 2.00A8d).
2.07 Disturbance of labyrinthine-vestibular function (including Meniere's disease), characterized by a history of frequent attacks of balance disturbance, tinnitus, and progressive loss of hearing. With both A and B:
A. Disturbed function of vestibular labyrinth demonstrated by caloric or other vestibular tests; and
B. Hearing loss established by audiometry.
2.09 Loss of speech due to any cause, with inability to produce by any means speech that can be heard, understood, or sustained.
Table 1 - Percentage of Visual Acuity Efficiency Corresponding to the Best-Corrected Visual Acuity Measurement for Distance in the Better Eye
| Snellen | Percent
visual acuity efficiency | |
|---|---|---|
| English | Metric | |
| 20/16 | 6/5 | 100 |
| 20/20 | 6/6 | 100 |
| 20/25 | 6/7.5 | 95 |
| 20/30 | 6/9 | 90 |
| 20/40 | 6/12 | 85 |
| 20/50 | 6/15 | 75 |
| 20/60 | 6/18 | 70 |
| 20/70 | 6/21 | 65 |
| 20/80 | 6/24 | 60 |
| 20/100 | 6/30 | 50 |
Table 2 - Chart of Visual Fields

1. The diagram of the right eye illustrates the extent of a normal visual field as measured with a III4e stimulus. The sum of the eight principal meridians of this field is 500 degrees.
2. The diagram of the left eye illustrates a visual field contracted to 30 degrees in two meridians and to 20 degrees in the remaining six meridians. The percent of visual field efficiency of this field is: (2 × 30) + (6 × 20) = 180 ÷ 500 = 0.36 or 36 percent visual field efficiency.
2.10 Hearing loss not treated with cochlear implantation.
A. An average air conduction hearing threshold of 90 decibels or greater in the better ear and an average bone conduction hearing threshold of 60 decibels or greater in the better ear (see 2.00B2c).
OR
B. A word recognition score of 40 percent or less in the better ear determined using a standardized list of phonetically balanced monosyllabic words (see 2.00B2e).
2.11 Hearing loss treated with cochlear implantation.
A. Consider under a disability for 1 year after initial implantation.
OR
B. If more than 1 year after initial implantation, a word recognition score of 60 percent or less determined using the HINT (see 2.00B3b).
3.00 Respiratory Disorders
A. Which disorders do we evaluate in this body system?
1. We evaluate respiratory disorders that result in obstruction (difficulty moving air out of the lungs) or restriction (difficulty moving air into the lungs), or that interfere with diffusion (gas exchange) across cell membranes in the lungs. Examples of such disorders and the listings we use to evaluate them include chronic obstructive pulmonary disease (chronic bronchitis and emphysema, 3.02), pulmonary fibrosis and pneumoconiosis (3.02), asthma (3.02 or 3.03), cystic fibrosis (3.04), and bronchiectasis (3.02 or 3.07). We also use listings in this body system to evaluate respiratory failure (3.04D or 3.14), chronic pulmonary hypertension (3.09), and lung transplantation (3.11).
2. We evaluate cancers affecting the respiratory system under the listings in 13.00. We evaluate the pulmonary effects of neuromuscular and autoimmune disorders under these listings or under the listings in 11.00 or 14.00, respectively.
B. What are the symptoms and signs of respiratory disorders? Symptoms and signs of respiratory disorders include dyspnea (shortness of breath), chest pain, coughing, wheezing, sputum production, hemoptysis (coughing up blood from the respiratory tract), use of accessory muscles of respiration, and tachypnea (rapid rate of breathing).
C. What abbreviations do we use in this body system?
1. ABG means arterial blood gas.
2. BiPAP means bi-level positive airway pressure ventilation.
3. BTPS means body temperature and ambient pressure, saturated with water vapor.
4. CF means cystic fibrosis.
5. CFRD means CF-related diabetes.
6. CFTR means CF transmembrane conductance regulator.
7. CO means carbon monoxide.
8. COPD means chronic obstructive pulmonary disease.
9. DLCO means diffusing capacity of the lungs for carbon monoxide.
10. FEV1 means forced expiratory volume in the first second of a forced expiratory maneuver.
11. FVC means forced vital capacity.
12. L means liter.
13. mL CO (STPD)/min/mmHg means milliliters of carbon monoxide at standard temperature and pressure, dry, per minute, per millimeter of mercury.
14. PaO2 means arterial blood partial pressure of oxygen.
15. PaCO2 means arterial blood partial pressure of carbon dioxide.
16. SpO2 means percentage of oxygen saturation of blood hemoglobin measured by pulse oximetry.
17. 6MWT means 6-minute walk test.
18. VI means volume of inhaled gas during a DLCO test.
D. What documentation do we need to evaluate your respiratory disorder?
1. We need medical evidence to document and assess the severity of your respiratory disorder. Medical evidence should include your medical history, physical examination findings, the results of imaging (see 3.00D3), pulmonary function tests (see 3.00D4), other relevant laboratory tests, and descriptions of any prescribed treatment and your response to it. We may not need all of this evidence depending on your particular respiratory disorder and its effects on you.
2. If you use supplemental oxygen, we still need medical evidence to establish the severity of your respiratory disorder.
3. Imaging refers to medical imaging techniques, such as x-ray and computerized tomography. The imaging must be consistent with the prevailing state of medical knowledge and clinical practice as the proper technique to support the evaluation of the disorder.
4. Pulmonary function tests include spirometry (which measures ventilation of the lungs), DLCO tests (which measure gas diffusion in the lungs), ABG tests (which measure the partial pressure of oxygen, PaO2, and carbon dioxide, PaCO2, in the arterial blood), and pulse oximetry (which measures oxygen saturation, SpO2, of peripheral blood hemoglobin).
E. What is spirometry and what are our requirements for an acceptable test and report?
1. Spirometry, which measures how well you move air into and out of your lungs, involves at least three forced expiratory maneuvers during the same test session. A forced expiratory maneuver is a maximum inhalation followed by a forced maximum exhalation, and measures exhaled volumes of air over time. The volume of air you exhale in the first second of the forced expiratory maneuver is the FEV1. The total volume of air that you exhale during the entire forced expiratory maneuver is the FVC. We use your highest FEV1 value to evaluate your respiratory disorder under 3.02A, 3.03A, and 3.04A, and your highest FVC value to evaluate your respiratory disorder under 3.02B, regardless of whether the values are from the same forced expiratory maneuver or different forced expiratory maneuvers.
2. We have the following requirements for spirometry under these listings:
a. You must be medically stable at the time of the test. Examples of when we would not consider you to be medically stable include when you are:
(i) Within 2 weeks of a change in your prescribed respiratory medication.
(ii) Experiencing, or within 30 days of completion of treatment for, a lower respiratory tract infection.
(iii) Experiencing, or within 30 days of completion of treatment for, an acute exacerbation (temporary worsening) of a chronic respiratory disorder. Wheezing by itself does not indicate that you are not medically stable.
(iv) Hospitalized, or within 30 days of a hospital discharge, for an acute myocardial infarction (heart attack).
b. During testing, if your FEV1 is less than 70 percent of your predicted normal value, we require repeat spirometry after inhalation of a bronchodilator to evaluate your respiratory disorder under these listings, unless it is medically contraindicated. If you used a bronchodilator before the test and your FEV1 is less than 70 percent of your predicted normal value, we still require repeat spirometry after inhalation of a bronchodilator unless the supervising physician determines that it is not safe for you to take a bronchodilator again (in which case we may need to reschedule the test). If you do not have post-bronchodilator spirometry, the test report must explain why. We can use the results of spirometry administered without bronchodilators when the use of bronchodilators is medically contraindicated.
c. Your forced expiratory maneuvers must be satisfactory. We consider a forced expiratory maneuver to be satisfactory when you exhale with maximum effort following a full inspiration, and when the test tracing has a sharp takeoff and rapid rise to peak flow, has a smooth contour, and either lasts for at least 6 seconds or maintains a plateau for at least 1 second.
3. The spirometry report must include the following information:
a. The date of the test and your name, age or date of birth, gender, and height without shoes. (We will assume that your recorded height on the date of the test is without shoes, unless we have evidence to the contrary.) If your spine is abnormally curved (for example, you have kyphoscoliosis), we will substitute the longest distance between your outstretched fingertips with your arms abducted 90 degrees in place of your height when this measurement is greater than your standing height without shoes.
b. Any factors, if applicable, that can affect the interpretation of the test results (for example, your cooperation or effort in doing the test).
c. Legible tracings of your forced expiratory maneuvers in a volume-time format showing your name and the date of the test for each maneuver.
4. If we purchase spirometry, the medical source we designate to administer the test is solely responsible for deciding whether it is safe for you to do the test and for how to administer it.
F. What is a DLCO test, and what are our requirements for an acceptable test and report?
1. A DLCO test measures the gas exchange across cell membranes in your lungs. It measures how well CO diffuses from the alveoli (air sacs) of your lungs into your blood. DLCO may be severely reduced in some disorders, such as interstitial lung disease (for example, idiopathic pulmonary fibrosis, asbestosis, and sarcoidosis) and COPD (particularly emphysema), even when the results of spirometry are not significantly reduced. We use the average of two of your unadjusted (that is, uncorrected for hemoglobin concentration) DLCO measurements reported in mL CO (STPD)/min/mmHg to evaluate your respiratory disorder under 3.02C1.
2. We have the following requirements for DLCO tests under these listings:
a. You must be medically stable at the time of the test. See 3.00E2a.
b. The test must use the single-breath technique.
(i) The VI during the DLCO maneuver must be at least 85 percent of your current FVC, and your time of inhalation must be less than 4 seconds. (See 3.00E for our rules for programmatically acceptable spirometry.) If you do not have an FVC measurement on the same day as the DLCO test, we may use your FVC from programmatically acceptable spirometry administered within 90 days of the DLCO test.
(ii) Your breath-hold time must be between 8 and 12 seconds.
(iii) Your total exhalation time must be less than or equal to 4 seconds, with a sample collection time of less than 3 seconds. If your FVC is at least 2.0 L, the washout volume must be between 0.75 L and 1.0 L. If your FVC is less than 2.0 L, the washout volume must be at least 0.5 L.
3. The DLCO test report must include the following information:
a. The date of the test and your name, age or date of birth, gender, and height without shoes. (We will assume that your recorded height on the date of the test is without shoes, unless we have evidence to the contrary.) If your spine is abnormally curved (for example, you have kyphoscoliosis), we will substitute the longest distance between your outstretched fingertips with your arms abducted 90 degrees in place of your height when this measurement is greater than your standing height without shoes.
b. Any factors, if applicable, that can affect the interpretation of the test results (for example, your cooperation or effort in doing the test).
c. Legible tracings of your VI, breath-hold maneuver, and volume of exhaled gas showing your name and the date of the test for each DLCO maneuver.
d. At least two acceptable (see 3.00F2) DLCO measurements within 3 mL CO (STPD)/min/mmHg of each other or within 10 percent of the highest value.
4. We may need to purchase a DLCO test to determine whether your disorder meets 3.02C1 when we have evidence showing that you have a chronic respiratory disorder that could result in impaired gas exchange, unless we can make a fully favorable determination or decision on another basis. Since the DLCO calculation requires a current FVC measurement, we may also purchase spirometry at the same time as the DLCO test, even if we already have programmatically acceptable spirometry.
5. Before we purchase a DLCO test, a medical consultant (see §§ 404.1616 and 416.1016 of this chapter), preferably one with experience in the care of people with respiratory disorders, must review your case record to determine if we need the test. The medical source we designate to administer the test is solely responsible for deciding whether it is safe for you to do the test and for how to administer it.
G. What is an ABG test, and what are our requirements for an acceptable test and report?
1. General. An ABG test measures PaO2, PaCO2, and the concentration of hydrogen ions in your arterial blood. We use a resting or an exercise ABG measurement to evaluate your respiratory disorder under 3.02C2.
2. Resting ABG tests.
a. We have the following requirements for resting ABG tests under these listings:
(i) You must be medically stable at the time of the test. See 3.00E2a.
(ii) The test must be administered while you are breathing room air; that is, without oxygen supplementation.
b. The resting ABG test report must include the following information:
(i) Your name, the date of the test, and either the altitude or both the city and State of the test site.
(ii) The PaO2 and PaCO2 values.
c. We may need to purchase a resting ABG test to determine whether your disorder meets 3.02C2 when we have evidence showing that you have a chronic respiratory disorder that could result in impaired gas exchange, unless we can make a fully favorable determination or decision on another basis.
d. Before we purchase a resting ABG test, a medical consultant (see §§ 404.1616 and 416.1016 of this chapter), preferably one with experience in the care of people with respiratory disorders, must review your case record to determine if we need the test. The medical source we designate to administer the test is solely responsible for deciding whether it is safe for you to do the test and for how to administer it.
3. Exercise ABG tests.
a. We will not purchase an exercise ABG test.
b. We have the following requirements for exercise ABG tests under these listings:
(i) You must have done the exercise under steady state conditions while breathing room air. If you were tested on a treadmill, you generally must have exercised for at least 4 minutes at a grade and speed providing oxygen (O2) consumption of approximately 17.5 milliliters per kilogram per minute (mL/kg/min) or 5.0 metabolic equivalents (METs). If you were tested on a cycle ergometer, you generally must have exercised for at least 4 minutes at an exercise equivalent of 5.0 METs.
(ii) We may use a test in which you have not exercised for at least 4 minutes. If you were unable to complete at least 4 minutes of steady state exercise, we need a statement by the person administering the test about whether the results are a valid indication of your respiratory status. For example, this statement may include information about your cooperation or effort in doing the test and whether you were limited in completing the test because of your respiratory disorder or another impairment.
c. The exercise ABG test report must include the following information:
(i) Your name, the date of the test, and either the altitude or both the city and state of the test site.
(ii) The PaO2 and PaCO2 values.
H. What is pulse oximetry, and what are our requirements for an acceptable test and report?
1. Pulse oximetry measures SpO2, the percentage of oxygen saturation of blood hemoglobin. We use a pulse oximetry measurement (either at rest, during a 6MWT, or after a 6MWT) to evaluate your respiratory disorder under 3.02C3 or, if you have CF, to evaluate it under 3.04F.
2. We have the following requirements for pulse oximetry under 3.02C3:
a. You must be medically stable at the time of the test. See 3.00E2a.
b. Your pulse oximetry measurement must be recorded while you are breathing room air; that is, without oxygen supplementation.
c. Your pulse oximetry measurement must be stable. By “stable,” we mean that the range of SpO2 values (that is, lowest to highest) during any 15-second interval cannot exceed 2 percentage points. For example: (1) The measurement is stable if the lowest SpO2 value during a 15-second interval is 87 percent and the highest value is 89 percent - a range of 2 percentage points. (2) The measurement is not stable if the lowest value is 86 percent and the highest value is 89 percent - a range of 3 percentage points.
d. If you have had more than one measurement (for example, at rest and after a 6MWT), we will use the measurement with the lowest SpO2 value.
e. The pulse oximetry report must include the following information:
(i) Your name, the date of the test, and either the altitude or both the city and State of the test site.
(ii) A graphical printout showing your SpO2 value and a concurrent, acceptable pulse wave. An acceptable pulse wave is one that shows the characteristic pulse wave; that is, sawtooth-shaped with a rapid systolic upstroke (nearly vertical) followed by a slower diastolic downstroke (angled downward).
f. We may need to purchase pulse oximetry at rest to determine whether your disorder meets 3.02C3 when we have evidence showing that you have a chronic respiratory disorder that could result in impaired gas exchange, unless we can make a fully favorable determination or decision on another basis. We may purchase pulse oximetry during and after a 6MWT if your SpO2 value at rest is greater than the value in Table V.
g. Before we purchase pulse oximetry, a medical consultant (see §§ 404.1616 and 416.1016 of this chapter), preferably one with experience in the care of people with respiratory disorders, must review your case record to determine if we need the test. The medical source we designate to administer the test is solely responsible for deciding whether it is safe for you to do the test and for how to administer it.
3. We have the following requirements for pulse oximetry under 3.04F:
a. You must be medically stable at the time of the test. See 3.00E2a.
b. Your pulse oximetry measurement must be recorded while you are breathing room air; that is, without oxygen supplementation.
c. If you have had more than one measurement (for example, at rest and after a 6MWT), we will use the measurement with the lowest SpO2 value.
d. The pulse oximetry report must include your name, the date of the test, and either the altitude or both the city and State of the test site. If you have CF, we do not require a graphical printout showing your SpO2 value and a concurrent, acceptable pulse wave.
I. What is asthma and how do we evaluate it?
1. Asthma is a chronic inflammatory disorder of the lung airways that we evaluate under 3.02 or 3.03. If you have respiratory failure resulting from chronic asthma (see 3.00N), we will evaluate it under 3.14.
2. For the purposes of 3.03:
a. We need evidence showing that you have listing-level (see Table VI in 3.03A) airflow obstruction at baseline while you are medically stable.
b. The phrase “consider under a disability for 1 year” in 3.03B does not refer to the date on which your disability began, only to the date on which we must reevaluate whether your asthma continues to meet a listing or is otherwise disabling.
c. We determine the onset of your disability based on the facts of your case, but it will be no later than the admission date of your first of three hospitalizations that satisfy the criteria of 3.03B.
J. What is CF and how do we evaluate it?
1. General. We evaluate CF, a genetic disorder that results in abnormal salt and water transport across cell membranes in the lungs, pancreas, and other body organs, under 3.04. We need the evidence described in 3.00J2 to establish that you have CF.
2. Documentation of CF. We need a report signed by a physician (see §§ 404.1513(a) and 416.913(a) of this chapter) showing both a and b:
a. One of the following:
(i) A positive newborn screen for CF; or
(ii) A history of CF in a sibling; or
(iii) Documentation of at least one specific CF phenotype or clinical criterion (for example, chronic sino-pulmonary disease with persistent colonization or infections with typical CF pathogens, pancreatic insufficiency, or salt-loss syndromes); and
b. One of the following definitive laboratory tests:
(i) An elevated sweat chloride concentration equal to or greater than 60 millimoles per L; or
(ii) The identification of two CF gene mutations affecting the CFTR; or
(iii) Characteristic abnormalities in ion transport across the nasal epithelium.
c. When we have the report showing a and b, but it is not signed by a physician, we also need a report from a physician stating that you have CF.
d. When we do not have the report showing a and b, we need a report from a physician that is persuasive that a positive diagnosis of CF was confirmed by an appropriate definitive laboratory test. To be persuasive, this report must include a statement by the physician that you had the appropriate definitive laboratory test for diagnosing CF. The report must provide the test results or explain how your diagnosis was established that is consistent with the prevailing state of medical knowledge and clinical practice.
3. CF pulmonary exacerbations. Examples of CF pulmonary exacerbations include increased cough and sputum production, hemoptysis, increased shortness of breath, increased fatigue, and reduction in pulmonary function. Treatment usually includes intravenous antibiotics and intensified airway clearance therapy (for example, increased frequencies of chest percussion or increased use of inhaled nebulized therapies, such as bronchodilators or mucolytics).
4. For 3.04G, we require any two exacerbations or complications from the list in 3.04G1 through 3.04G4 within a 12-month period. You may have two of the same exacerbation or complication or two different ones.
a. If you have two of the acute exacerbations or complications we describe in 3.04G1 and 3.04G2, there must be at least 30 days between the two.
b. If you have one of the acute exacerbations or complications we describe in 3.04G1 and 3.04G2 and one of the chronic complications we describe in 3.04G3 and 3.04G4, the two can occur during the same time. For example, your CF meets 3.04G if you have the pulmonary hemorrhage we describe in 3.04G2 and the weight loss we describe in 3.04G3 even if the pulmonary hemorrhage occurs during the 90-day period in 3.04G3.
c. Your CF also meets 3.04G if you have both of the chronic complications in 3.04G3 and 3.04G4.
5. CF may also affect other body systems such as digestive or endocrine. If your CF, including pulmonary exacerbations and nonpulmonary complications, does not meet or medically equal a respiratory disorders listing, we may evaluate your CF-related impairments under the listings in the affected body system.
K. What is bronchiectasis and how do we evaluate it? Bronchiectasis is a chronic respiratory disorder that is characterized by abnormal and irreversible dilatation (enlargement) of the airways below the trachea, which may be associated with the accumulation of mucus, bacterial infections, and eventual airway scarring. We require imaging (see 3.00D3) to document this disorder. We evaluate your bronchiectasis under 3.02, or under 3.07 if you are having exacerbations or complications (for example, acute bacterial infections, increased shortness of breath, or coughing up blood) that require hospitalization.
L. What is chronic pulmonary hypertension and how do we evaluate it?
1. Chronic pulmonary hypertension is an increase in the blood pressure of the blood vessels of the lungs. If pulmonary hypertension is not adequately treated, it can eventually result in right heart failure. We evaluate chronic pulmonary hypertension due to any cause under 3.09.
2. Chronic pulmonary hypertension is usually diagnosed by catheterization of the pulmonary artery. We will not purchase cardiac catheterization.
M. How do we evaluate lung transplantation? If you receive a lung transplant (or a lung transplant simultaneously with other organs, such as the heart), we will consider you to be disabled under 3.11 for 3 years from the date of the transplant. After that, we evaluate your residual impairment(s) by considering the adequacy of your post-transplant function, the frequency and severity of any rejection episodes you have, complications in other body systems, and adverse treatment effects. People who receive organ transplants generally have impairments that meet our definition of disability before they undergo transplantation. The phrase “consider under a disability for 3 years” in 3.11 does not refer to the date on which your disability began, only to the date on which we must reevaluate whether your impairment(s) continues to meet a listing or is otherwise disabling. We determine the onset of your disability based on the facts of your case.
N. What is respiratory failure and how do we evaluate it? Respiratory failure is the inability of the lungs to perform their basic function of gas exchange. We evaluate respiratory failure under 3.04D if you have CF-related respiratory failure, or under 3.14 if you have respiratory failure due to any other chronic respiratory disorder. Continuous positive airway pressure does not satisfy the criterion in 3.04D or 3.14, and cannot be substituted as an equivalent finding, for invasive mechanical ventilation or noninvasive ventilation with BiPAP.
O. How do we consider the effects of obesity when we evaluate your respiratory disorder? Obesity is a medically determinable impairment that is often associated with respiratory disorders. Obesity makes it harder for the chest and lungs to expand, which can compromise the ability of the respiratory system to supply adequate oxygen to the body. The combined effects of obesity with a respiratory disorder can be greater than the effects of each of the impairments considered separately. We consider any additional and cumulative effects of your obesity when we determine whether you have a severe respiratory disorder, a listing-level respiratory disorder, a combination of impairments that medically equals the severity of a listed impairment, and when we assess your residual functional capacity.
P. What are sleep-related breathing disorders and how do we evaluate them?
1. Sleep-related breathing disorders (for example, sleep apnea) are characterized by transient episodes of interrupted breathing during sleep, which disrupt normal sleep patterns. Prolonged episodes can result in disorders such as hypoxemia (low blood oxygen) and pulmonary vasoconstriction (restricted blood flow in pulmonary blood vessels). Over time, these disorders may lead to chronic pulmonary hypertension or other complications.
2. We evaluate the complications of sleep-related breathing disorders under the listings in the affected body system(s). For example, we evaluate chronic pulmonary hypertension due to any cause under 3.09; chronic heart failure under 4.02; and disturbances in mood, cognition, and behavior under 12.02 or another appropriate mental disorders listing. We will not purchase polysomnography (sleep study).
Q. How do we evaluate mycobacterial, mycotic, and other chronic infections of the lungs? We evaluate chronic infections of the lungs that result in limitations in your respiratory function under 3.02.
R. How do we evaluate respiratory disorders that do not meet one of these listings?
1. These listings are only examples of common respiratory disorders that we consider severe enough to prevent you from doing any gainful activity. If your impairment(s) does not meet the criteria of any of these listings, we must also consider whether you have an impairment(s) that meets the criteria of a listing in another body system. For example, if your CF has resulted in chronic pancreatic or hepatobiliary disease, we evaluate your impairment under the listings in 5.00.
2. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. See §§ 404.1526 and 416.926 of this chapter. Respiratory disorders may be associated with disorders in other body systems, and we consider the combined effects of multiple impairments when we determine whether they medically equal a listing. If your impairment(s) does not meet or medically equal a listing, you may or may not have the residual functional capacity to engage in substantial gainful activity. We proceed to the fourth step and, if necessary, the fifth step of the sequential evaluation process in §§ 404.1520 and 416.920 of this chapter. We use the rules in §§ 404.1594 and 416.994 of this chapter, as appropriate, when we decide whether you continue to be disabled.
3.01 Category of Impairments, Respiratory Disorders
3.02 Chronic respiratory disorders due to any cause except CF (for CF, see 3.04) with A, B, C, or D:
A. FEV1 (see 3.00E) less than or equal to the value in Table I-A or I-B for your age, gender, and height without shoes (see 3.00E3a).
Table I - FEV1 Criteria for 3.02A
| Height without shoes
(centimeters) < means less than | Height without shoes
(inches) < means less than | Table I-A | Table I-B | ||
|---|---|---|---|---|---|
| Age 18 to attainment of age 20 | Age 20 or older | ||||
| Females FEV1 less than or equal to
(L, BTPS) | Males FEV1 less than or equal to
(L, BTPS) | Females FEV1 less than or equal to
(L, BTPS) | Males FEV1 less than or equal to
(L, BTPS) | ||
| <153.0 | <60.25 | 1.20 | 1.45 | 1.05 | 1.20 |
| 153.0 to <159.0 | 60.25 to <62.50 | 1.30 | 1.55 | 1.15 | 1.35 |
| 159.0 to <164.0 | 62.50 to <64.50 | 1.40 | 1.65 | 1.25 | 1.40 |
| 164.0 to <169.0 | 64.50 to <66.50 | 1.45 | 1.75 | 1.35 | 1.50 |
| 169.0 to <174.0 | 66.50 to <68.50 | 1.55 | 1.85 | 1.45 | 1.60 |
| 174.0 to <180.0 | 68.50 to <70.75 | 1.65 | 2.00 | 1.55 | 1.75 |
| 180.0 to <185.0 | 70.75 to <72.75 | 1.75 | 2.10 | 1.65 | 1.85 |
| 185.0 or more | 72.75 or more | 1.80 | 2.15 | 1.70 | 1.90 |
OR
B. FVC (see 3.00E) less than or equal to the value in Table II-A or II-B for your age, gender, and height without shoes (see 3.00E3a).
| Height without shoes
(centimeters) < means less than | Height without shoes
(inches) < means less than | Table II-A | Table II-B | ||
|---|---|---|---|---|---|
| Age 18 to attainment of age 20 | Age 20 or older | ||||
| Females FVC less than or equal to
(L, BTPS) | Males FVC less than or equal to
(L, BTPS) | Females FVC less than or equal to
(L, BTPS) | Males FVC less than or equal to
(L, BTPS) | ||
| <153.0 | <60.25 | 1.35 | 1.65 | 1.30 | 1.50 |
| 153.0 to <159.0 | 60.25 to <62.50 | 1.50 | 1.80 | 1.40 | 1.65 |
| 159.0 to <164.0 | 62.50 to <64.50 | 1.60 | 1.90 | 1.50 | 1.75 |
| 164.0 to <169.0 | 64.50 to <66.50 | 1.70 | 2.05 | 1.60 | 1.90 |
| 169.0 to <174.0 | 66.50 to <68.50 | 1.80 | 2.20 | 1.70 | 2.00 |
| 174.0 to <180.0 | 68.50 to <70.75 | 1.90 | 2.35 | 1.85 | 2.20 |
| 180.0 to <185.0 | 70.75 to <72.75 | 2.05 | 2.50 | 1.95 | 2.30 |
| 185.0 or more | 72.75 or more | 2.10 | 2.60 | 2.00 | 2.40 |
OR
C. Chronic impairment of gas exchange demonstrated by 1, 2, or 3:
1. Average of two unadjusted, single-breath DLCO measurements (see 3.00F) less than or equal to the value in Table III for your gender and height without shoes (see 3.00F3a); or
Table III - DLCO Criteria for 3.02C1
| Height without shoes
(centimeters) < means less than | Height without shoes
(inches) < means less than | Females DLCO less than or equal to
(mL CO (STPD)/min/mmHg) | Males DLCO less than or equal to
(mL CO (STPD)/min/mmHg) |
|---|---|---|---|
| <153.0 | < 60.25 | 8.0 | 9.0 |
| 153.0 to <159.0 | 60.25 to <62.50 | 8.5 | 9.5 |
| 159.0 to <164.0 | 62.50 to <64.50 | 9.0 | 10.0 |
| 164.0 to <169.0 | 64.50 to <66.50 | 9.5 | 10.5 |
| 169.0 to <174.0 | 66.50 to <68.50 | 10.0 | 11.0 |
| 174.0 to <180.0 | 68.50 to <70.75 | 10.5 | 11.5 |
| 180.0 to <185.0 | 70.75 to <72.75 | 11.0 | 12.0 |
| 185.0 or more | 72.75 or more | 11.5 | 12.5 |
2. Arterial PaO2 and PaCO2 measured concurrently by an ABG test, while at rest or during steady state exercise, breathing room air (see 3.00G3b), less than or equal to the applicable values in Table IV-A, IV-B, or IV-C; or
Tables IV-A, IV-B, and IV-C - ABG Criteria for 3.02C2
Table IV-A
[Applicable at test sites less than 3,000 feet above sea level]
| Arterial PaCO2 (mm Hg) and | Arterial PaO2 less than or equal to
(mm Hg) |
|---|---|
| 30 or below | 65 |
| 31 | 64 |
| 32 | 63 |
| 33 | 62 |
| 34 | 61 |
| 35 | 60 |
| 36 | 59 |
| 37 | 58 |
| 38 | 57 |
| 39 | 56 |
| 40 or above | 55 |
Table IV-B
[Applicable at test sites from 3,000 through 6,000 feet above sea level]
| Arterial PaCO2 (mm Hg) and | Arterial PaO2 less than or equal to
(mm Hg) |
|---|---|
| 30 or below | 60 |
| 31 | 59 |
| 32 | 58 |
| 33 | 57 |
| 34 | 56 |
| 35 | 55 |
| 36 | 54 |
| 37 | 53 |
| 38 | 52 |
| 39 | 51 |
| 40 or above | 50 |
Table IV-C
[Applicable at test sites over 6,000 feet above sea level]
| Arterial PaCO2 (mm Hg) and | Arterial PaO2 less than or equal to
(mm Hg) |
|---|---|
| 30 or below | 55 |
| 31 | 54 |
| 32 | 53 |
| 33 | 52 |
| 34 | 51 |
| 35 | 50 |
| 36 | 49 |
| 37 | 48 |
| 38 | 47 |
| 39 | 46 |
| 40 or above | 45 |
3. SpO2 measured by pulse oximetry (see 3.00H2) either at rest, during a 6MWT, or after a 6MWT, less than or equal to the value in Table V.
Table V - SpO2 Criteria for 3.02C3
| Test site altitude
(feet above sea level) | SpO2 less than or equal to |
|---|---|
| Less than 3,000 | 87 percent. |
| 3,000 through 6,000 | 85 percent. |
| Over 6,000 | 83 percent. |
OR
D. Exacerbations or complications requiring three hospitalizations within a 12-month period and at least 30 days apart (the 12-month period must occur within the period we are considering in connection with your application or continuing disability review). Each hospitalization must last at least 48 hours, including hours in a hospital emergency department immediately before the hospitalization.
3.03 Asthma (see 3.00I), with both A and B:
A. FEV1 (see 3.00E1) less than or equal to the value in Table VI-A or VI-B for your age, gender, and height without shoes (see 3.00E3a) measured within the same 12-month period as the hospitalizations in 3.03B.
Table VI - FEV1 Criteria for 3.03A
| Height without shoes
(centimeters) < means less than | Height without shoes
(inches) < means less than | Table VI-A | Table VI-B | ||
|---|---|---|---|---|---|
| Age 18 to attainment of age 20 | Age 20 or older | ||||
| Females FEV1
less than or equal to (L, BTPS) | Males
FEV1 less than or equal to (L, BTPS) | Females FEV1
less than or equal to (L, BTPS) | Males
FEV1 less than or equal to (L, BTPS) | ||
| <153.0 | <60.25 | 1.65 | 1.90 | 1.45 | 1.60 |
| 153.0 to <159.0 | 60.25 to <62.50 | 1.75 | 2.05 | 1.55 | 1.75 |
| 159.0 to <164.0 | 62.50 to <64.50 | 1.85 | 2.15 | 1.65 | 1.90 |
| 164.0 to <169.0 | 64.50 to <66.50 | 1.95 | 2.30 | 1.75 | 2.00 |
| 169.0 to <174.0 | 66.50 to <68.50 | 2.05 | 2.45 | 1.85 | 2.15 |
| 174.0 to <180.0 | 68.50 to <70.75 | 2.20 | 2.60 | 2.00 | 2.30 |
| 180.0 to <185.0 | 70.75 to <72.75 | 2.35 | 2.75 | 2.10 | 2.45 |
| 185.0 or more | 72.75 or more | 2.40 | 2.85 | 2.20 | 2.55 |
AND
B. Exacerbations or complications requiring three hospitalizations within a 12-month period and at least 30 days apart (the 12-month period must occur within the period we are considering in connection with your application or continuing disability review). Each hospitalization must last at least 48 hours, including hours in a hospital emergency department immediately before the hospitalization. Consider under a disability for 1 year from the discharge date of the last hospitalization; after that, evaluate the residual impairment(s) under 3.03 or another appropriate listing.
3.04 Cystic fibrosis (documented as described in 3.00J2) with A, B, C, D, E, F, or G:
A. FEV1 (see 3.00E) less than or equal to the value in Table VII-A or VII-B for your age, gender, and height without shoes (see 3.00E3a).
Table VII - FEV1 Criteria for 3.04A
| Height without shoes
(centimeters) < means less than | Height without shoes
(inches) < means less than | Table VII-A | Table VII-B | ||
|---|---|---|---|---|---|
| Age 18 to attainment of age 20 | Age 20 or older | ||||
| Females
FEV1 less than or equal to (L, BTPS) | Males
FEV1 less than or equal to (L, BTPS) | Females
FEV1 less than or equal to (L, BTPS) | Males
FEV1 less than or equal to (L, BTPS) | ||
| <153.0 | <60.25 | 1.65 | 1.90 | 1.45 | 1.60 |
| 153.0 to <159.0 | 60.25 to <62.50 | 1.75 | 2.05 | 1.55 | 1.75 |
| 159.0 to <164.0 | 62.50 to <64.50 | 1.85 | 2.15 | 1.65 | 1.90 |
| 164.0 to <169.0 | 64.50 to <66.50 | 1.95 | 2.30 | 1.75 | 2.00 |
| 169.0 to <174.0 | 66.50 to <68.50 | 2.05 | 2.45 | 1.85 | 2.15 |
| 174.0 to <180.0 | 68.50 to <70.75 | 2.20 | 2.60 | 2.00 | 2.30 |
| 180.0 to <185.0 | 70.75 to <72.75 | 2.35 | 2.75 | 2.10 | 2.45 |
| 185.0 or more | 72.75 or more | 2.40 | 2.85 | 2.20 | 2.55 |
OR
B. Exacerbations or complications (see 3.00J3) requiring three hospitalizations of any length within a 12-month period and at least 30 days apart (the 12-month period must occur within the period we are considering in connection with your application or continuing disability review).
OR
C. Spontaneous pneumothorax, secondary to CF, requiring chest tube placement.
OR
D. Respiratory failure (see 3.00N) requiring invasive mechanical ventilation, noninvasive ventilation with BiPAP, or a combination of both treatments, for a continuous period of at least 48 hours, or for a continuous period of at least 72 hours if postoperatively.
OR
E. Pulmonary hemorrhage requiring vascular embolization to control bleeding.
OR
F. SpO2 measured by pulse oximetry (see 3.00H3) either at rest, during a 6MWT, or after a 6MWT, less than or equal to the value in Table VIII, twice within a 12-month period and at least 30 days apart (the 12-month period must occur within the period we are considering in connection with your application or continuing disability review).
Tables VIII - SpO2 Criteria for 3.04F
| Test site altitude
(feet above sea level) | SpO2 less than or equal to |
|---|---|
| Less than 3,000 | 89 percent. |
| 3,000 through 6,000 | 87 percent. |
| Over 6,000 | 85 percent. |
OR
G. Two of the following exacerbations or complications (either two of the same or two different, see 3.00J3 and 3.00J4) within a 12-month period (the 12-month period must occur within the period we are considering in connection with your application or continuing disability review):
1. Pulmonary exacerbation requiring 10 consecutive days of intravenous antibiotic treatment.
2. Pulmonary hemorrhage (hemoptysis with more than blood-streaked sputum but not requiring vascular embolization) requiring hospitalization of any length.
3. Weight loss requiring daily supplemental enteral nutrition via a gastrostomy for at least 90 consecutive days or parenteral nutrition via a central venous catheter for at least 90 consecutive days.
4. CFRD requiring daily insulin therapy for at least 90 consecutive days.
3.05 [Reserved]
3.06 [Reserved]
3.07 Bronchiectasis (see 3.00K), documented by imaging (see 3.00D3), with exacerbations or complications requiring three hospitalizations within a 12-month period and at least 30 days apart (the 12-month period must occur within the period we are considering in connection with your application or continuing disability review). Each hospitalization must last at least 48 hours, including hours in a hospital emergency department immediately before the hospitalization.
3.08 [Reserved]
3.09 Chronic pulmonary hypertension due to any cause (see 3.00L) documented by mean pulmonary artery pressure equal to or greater than 40 mm Hg as determined by cardiac catheterization while medically stable (see 3.00E2a).
3.10 [Reserved]
3.11 Lung transplantation (see 3.00M). Consider under a disability for 3 years from the date of the transplant; after that, evaluate the residual impairment(s).
3.12 [Reserved]
3.13 [Reserved]
3.14 Respiratory failure (see 3.00N) resulting from any underlying chronic respiratory disorder except CF (for CF, see 3.04D), requiring invasive mechanical ventilation, noninvasive ventilation with BiPAP, or a combination of both treatments, for a continuous period of at least 48 hours, or for a continuous period of at least 72 hours if postoperatively, twice within a 12-month period and at least 30 days apart (the 12-month period must occur within the period we are considering in connection with your application or continuing disability review).
4.00 Cardiovascular System
A. General
1. What do we mean by a cardiovascular impairment?
a. We mean any disorder that affects the proper functioning of the heart or the circulatory system (that is, arteries, veins, capillaries, and the lymphatic drainage). The disorder can be congenital or acquired.
b. Cardiovascular impairment results from one or more of four consequences of heart disease:
(i) Chronic heart failure or ventricular dysfunction.
(ii) Discomfort or pain due to myocardial ischemia, with or without necrosis of heart muscle.
(iii) Syncope, or near syncope, due to inadequate cerebral perfusion from any cardiac cause, such as obstruction of flow or disturbance in rhythm or conduction resulting in inadequate cardiac output.
(iv) Central cyanosis due to right-to-left shunt, reduced oxygen concentration in the arterial blood, or pulmonary vascular disease.
c. Disorders of the veins or arteries (for example, obstruction, rupture, or aneurysm) may cause impairments of the lower extremities (peripheral vascular disease), the central nervous system, the eyes, the kidneys, and other organs. We will evaluate peripheral vascular disease under 4.11 or 4.12 and impairments of another body system(s) under the listings for that body system(s).
2. What do we consider in evaluating cardiovascular impairments? The listings in this section describe cardiovascular impairments based on symptoms, signs, laboratory findings, response to a regimen of prescribed treatment, and functional limitations.
3. What do the following terms or phrases mean in these listings?
a. Medical consultant is an individual defined in §§ 404.1616(a) and 416.1016(a). This term does not include medical sources who provide consultative examinations for us. We use the abbreviation “MC” throughout this section to designate a medical consultant.
b. Persistent means that the longitudinal clinical record shows that, with few exceptions, the required finding(s) has been present, or is expected to be present, for a continuous period of at least 12 months, such that a pattern of continuing severity is established.
c. Recurrent means that the longitudinal clinical record shows that, within a consecutive 12-month period, the finding(s) occurs at least three times, with intervening periods of improvement of sufficient duration that it is clear that separate events are involved.
d. Appropriate medically acceptable imaging means that the technique used is the proper one to evaluate and diagnose the impairment and is commonly recognized as accurate for assessing the cited finding.
e. A consecutive 12-month period means a period of 12 consecutive months, all or part of which must occur within the period we are considering in connection with an application or continuing disability review.
f. Uncontrolled means the impairment does not adequately respond to standard prescribed medical treatment.
B. Documenting Cardiovascular Impairment
1. What basic documentation do we need? We need sufficiently detailed reports of history, physical examinations, laboratory studies, and any prescribed treatment and response to allow us to assess the severity and duration of your cardiovascular impairment. A longitudinal clinical record covering a period of not less than 3 months of observations and treatment is usually necessary, unless we can make a determination or decision based on the current evidence.
2. Why is a longitudinal clinical record important? We will usually need a longitudinal clinical record to assess the severity and expected duration of your impairment(s). If you have a listing-level impairment, you probably will have received medically prescribed treatment. Whenever there is evidence of such treatment, your longitudinal clinical record should include a description of the ongoing management and evaluation provided by your treating or other medical source. It should also include your response to this medical management, as well as information about the nature and severity of your impairment. The record will provide us with information on your functional status over an extended period of time and show whether your ability to function is improving, worsening, or unchanging.
3. What if you have not received ongoing medical treatment?
a. You may not have received ongoing treatment or have an ongoing relationship with the medical community despite the existence of a severe impairment(s). In this situation, we will base our evaluation on the current objective medical evidence and the other evidence we have. If you do not receive treatment, you cannot show an impairment that meets the criteria of most of these listings. However, we may find you disabled because you have another impairment(s) that in combination with your cardiovascular impairment medically equals the severity of a listed impairment or based on consideration of your residual functional capacity and age, education, and work experience.
b. Unless we can decide your claim favorably on the basis of the current evidence, a longitudinal record is still important. In rare instances where there is no or insufficient longitudinal evidence, we may purchase a consultative examination(s) to help us establish the severity and duration of your impairment.
4. When will we wait before we ask for more evidence?
a. We will wait when we have information showing that your impairment is not yet stable and the expected change in your impairment might affect our determination or decision. In these situations, we need to wait to properly evaluate the severity and duration of your impairment during a stable period. Examples of when we might wait are:
(i) If you have had a recent acute event; for example, a myocardial infarction (heart attack).
(ii) If you have recently had a corrective cardiac procedure; for example, coronary artery bypass grafting.
(iii) If you have started new drug therapy and your response to this treatment has not yet been established; for example, beta-blocker therapy for dilated congestive cardiomyopathy.
b. In these situations, we will obtain more evidence 3 months following the event before we evaluate your impairment. However, we will not wait if we have enough information to make a determination or decision based on all of the relevant evidence in your case.
5. Will we purchase any studies? In appropriate situations, we will purchase studies necessary to substantiate the diagnosis or to document the severity of your impairment, generally after we have evaluated the medical and other evidence we already have. We will not purchase studies involving exercise testing if there is significant risk involved or if there is another medical reason not to perform the test. We will follow sections 4.00C6, 4.00C7, and 4.00C8 when we decide whether to purchase exercise testing.
6. What studies will we not purchase? We will not purchase any studies involving cardiac catheterization, such as coronary angiography, arteriograms, or electrophysiological studies. However, if the results of catheterization are part of the existing evidence we have, we will consider them together with the other relevant evidence. See 4.00C15a.
C. Using Cardiovascular Test Results
1. What is an ECG?
a. ECG stands for electrocardiograph or electrocardiogram. An electrocardiograph is a machine that records electrical impulses of your heart on a strip of paper called an electrocardiogram or a tracing. To record the ECG, a technician positions a number of small contacts (or leads) on your arms, legs, and across your chest to connect them to the ECG machine. An ECG may be done while you are resting or exercising.
b. The ECG tracing may indicate that you have a heart abnormality. It may indicate that your heart muscle is not getting as much oxygen as it needs (ischemia), that your heart rhythm is abnormal (arrhythmia), or that there are other abnormalities of your heart, such as left ventricular enlargement.
2. How do we evaluate ECG evidence? We consider a number of factors when we evaluate ECG evidence:
a. An original or legible copy of the 12-lead ECG obtained at rest must be appropriately dated and labeled, with the standardization inscribed on the tracing. Alteration in standardization of specific leads (such as to accommodate large QRS amplitudes) must be identified on those leads.
(i) Detailed descriptions or computer-averaged signals without original or legible copies of the ECG as described in listing 4.00C2a are not acceptable.
(ii) The effects of drugs or electrolyte abnormalities must be considered as possible noncardiac causes of ECG abnormalities of ventricular repolarization; that is, those involving the ST segment and T wave. If available, the predrug (especially digitalis glycosides) ECG should be submitted.
b. ECGs obtained in conjunction with treadmill, bicycle, or arm exercise tests should meet the following specifications:
(i) ECG reports must include the original calibrated ECG tracings or a legible copy.
(ii) A 12-lead baseline ECG must be recorded in the upright position before exercise.
(iii) A 12-lead ECG should be recorded at the end of each minute of exercise.
(iv) If ECG documentation of the effects of hyperventilation is obtained, the exercise test should be deferred for at least 10 minutes because metabolic changes of hyperventilation may alter the physiologic and ECG-recorded response to exercise.
(v) Post-exercise ECGs should be recorded using a generally accepted protocol consistent with the prevailing state of medical knowledge and clinical practice.
(vi) All resting, exercise, and recovery ECG strips must have the standardization inscribed on the tracing. The ECG strips should be labeled to indicate the date, the times recorded and the relationship to the stage of the exercise protocol. The speed and grade (treadmill test) or work rate (bicycle or arm ergometric test) should be recorded. The highest level of exercise achieved, heart rate and blood pressure levels during testing, and the reason(s) for terminating the test (including limiting signs or symptoms) must be recorded.
3. What are exercise tests and what are they used for?
a. Exercise tests have you perform physical activity and record how your cardiovascular system responds. Exercise tests usually involve walking on a treadmill, but other forms of exercise, such as an exercise bicycle or an arm exercise machine, may be used. Exercise testing may be done for various reasons; such as to evaluate the severity of your coronary artery disease or peripheral vascular disease or to evaluate your progress after a cardiac procedure or an acute event, like a myocardial infarction (heart attack). Exercise testing is the most widely used testing for identifying the presence of myocardial ischemia and for estimating maximal aerobic capacity (usually expressed in METs - metabolic equivalents) if you have heart disease.
b. We include exercise tolerance test (ETT) criteria in 4.02B3 (chronic heart failure) and 4.04A (ischemic heart disease). To meet the ETT criteria in these listings, the ETT must be a sign-or symptom-limited test in which you exercise while connected to an ECG until you develop a sign or symptom that indicates that you have exercised as much as is considered safe for you.
c. In 4.12B, we also refer to exercise testing for peripheral vascular disease. In this test, you walk on a treadmill, usually for a specified period of time, and the individual who administers the test measures the effect of exercise on the flow of blood in your legs, usually by using ultrasound. The test is also called an exercise Doppler test. Even though this test is intended to evaluate peripheral vascular disease, it will be stopped for your safety if you develop abnormal signs or symptoms because of heart disease.
d. Each type of test is done in a certain way following specific criteria, called a protocol. For our program, we also specify certain aspects of how any exercise test we purchase is to be done. See 4.00C10 and 4.00C17.
4. Do ETTs have limitations? An ETT provides an estimate of aerobic capacity for walking on a grade, bicycling, or moving one's arms in an environmentally controlled setting. Therefore, ETT results do not correlate with the ability to perform other types of exertional activities, such as lifting and carrying heavy loads, and do not provide an estimate of the ability to perform activities required for work in all possible work environments or throughout a workday. Also, certain medications (such as beta blockers) and conduction disorders (such as left or right bundle branch blocks) can cause false-negative or false-positive results. Therefore, we must consider the results of an ETT together with all the other relevant evidence in your case record.
5. How does an ETT with measurement of maximal or peak oxygen uptake VO2) differ from other ETTs? Occasionally, medical evidence will include the results of an ETT with VO2 While ETTs without measurement of VO2 provide only an estimate of aerobic capacity, measured maximal or peak oxygen uptake provides an accurate measurement of aerobic capacity, which is often expressed in METs (metabolic equivalents). The MET level may not be indicated in the report of attained maximal or peak VO2 testing, but can be calculated as follows: 1 MET = 3.5 milliliters (ml) of oxygen uptake per kilogram (kg) of body weight per minute. For example, a 70 kg (154 lb.) individual who achieves a maximal or peak VO2 of 1225 ml in 1 minute has attained 5 METs (1225 ml/70 kg/1 min = 17.5 ml/kg/min. 17.5/3.5 = 5 METs).
6. When will we consider whether to purchase an exercise test?
a. We will consider whether to purchase an exercise test when:
(i) There is a question whether your cardiovascular impairment meets or medically equals the severity of one of the listings, or there is no timely test in the evidence we have (see 4.00C9), and we cannot find you disabled on some other basis; or
(ii) We need to assess your residual functional capacity and there is insufficient evidence in the record to make a determination or decision.
b. We will not purchase an exercise test when we can make our determination or decision based on the evidence we already have.
7. What must we do before purchasing an exercise test?
a. Before we purchase an exercise test, an MC, preferably one with experience in the care of patients with cardiovascular disease, must review the pertinent history, physical examinations, and laboratory tests that we have to determine whether the test would present a significant risk to you or if there is some other medical reason not to purchase the test (see 4.00C8).
b. If you are under the care of a treating source (see §§ 404.1502 and 416.902) for a cardiovascular impairment, this source has not performed an exercise test, and there are no reported significant risks to testing, we will request a statement from that source explaining why it was not done or should not be done before we decide whether we will purchase the test.
c. The MC, in accordance with the regulations and other instructions on consultative examinations, will generally give great weight to the treating source's opinion about the risk of exercise testing to you and will generally not override it. In the rare situation in which the MC does override the treating source's opinion, the MC must prepare a written rationale documenting the reasons for overriding the opinion.
d. If you do not have a treating source or we cannot obtain a statement from your treating source, the MC is responsible for assessing the risk to exercise testing based on a review of the records we have before purchasing an exercise test for you.
e. We must also provide your records to the medical source who performs the exercise test for review prior to conducting the test if the source does not already have them. The medical source who performs the exercise test has the ultimate responsibility for deciding whether you would be at risk.
8. When will we not purchase an exercise test or wait before we purchase an exercise test?
a. We will not purchase an exercise test when an MC finds that you have one of the following significant risk factors:
(i) Unstable angina not previously stabilized by medical treatment.
(ii) Uncontrolled cardiac arrhythmias causing symptoms or hemodynamic compromise.
(iii) An implanted cardiac defibrillator.
(iv) Symptomatic severe aortic stenosis.
(v) Uncontrolled symptomatic heart failure.
(vi) Aortic dissection.
(vii) Severe pulmonary hypertension (pulmonary artery systolic pressure greater than 60 mm Hg).
(viii) Left main coronary stenosis of 50 percent or greater that has not been bypassed.
(ix) Moderate stenotic valvular disease with a systolic gradient across the aortic valve of 50 mm Hg or greater.
(x) Severe arterial hypertension (systolic greater than 200 mm Hg or diastolic greater than 110 mm Hg).
(xi) Hypertrophic cardiomyopathy with a systolic gradient of 50 mm Hg or greater.
b. We also will not purchase an exercise test when you are prevented from performing exercise testing due to another impairment affecting your ability to use your arms and legs.
c. We will not purchase an ETT to document the presence of a cardiac arrhythmia.
d. We will wait to purchase an exercise test until 3 months after you have had one of the following events. This will allow for maximal, attainable restoration of functional capacity.
(i) Acute myocardial infarction.
(ii) Surgical myocardial revascularization (bypass surgery).
(iii) Other open-heart surgical procedures.
(iv) Percutaneous transluminal coronary angioplasty with or without stenting.
e. If you are deconditioned after an extended period of bedrest or inactivity and could improve with activity, or if you are in acute heart failure and are expected to improve with treatment, we will wait an appropriate period of time for you to recuperate before we purchase an exercise test.
9. What do we mean by a “timely” test?
a. We consider exercise test results to be timely for 12 months after the date they are performed, provided there has been no change in your clinical status that may alter the severity of your cardiovascular impairment.
b. However, an exercise test that is older than 12 months, especially an abnormal one, can still provide information important to our adjudication. For example, a test that is more than 12 months old can provide evidence of ischemic heart disease or peripheral vascular disease, information on decreased aerobic capacity, or information about the duration or onset of your impairment. Such tests can be an important component of the longitudinal record.
c. When we evaluate a test that is more than 12 months old, we must consider the results in the context of all the relevant evidence, including why the test was performed and whether there has been an intervening event or improvement or worsening of your impairment.
d. We will purchase a new exercise test only if we cannot make a determination or decision based on the evidence we have.
10. How must ETTs we purchase be performed?
a. The ETT must be a sign- or symptom-limited test characterized by a progressive multistage regimen. It must be performed using a generally accepted protocol consistent with the prevailing state of medical knowledge and clinical practice. A description of the protocol that was followed must be provided, and the test must meet the requirements of 4.00C2b and this section. A radionuclide perfusion scan may be useful for detecting or confirming ischemia when resting ECG abnormalities, medications, or other factors may decrease the accuracy of ECG interpretation of ischemia. (The perfusion imaging is done at the termination of exercise, which may be at a higher MET level than that at which ischemia first occurs. If the imaging confirms the presence of reversible ischemia, the exercise ECG may be useful for detecting the MET level at which ischemia initially appeared.) Exercise tests may also be performed using echocardiography to detect stress-induced ischemia and left ventricular dysfunction (see 4.00C12 and 4.00C13).
b. The exercise test must be paced to your capabilities and be performed following the generally accepted standards for adult exercise test laboratories. With a treadmill test, the speed, grade (incline), and duration of exercise must be recorded for each exercise test stage performed. Other exercise test protocols or techniques should use similar workloads. The exercise protocol may need to be modified in individual cases to allow for a lower initial workload with more slowly graded increments than the standard Bruce protocol.
c. Levels of exercise must be described in terms of workload and duration of each stage; for example, treadmill speed and grade, or bicycle ergometer work rate in kpm/min or watts.
d. The exercise laboratory's physical environment, staffing, and equipment must meet the generally accepted standards for adult exercise test laboratories.
11. How do we evaluate ETT results? We evaluate ETT results on the basis of the work level at which the test becomes abnormal, as documented by onset of signs or symptoms and any ECG or imaging abnormalities. The absence of an ischemic response on an ETT alone does not exclude the diagnosis of ischemic heart disease. We must consider the results of an ETT in the context of all of the other evidence in your case record.
12. When are ETTs done with imaging? When resting ECG abnormalities preclude interpretation of ETT tracings relative to ischemia, a radionuclide (for example, thallium-201 or technetium-99m) perfusion scan or echocardiography in conjunction with an ETT provides better results. You may have resting ECG abnormalities when you have a conduction defect - for example, Wolff-Parkinson-White syndrome, left bundle branch block, left ventricular hypertrophy - or when you are taking digitalis or other antiarrhythmic drugs, or when resting ST changes are present. Also, these techniques can provide a reliable estimate of ejection fraction.
13. Will we purchase ETTs with imaging? We may purchase an ETT with imaging in your case after an MC, preferably one with experience in the care of patients with cardiovascular disease, has reviewed your medical history and physical examination, any report(s) of appropriate medically acceptable imaging, ECGs, and other appropriate tests. We will consider purchasing an ETT with imaging when other information we have is not adequate for us to assess whether you have severe ventricular dysfunction or myocardial ischemia, there is no significant risk involved (see 4.00C8a), and we cannot make our determination or decision based on the evidence we already have.
14. What are drug-induced stress tests? These tests are designed primarily to provide evidence about myocardial ischemia or prior myocardial infarction, but do not require you to exercise. These tests are used when you cannot exercise or cannot exercise enough to achieve the desired cardiac stress. Drug-induced stress tests can also provide evidence about heart chamber dimensions and function; however, these tests do not provide information about your aerobic capacity and cannot be used to help us assess your ability to function. Some of these tests use agents, such as Persantine or adenosine, that dilate the coronary arteries and are used in combination with nuclear agents, such as thallium or technetium (for example, Cardiolyte or Myoview), and a myocardial scan. Other tests use agents, such as dobutamine, that stimulate the heart to contract more forcefully and faster to simulate exercise and are used in combination with a 2-dimensional echocardiogram. We may, when appropriate, purchase a drug-induced stress test to confirm the presence of myocardial ischemia after a review of the evidence in your file by an MC, preferably one with experience in the care of patients with cardiovascular disease.
15. How do we evaluate cardiac catheterization evidence?
a. We will not purchase cardiac catheterization; however, if you have had catheterization, we will make every reasonable effort to obtain the report and any ancillary studies. We will consider the quality and type of data provided and its relevance to the evaluation of your impairment. For adults, we generally see two types of catheterization reports: Coronary arteriography and left ventriculography.
b. For coronary arteriography, the report should provide information citing the method of assessing coronary arterial lumen diameter and the nature and location of obstructive lesions. Drug treatment at baseline and during the procedure should be reported. Some individuals with significant coronary atherosclerotic obstruction have collateral vessels that supply the myocardium distal to the arterial obstruction so that there is no evidence of myocardial damage or ischemia, even with exercise. When the results of quantitative computer measurements and analyses are included in your case record, we will consider them in interpreting the severity of stenotic lesions.
c. For left ventriculography, the report should describe the wall motion of the myocardium with regard to any areas of hypokinesis (abnormally decreased motion), akinesis (lack of motion), or dyskinesis (distortion of motion), and the overall contraction of the ventricle as measured by the ejection fraction. Measurement of chamber volumes and pressures may be useful. Quantitative computer analysis provides precise measurement of segmental left ventricular wall thickness and motion. There is often a poor correlation between left ventricular function at rest and functional capacity for physical activity.
16. What details should exercise Doppler test reports contain? The reports of exercise Doppler tests must describe the level of exercise; for example, the speed and grade of the treadmill settings, the duration of exercise, symptoms during exercise, and the reasons for stopping exercise if the expected level of exercise was not attained. They must also include the blood pressures at the ankle and other pertinent sites measured after exercise and the time required for the systolic blood pressure to return toward or to the pre-exercise level. The graphic tracings, if available, should also be included with the report. All tracings must be annotated with the standardization used by the testing facility.
17. How must exercise Doppler tests we purchase be performed? When we purchase an exercise Doppler test, you must exercise on a treadmill at 2 mph on a 12 percent grade for up to 5 minutes. The reports must include the information specified in 4.00C16. Because this is an exercise test, we must evaluate whether such testing would put you at significant risk, in accordance with the guidance found in 4.00C6, 4.00C7, and 4.00C8.
D. Evaluating Chronic Heart Failure
1. What is chronic heart failure (CHF)?
a. CHF is the inability of the heart to pump enough oxygenated blood to body tissues. This syndrome is characterized by symptoms and signs of pulmonary or systemic congestion (fluid retention) or limited cardiac output. Certain laboratory findings of cardiac functional and structural abnormality support the diagnosis of CHF. There are two main types of CHF:
(i) Predominant systolic dysfunction (the inability of the heart to contract normally and expel sufficient blood), which is characterized by a dilated, poorly contracting left ventricle and reduced ejection fraction (abbreviated EF, it represents the percentage of the blood in the ventricle actually pumped out with each contraction), and
(ii) Predominant diastolic dysfunction (the inability of the heart to relax and fill normally), which is characterized by a thickened ventricular muscle, poor ability of the left ventricle to distend, increased ventricular filling pressure, and a normal or increased EF.
b. CHF is considered in these listings as a single category whether due to atherosclerosis (narrowing of the arteries), cardiomyopathy, hypertension, or rheumatic, congenital, or other heart disease. However, if the CHF is the result of primary pulmonary hypertension secondary to disease of the lung (cor pulmonale), we will evaluate your impairment using 3.09, in the respiratory system listings.
2. What evidence of CHF do we need?
a. Cardiomegaly or ventricular dysfunction must be present and demonstrated by appropriate medically acceptable imaging, such as chest x-ray, echocardiography (M-Mode, 2-dimensional, and Doppler), radionuclide studies, or cardiac catheterization.
(i) Abnormal cardiac imaging showing increased left ventricular end diastolic diameter (LVEDD), decreased EF, increased left atrial chamber size, increased ventricular filling pressures measured at cardiac catheterization, or increased left ventricular wall or septum thickness, provides objective measures of both left ventricular function and structural abnormality in heart failure.
(ii) An LVEDD greater than 6.0 cm or an EF of 30 percent or less measured during a period of stability (that is, not during an episode of acute heart failure) may be associated clinically with systolic failure.
(iii) Left ventricular posterior wall thickness added to septal thickness totaling 2.5 cm or greater with left atrium enlarged to 4.5 cm or greater may be associated clinically with diastolic failure.
(iv) However, these measurements alone do not reflect your functional capacity, which we evaluate by considering all of the relevant evidence. In some situations, we may need to purchase an ETT to help us assess your functional capacity.
(v) Other findings on appropriate medically acceptable imaging may include increased pulmonary vascular markings, pleural effusion, and pulmonary edema. These findings need not be present on each report, since CHF may be controlled by prescribed treatment.
b. To establish that you have chronic heart failure, your medical history and physical examination should describe characteristic symptoms and signs of pulmonary or systemic congestion or of limited cardiac output associated with the abnormal findings on appropriate medically acceptable imaging. When an acute episode of heart failure is triggered by a remediable factor, such as an arrhythmia, dietary sodium overload, or high altitude, cardiac function may be restored and a chronic impairment may not be present.
(i) Symptoms of congestion or of limited cardiac output include easy fatigue, weakness, shortness of breath (dyspnea), cough, or chest discomfort at rest or with activity. Individuals with CHF may also experience shortness of breath on lying flat (orthopnea) or episodes of shortness of breath that wake them from sleep (paroxysmal nocturnal dyspnea). They may also experience cardiac arrhythmias resulting in palpitations, lightheadedness, or fainting.
(ii) Signs of congestion may include hepatomegaly, ascites, increased jugular venous distention or pressure, rales, peripheral edema, or rapid weight gain. However, these signs need not be found on all examinations because fluid retention may be controlled by prescribed treatment.
3. Is it safe for you to have an ETT, if you have CHF? The presence of CHF is not necessarily a contraindication to an ETT, unless you are having an acute episode of heart failure. Measures of cardiac performance are valuable in helping us evaluate your ability to do work-related activities. Exercise testing has been safely used in individuals with CHF; therefore, we may purchase an ETT for evaluation under 4.02B3 if an MC, preferably one experienced in the care of patients with cardiovascular disease, determines that there is no significant risk to you. (See 4.00C6 for when we will consider the purchase of an ETT. See 4.00C7-4.00C8 for what we must do before we purchase an ETT and when we will not purchase one.) ST segment changes from digitalis use in the treatment of CHF do not preclude the purchase of an ETT.
4. How do we evaluate CHF using 4.02?
a. We must have objective evidence, as described in 4.00D2, that you have chronic heart failure.
b. To meet the required level of severity for this listing, your impairment must satisfy the requirements of one of the criteria in A and one of the criteria in B.
c. In 4.02B2, the phrase periods of stabilization means that, for at least 2 weeks between episodes of acute heart failure, there must be objective evidence of clearing of the pulmonary edema or pleural effusions and evidence that you returned to, or you were medically considered able to return to, your prior level of activity.
d. Listing 4.02B3c requires a decrease in systolic blood pressure below the baseline level (taken in the standing position immediately prior to exercise) or below any systolic pressure reading recorded during exercise. This is because, normally, systolic blood pressure and heart rate increase gradually with exercise. Decreases in systolic blood pressure below the baseline level that occur during exercise are often associated with ischemia-induced left ventricular dysfunction resulting in decreased cardiac output. However, a blunted response (that is, failure of the systolic blood pressure to rise 10 mm Hg or more), particularly in the first 3 minutes of exercise, may be drug-related and is not necessarily associated with left ventricular dysfunction. Also, some individuals with increased sympathetic responses because of deconditioning or apprehension may increase their systolic blood pressure and heart rate above their baseline level just before and early into exercise. This can be associated with a drop in systolic pressure in early exercise that is not due to left ventricular dysfunction. Therefore, an early decrease in systolic blood pressure must be interpreted within the total context of the test; that is, the presence or absence of symptoms such as lightheadedness, ischemic changes, or arrhythmias on the ECG.
E. Evaluating Ischemic Heart Disease
1. What is ischemic heart disease (IHD)? IHD results when one or more of your coronary arteries is narrowed or obstructed or, in rare situations, constricted due to vasospasm, interfering with the normal flow of blood to your heart muscle (ischemia). The obstruction may be the result of an embolus, a thrombus, or plaque. When heart muscle tissue dies as a result of the reduced blood supply, it is called a myocardial infarction (heart attack).
2. What causes chest discomfort of myocardial origin?
a. Chest discomfort of myocardial ischemic origin, commonly known as angina pectoris, is usually caused by coronary artery disease (often abbreviated CAD). However, ischemic discomfort may be caused by a noncoronary artery impairment, such as aortic stenosis, hypertrophic cardiomyopathy, pulmonary hypertension, or anemia.
b. Instead of typical angina pectoris, some individuals with IHD experience atypical angina, anginal equivalent, variant angina, or silent ischemia, all of which we may evaluate using 4.04. We discuss the various manifestations of ischemia in 4.00E3-4.00E7.
3. What are the characteristics of typical angina pectoris? Discomfort of myocardial ischemic origin (angina pectoris) is discomfort that is precipitated by effort or emotion and promptly relieved by rest, sublingual nitroglycerin (that is, nitroglycerin tablets that are placed under the tongue), or other rapidly acting nitrates. Typically, the discomfort is located in the chest (usually substernal) and described as pressing, crushing, squeezing, burning, aching, or oppressive. Sharp, sticking, or cramping discomfort is less common. Discomfort occurring with activity or emotion should be described specifically as to timing and usual inciting factors (type and intensity), character, location, radiation, duration, and response to nitrate treatment or rest.
4. What is atypical angina? Atypical angina describes discomfort or pain from myocardial ischemia that is felt in places other than the chest. The common sites of cardiac pain are the inner aspect of the left arm, neck, jaw(s), upper abdomen, and back, but the discomfort or pain can be elsewhere. When pain of cardiac ischemic origin presents in an atypical site in the absence of chest discomfort, the source of the pain may be difficult to diagnose. To represent atypical angina, your discomfort or pain should have precipitating and relieving factors similar to those of typical chest discomfort, and we must have objective medical evidence of myocardial ischemia; for example, ECG or ETT evidence or appropriate medically acceptable imaging.
5. What is anginal equivalent? Often, individuals with IHD will complain of shortness of breath (dyspnea) on exertion without chest pain or discomfort. In a minority of such situations, the shortness of breath is due to myocardial ischemia; this is called anginal equivalent. To represent anginal equivalent, your shortness of breath should have precipitating and relieving factors similar to those of typical chest discomfort, and we must have objective medical evidence of myocardial ischemia; for example, ECG or ETT evidence or appropriate medically acceptable imaging. In these situations, it is essential to establish objective evidence of myocardial ischemia to ensure that you do not have effort dyspnea due to non-ischemic or non-cardiac causes.
6. What is variant angina?
a. Variant angina (Prinzmetal's angina, vasospastic angina) refers to the occurrence of anginal episodes at rest, especially at night, accompanied by transitory ST segment elevation (or, at times, ST depression) on an ECG. It is due to severe spasm of a coronary artery, causing ischemia of the heart wall, and is often accompanied by major ventricular arrhythmias, such as ventricular tachycardia. We will consider variant angina under 4.04 only if you have spasm of a coronary artery in relation to an obstructive lesion of the vessel. If you have an arrhythmia as a result of variant angina, we may consider your impairment under 4.05.
b. Variant angina may also occur in the absence of obstructive coronary disease. In this situation, an ETT will not demonstrate ischemia. The diagnosis will be established by showing the typical transitory ST segment changes during attacks of pain, and the absence of obstructive lesions shown by catheterization. Treatment in cases where there is no obstructive coronary disease is limited to medications that reduce coronary vasospasm, such as calcium channel blockers and nitrates. In such situations, we will consider the frequency of anginal episodes despite prescribed treatment when evaluating your residual functional capacity.
c. Vasospasm that is catheter-induced during coronary angiography is not variant angina.
7. What is silent ischemia?
a. Myocardial ischemia, and even myocardial infarction, can occur without perception of pain or any other symptoms; when this happens, we call it silent ischemia. Pain sensitivity may be altered by a variety of diseases, most notably diabetes mellitus and other neuropathic disorders. Individuals also vary in their threshold for pain.
b. Silent ischemia occurs most often in:
(i) Individuals with documented past myocardial infarction or established angina without prior infarction who do not have chest pain on ETT, but have a positive test with ischemic abnormality on ECG, perfusion scan, or other appropriate medically acceptable imaging.
(ii) Individuals with documented past myocardial infarction or angina who have ST segment changes on ambulatory monitoring (Holter monitoring) that are similar to those that occur during episodes of angina. ST depression shown on the ambulatory recording should not be interpreted as positive for ischemia unless similar depression is also seen during chest pain episodes annotated in the diary that the individual keeps while wearing the Holter monitor.
c. ST depression can result from a variety of factors, such as postural changes and variations in cardiac sympathetic tone. In addition, there are differences in how different Holter monitors record the electrical responses. Therefore, we do not consider the Holter monitor reliable for the diagnosis of silent ischemia except in the situation described in 4.00E7b(ii).
8. What other sources of chest discomfort are there? Chest discomfort of nonischemic origin may result from other cardiac impairments, such as pericarditis. Noncardiac impairments may also produce symptoms mimicking that of myocardial ischemia. These impairments include acute anxiety or panic attacks, gastrointestinal tract disorders, such as esophageal spasm, esophagitis, hiatal hernia, biliary tract disease, gastritis, peptic ulcer, and pancreatitis, and musculoskeletal syndromes, such as chest wall muscle spasm, chest wall syndrome (especially after coronary bypass surgery), costochondritis, and cervical or dorsal spine arthritis. Hyperventilation may also mimic ischemic discomfort. Thus, in the absence of documented myocardial ischemia, such disorders should be considered as possible causes of chest discomfort.
9. How do we evaluate IHD using 4.04?
a. We must have objective evidence, as described under 4.00C, that your symptoms are due to myocardial ischemia.
b. Listing-level changes on the ECG in 4.04A1 are the classically accepted changes of horizontal or downsloping ST depression occurring both during exercise and recovery. Although we recognize that ischemic changes may at times occur only during exercise or recovery, and may at times be upsloping with only junctional ST depression, such changes can be false positive; that is, occur in the absence of ischemia. Diagnosis of ischemia in this situation requires radionuclide or echocardiogram confirmation. See 4.00C12 and 4.00C13.
c. Also in 4.04A1, we require that the depression of the ST segment last for at least 1 minute of recovery because ST depression that occurs during exercise but that rapidly normalizes in recovery is a common false-positive response.
d. In 4.04A2, we specify that the ST elevation must be in non-infarct leads during both exercise and recovery. This is because, in the absence of ECG signs of prior infarction, ST elevation during exercise denotes ischemia, usually severe, requiring immediate termination of exercise. However, if there is baseline ST elevation in association with a prior infarction or ventricular aneurysm, further ST elevation during exercise does not necessarily denote ischemia and could be a false-positive ECG response. Diagnosis of ischemia in this situation requires radionuclide or echocardiogram confirmation. See 4.00C12 and 4.00C13.
e. Listing 4.04A3 requires a decrease in systolic blood pressure below the baseline level (taken in the standing position immediately prior to exercise) or below any systolic pressure reading recorded during exercise. This is the same finding required in 4.02B3c. See 4.00D4d for full details.
f. In 4.04B, each of the three ischemic episodes must require revascularization or be not amenable to treatment. Revascularization means angioplasty (with or without stent placement) or bypass surgery. However, reocclusion that occurs after a revascularization procedure but during the same hospitalization and that requires a second procedure during the same hospitalization will not be counted as another ischemic episode. Not amenable means that the revascularization procedure could not be done because of another medical impairment or because the vessel was not suitable for revascularization.
g. We will use 4.04C only when you have symptoms due to myocardial ischemia as described in 4.00E3-4.00E7 while on a regimen of prescribed treatment, you are at risk for exercise testing (see 4.00C8), and we do not have a timely ETT or a timely normal drug-induced stress test for you. See 4.00C9 for what we mean by a timely test.
h. In 4.04C1 the term nonbypassed means that the blockage is in a vessel that is potentially bypassable; that is, large enough to be bypassed and considered to be a cause of your ischemia. These vessels are usually major arteries or one of a major artery's major branches. A vessel that has become obstructed again after angioplasty or stent placement and has remained obstructed or is not amenable to another revascularization is considered a nonbypassed vessel for purposes of this listing. When you have had revascularization, we will not use the pre-operative findings to assess the current severity of your coronary artery disease under 4.04C, although we will consider the severity and duration of your impairment prior to your surgery in making our determination or decision.
F. Evaluating Arrhythmias
1. What is an arrhythmia? An arrhythmia is a change in the regular beat of the heart. Your heart may seem to skip a beat or beat irregularly, very quickly (tachycardia), or very slowly (bradycardia).
2. What are the different types of arrhythmias?
a. There are many types of arrhythmias. Arrhythmias are identified by where they occur in the heart (atria or ventricles) and by what happens to the heart's rhythm when they occur.
b. Arrhythmias arising in the cardiac atria (upper chambers of the heart) are called atrial or supraventricular arrhythmias. Ventricular arrhythmias begin in the ventricles (lower chambers). In general, ventricular arrhythmias caused by heart disease are the most serious.
3. How do we evaluate arrhythmias using 4.05?
a. We will use 4.05 when you have arrhythmias that are not fully controlled by medication, an implanted pacemaker, or an implanted cardiac defibrillator and you have uncontrolled recurrent episodes of syncope or near syncope. If your arrhythmias are controlled, we will evaluate your underlying heart disease using the appropriate listing. For other considerations when we evaluate arrhythmias in the presence of an implanted cardiac defibrillator, see 4.00F4.
b. We consider near syncope to be a period of altered consciousness, since syncope is a loss of consciousness or a faint. It is not merely a feeling of light-headedness, momentary weakness, or dizziness.
c. For purposes of 4.05, there must be a documented association between the syncope or near syncope and the recurrent arrhythmia. The recurrent arrhythmia, not some other cardiac or non-cardiac disorder, must be established as the cause of the associated symptom. This documentation of the association between the symptoms and the arrhythmia may come from the usual diagnostic methods, including Holter monitoring (also called ambulatory electrocardiography) and tilt-table testing with a concurrent ECG. Although an arrhythmia may be a coincidental finding on an ETT, we will not purchase an ETT to document the presence of a cardiac arrhythmia.
4. What will we consider when you have an implanted cardiac defibrillator and you do not have arrhythmias that meet the requirements of 4.05?
a. Implanted cardiac defibrillators are used to prevent sudden cardiac death in individuals who have had, or are at high risk for, cardiac arrest from life-threatening ventricular arrhythmias. The largest group at risk for sudden cardiac death consists of individuals with cardiomyopathy (ischemic or non-ischemic) and reduced ventricular function. However, life-threatening ventricular arrhythmias can also occur in individuals with little or no ventricular dysfunction. The shock from the implanted cardiac defibrillator is a unique form of treatment; it rescues an individual from what may have been cardiac arrest. However, as a consequence of the shock(s), individuals may experience psychological distress, which we may evaluate under the mental disorders listings in 12.00ff.
b. Most implantable cardiac defibrillators have rhythm-correcting and pacemaker capabilities. In some individuals, these functions may result in the termination of ventricular arrhythmias without an otherwise painful shock. (The shock is like being kicked in the chest.) Implanted cardiac defibrillators may deliver inappropriate shocks, often repeatedly, in response to benign arrhythmias or electrical malfunction. Also, exposure to strong electrical or magnetic fields, such as from MRI (magnetic resonance imaging), can trigger or reprogram an implanted cardiac defibrillator, resulting in inappropriate shocks. We must consider the frequency of, and the reason(s) for, the shocks when evaluating the severity and duration of your impairment.
c. In general, the exercise limitations imposed on individuals with an implanted cardiac defibrillator are those dictated by the underlying heart impairment. However, the exercise limitations may be greater when the implanted cardiac defibrillator delivers an inappropriate shock in response to the increase in heart rate with exercise, or when there is exercise-induced ventricular arrhythmia.
G. Evaluating Peripheral Vascular Disease
1. What is peripheral vascular disease (PVD)? Generally, PVD is any impairment that affects either the arteries (peripheral arterial disease) or the veins (venous insufficiency) in the extremities, particularly the lower extremities. The usual effect is blockage of the flow of blood either from the heart (arterial) or back to the heart (venous). If you have peripheral arterial disease, you may have pain in your calf after walking a distance that goes away when you rest (intermittent claudication); at more advanced stages, you may have pain in your calf at rest or you may develop ulceration or gangrene. If you have venous insufficiency, you may have swelling, varicose veins, skin pigmentation changes, or skin ulceration.
2. How do we assess limitations resulting from PVD? We will assess your limitations based on your symptoms together with physical findings, Doppler studies, other appropriate non-invasive studies, or angiographic findings. However, if the PVD has resulted in amputation, we will evaluate any limitations related to the amputation under the musculoskeletal listings, 1.00ff.
3. What is brawny edema? Brawny edema (4.11A) is swelling that is usually dense and feels firm due to the presence of increased connective tissue; it is also associated with characteristic skin pigmentation changes. It is not the same thing as pitting edema. Brawny edema generally does not pit (indent on pressure), and the terms are not interchangeable. Pitting edema does not satisfy the requirements of 4.11A.
4. What is lymphedema and how will we evaluate it?
a. Lymphedema is edema of the extremities due to a disorder of the lymphatic circulation; at its worst, it is called elephantiasis. Primary lymphedema is caused by abnormal development of lymph vessels and may be present at birth (congenital lymphedema), but more often develops during the teens (lymphedema praecox). It may also appear later, usually after age 35 (lymphedema tarda). Secondary lymphedema is due to obstruction or destruction of normal lymphatic channels due to tumor, surgery, repeated infections, or parasitic infection such as filariasis. Lymphedema most commonly affects one extremity.
b. Lymphedema does not meet the requirements of 4.11, although it may medically equal the severity of that listing. We will evaluate lymphedema by considering whether the underlying cause meets or medically equals any listing or whether the lymphedema medically equals a cardiovascular listing, such as 4.11, or a musculoskeletal disorders listing, such as 1.18. If no listing is met or medically equaled, we will evaluate any functional limitations imposed by your lymphedema when we assess your residual functional capacity.
5. When will we purchase exercise Doppler studies for evaluating peripheral arterial disease (PAD)? If we need additional evidence of your PAD, we will generally purchase exercise Doppler studies (see 4.00C16 and 4.00C17) when your resting ankle/brachial systolic blood pressure ratio is at least 0.50 but less than 0.80, and only rarely when it is 0.80 or above. We will not purchase exercise Doppler testing if you have a disease that results in abnormal arterial calcification or small vessel disease, but will use your resting toe systolic blood pressure or resting toe/brachial systolic blood pressure ratio. (See 4.00G7c and 4.00G8.) There are no current medical standards for evaluating exercise toe pressures. Because any exercise test stresses your entire cardiovascular system, we will purchase exercise Doppler studies only after an MC, preferably one with experience in the care of patients with cardiovascular disease, has determined that the test would not present a significant risk to you and that there is no other medical reason not to purchase the test (see 4.00C6, 4.00C7, and 4.00C8).
6. Are there any other studies that are helpful in evaluating PAD? Doppler studies done using a recording ultrasonic Doppler unit and strain-gauge plethysmography are other useful tools for evaluating PAD. A recording Doppler, which prints a tracing of the arterial pulse wave in the femoral, popliteal, dorsalis pedis, and posterior tibial arteries, is an excellent evaluation tool to compare wave forms in normal and compromised peripheral blood flow. Qualitative analysis of the pulse wave is very helpful in the overall assessment of the severity of the occlusive disease. Tracings are especially helpful in assessing severity if you have small vessel disease related to diabetes mellitus or other diseases with similar vascular changes, or diseases causing medial calcifications when ankle pressure is either normal or falsely high.
7. How do we evaluate PAD under 4.12?
a. The ankle blood pressure referred to in 4.12A and B is the higher of the pressures recorded from the posterior tibial and dorsalis pedis arteries in the affected leg. The higher pressure recorded from the two sites is the more significant measurement in assessing the extent of arterial insufficiency. Techniques for obtaining ankle systolic blood pressures include Doppler (See 4.00C16 and 4.00C17), plethysmographic studies, or other techniques. We will request any available tracings generated by these studies so that we can review them.
b. In 4.12A, the ankle/brachial systolic blood pressure ratio is the ratio of the systolic blood pressure at the ankle to the systolic blood pressure at the brachial artery; both taken at the same time while you are lying on your back. We do not require that the ankle and brachial pressures be taken on the same side of your body. This is because, as with the ankle pressure, we will use the higher brachial systolic pressure measured. Listing 4.12A is met when your resting ankle/brachial systolic blood pressure ratio is less than 0.50. If your resting ankle/brachial systolic blood pressure ratio is 0.50 or above, we will use 4.12B to evaluate the severity of your PAD, unless you also have a disease causing abnormal arterial calcification or small vessel disease, such as diabetes mellitus. See 4.00G7c and 4.00G8.
c. We will use resting toe systolic blood pressures or resting toe/brachial systolic blood pressure ratios (determined the same way as ankle/brachial ratios, see 4.00G7b) when you have intermittent claudication and a disease that results in abnormal arterial calcification (for example, Monckeberg's sclerosis or diabetes mellitus) or small vessel disease (for example, diabetes mellitus). These diseases may result in misleadingly high blood pressure readings at the ankle. However, high blood pressures due to vascular changes related to these diseases seldom occur at the toe level. While the criteria in 4.12C and 4.12D are intended primarily for individuals who have a disease causing abnormal arterial calcification or small vessel disease, we may also use them for evaluating anyone with PAD.
8. How are toe pressures measured? Toe pressures are measured routinely in most vascular laboratories through one of three methods: most frequently, photoplethysmography; less frequently, plethysmography using strain gauge cuffs; and Doppler ultrasound. Toe pressure can also be measured by using any blood pressure cuff that fits snugly around the big toe and is neither too tight nor too loose. A neonatal cuff or a cuff designed for use on fingers or toes can be used in the measurement of toe pressure.
9. How do we use listing 4.12 if you have had a peripheral graft? Peripheral grafting serves the same purpose as coronary grafting; that is, to bypass a narrow or obstructed arterial segment. If intermittent claudication recurs or persists after peripheral grafting, we may purchase Doppler studies to assess the flow of blood through the bypassed vessel and to establish the current severity of the peripheral arterial impairment. However, if you have had peripheral grafting done for your PAD, we will not use the findings from before the surgery to assess the current severity of your impairment, although we will consider the severity and duration of your impairment prior to your surgery in making our determination or decision.
H. Evaluating Other Cardiovascular Impairments
1. How will we evaluate hypertension? Because hypertension (high blood pressure) generally causes disability through its effects on other body systems, we will evaluate it by reference to the specific body system(s) affected (heart, brain, kidneys, or eyes) when we consider its effects under the listings. We will also consider any limitations imposed by your hypertension when we assess your residual functional capacity.
2. How will we evaluate symptomatic congenital heart disease? Congenital heart disease is any abnormality of the heart or the major blood vessels that is present at birth. Because of improved treatment methods, more children with congenital heart disease are living to adulthood. Although some types of congenital heart disease may be corrected by surgery, many individuals with treated congenital heart disease continue to have problems throughout their lives (symptomatic congenital heart disease). If you have congenital heart disease that results in chronic heart failure with evidence of ventricular dysfunction or in recurrent arrhythmias, we will evaluate your impairment under 4.02 or 4.05. Otherwise, we will evaluate your impairment under 4.06.
3. What is cardiomyopathy and how will we evaluate it? Cardiomyopathy is a disease of the heart muscle. The heart loses its ability to pump blood (heart failure), and in some instances, heart rhythm is disturbed, leading to irregular heartbeats (arrhythmias). Usually, the exact cause of the muscle damage is never found (idiopathic cardiomyopathy). There are various types of cardiomyopathy, which fall into two major categories: Ischemic and nonischemic cardiomyopathy. Ischemic cardiomyopathy typically refers to heart muscle damage that results from coronary artery disease, including heart attacks. Nonischemic cardiomyopathy includes several types: Dilated, hypertrophic, and restrictive. We will evaluate cardiomyopathy under 4.02, 4.04, 4.05, or 11.04, depending on its effects on you.
4. How will we evaluate valvular heart disease? We will evaluate valvular heart disease under the listing appropriate for its effect on you. Thus, we may use 4.02, 4.04, 4.05, 4.06, or an appropriate neurological listing in 11.00ff.
5. What do we consider when we evaluate heart transplant recipients?
a. After your heart transplant, we will consider you disabled for 1 year following the surgery because there is a greater likelihood of rejection of the organ and infection during the first year.
b. However, heart transplant patients generally meet our definition of disability before they undergo transplantation. We will determine the onset of your disability based on the facts in your case.
c. We will not assume that you became disabled when your name was placed on a transplant waiting list. This is because you may be placed on a waiting list soon after diagnosis of the cardiac disorder that may eventually require a transplant. Physicians recognize that candidates for transplantation often have to wait months or even years before a suitable donor heart is found, so they place their patients on the list as soon as permitted.
d. When we do a continuing disability review to determine whether you are still disabled, we will evaluate your residual impairment(s), as shown by symptoms, signs, and laboratory findings, including any side effects of medication. We will consider any remaining symptoms, signs, and laboratory findings indicative of cardiac dysfunction in deciding whether medical improvement (as defined in §§ 404.1594 and 416.994) has occurred.
6. When does an aneurysm have “dissection not controlled by prescribed treatment,” as required under 4.10? An aneurysm (or bulge in the aorta or one of its major branches) is dissecting when the inner lining of the artery begins to separate from the arterial wall. We consider the dissection not controlled when you have persistence of chest pain due to progression of the dissection, an increase in the size of the aneurysm, or compression of one or more branches of the aorta supplying the heart, kidneys, brain, or other organs. An aneurysm with dissection can cause heart failure, renal (kidney) failure, or neurological complications. If you have an aneurysm that does not meet the requirements of 4.10 and you have one or more of these associated conditions, we will evaluate the condition(s) using the appropriate listing.
7. What is hyperlipidemia and how will we evaluate it? Hyperlipidemia is the general term for an elevation of any or all of the lipids (fats or cholesterol) in the blood; for example, hypertriglyceridemia, hypercholesterolemia, and hyperlipoproteinemia. These disorders of lipoprotein metabolism and transport can cause defects throughout the body. The effects most likely to interfere with function are those produced by atherosclerosis (narrowing of the arteries) and coronary artery disease. We will evaluate your lipoprotein disorder by considering its effects on you.
8. What is Marfan syndrome and how will we evaluate it?
a. Marfan syndrome is a genetic connective tissue disorder that affects multiple body systems, including the skeleton, eyes, heart, blood vessels, nervous system, skin, and lungs. There is no specific laboratory test to diagnose Marfan syndrome. The diagnosis is generally made by medical history, including family history, physical examination, including an evaluation of the ratio of arm/leg size to trunk size, a slit lamp eye examination, and a heart test(s), such as an echocardiogram. In some cases, a genetic analysis may be useful, but such analyses may not provide any additional helpful information.
b. The effects of Marfan syndrome can range from mild to severe. In most cases, the disorder progresses as you age. Most individuals with Marfan syndrome have abnormalities associated with the heart and blood vessels. Your heart's mitral valve may leak, causing a heart murmur. Small leaks may not cause symptoms, but larger ones may cause shortness of breath, fatigue, and palpitations. Another effect is that the wall of the aorta may be weakened and abnormally stretch (aortic dilation). This aortic dilation may tear, dissect, or rupture, causing serious heart problems or sometimes sudden death. We will evaluate the manifestations of your Marfan syndrome under the appropriate body system criteria, such as 4.10, or if necessary, consider the functional limitations imposed by your impairment.
I. Other Evaluation Issues
1. What effect does obesity have on the cardiovascular system and how will we evaluate it? Obesity is a medically determinable impairment that is often associated with disorders of the cardiovascular system. Disturbance of this system can be a major cause of disability if you have obesity. Obesity may affect the cardiovascular system because of the increased workload the additional body mass places on the heart. Obesity may make it harder for the chest and lungs to expand. This can mean that the respiratory system must work harder to provide needed oxygen. This in turn would make the heart work harder to pump blood to carry oxygen to the body. Because the body would be working harder at rest, its ability to perform additional work would be less than would otherwise be expected. Thus, the combined effects of obesity with cardiovascular impairments can be greater than the effects of each of the impairments considered separately. We must consider any additional and cumulative effects of obesity when we determine whether you have a severe cardiovascular impairment or a listing-level cardiovascular impairment (or a combination of impairments that medically equals the severity of a listed impairment), and when we assess your residual functional capacity.
2. How do we relate treatment to functional status? In general, conclusions about the severity of a cardiovascular impairment cannot be made on the basis of type of treatment rendered or anticipated. The amount of function restored and the time required for improvement after treatment (medical, surgical, or a prescribed program of progressive physical activity) vary with the nature and extent of the disorder, the type of treatment, and other factors. Depending upon the timing of this treatment in relation to the alleged onset date of disability, we may need to defer evaluation of the impairment for a period of up to 3 months from the date treatment began to permit consideration of treatment effects, unless we can make a determination or decision using the evidence we have. See 4.00B4.
3. How do we evaluate impairments that do not meet one of the cardiovascular listings?
a. These listings are only examples of common cardiovascular impairments that we consider severe enough to prevent you from doing any gainful activity. If your severe impairment(s) does not meet the criteria of any of these listings, we must also consider whether you have an impairment(s) that satisfies the criteria of a listing in another body system.
b. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairments(s) medically equals a listing. (See §§ 404.1526 and 416.926.) If you have a severe impairment(s) that does not meet or medically equal the criteria of a listing, you may or may not have the residual functional capacity to engage in substantial gainful activity. Therefore, we proceed to the fourth and, if necessary, the fifth steps of the sequential evaluation process in §§ 404.1520 and 416.920. If you are an adult, we use the rules in §§ 404.1594 or 416.994, as appropriate, when we decide whether you continue to be disabled.
4.01 Category of Impairments, Cardiovascular System
4.02 Chronic heart failure while on a regimen of prescribed treatment, with symptoms and signs described in 4.00D2. The required level of severity for this impairment is met when the requirements in both A and B are satisfied.
A. Medically documented presence of one of the following:
1. Systolic failure (see 4.00D1a(i)), with left ventricular end diastolic dimensions greater than 6.0 cm or ejection fraction of 30 percent or less during a period of stability (not during an episode of acute heart failure); or
2. Diastolic failure (see 4.00D1a(ii)), with left ventricular posterior wall plus septal thickness totaling 2.5 cm or greater on imaging, with an enlarged left atrium greater than or equal to 4.5 cm, with normal or elevated ejection fraction during a period of stability (not during an episode of acute heart failure);
AND
B. Resulting in one of the following:
1. Persistent symptoms of heart failure which very seriously limit the ability to independently initiate, sustain, or complete activities of daily living in an individual for whom an MC, preferably one experienced in the care of patients with cardiovascular disease, has concluded that the performance of an exercise test would present a significant risk to the individual; or
2. Three or more separate episodes of acute congestive heart failure within a consecutive 12-month period (see 4.00A3e), with evidence of fluid retention (see 4.00D2b(ii)) from clinical and imaging assessments at the time of the episodes, requiring acute extended physician intervention such as hospitalization or emergency room treatment for 12 hours or more, separated by periods of stabilization (see 4.00D4c); or
3. Inability to perform on an exercise tolerance test at a workload equivalent to 5 METs or less due to:
a. Dyspnea, fatigue, palpitations, or chest discomfort; or
b. Three or more consecutive premature ventricular contractions (ventricular tachycardia), or increasing frequency of ventricular ectopy with at least 6 premature ventricular contractions per minute; or
c. Decrease of 10 mm Hg or more in systolic pressure below the baseline systolic blood pressure or the preceding systolic pressure measured during exercise (see 4.00D4d) due to left ventricular dysfunction, despite an increase in workload; or
d. Signs attributable to inadequate cerebral perfusion, such as ataxic gait or mental confusion.
4.04 Ischemic heart disease, with symptoms due to myocardial ischemia, as described in 4.00E3-4.00E7, while on a regimen of prescribed treatment (see 4.00B3 if there is no regimen of prescribed treatment), with one of the following:
A. Sign-or symptom-limited exercise tolerance test demonstrating at least one of the following manifestations at a workload equivalent to 5 METs or less:
1. Horizontal or downsloping depression, in the absence of digitalis glycoside treatment or hypokalemia, of the ST segment of at least −0.10 millivolts (−1.0 mm) in at least 3 consecutive complexes that are on a level baseline in any lead other than aVR, and depression of at least −0.10 millivolts lasting for at least 1 minute of recovery; or
2. At least 0.1 millivolt (1 mm) ST elevation above resting baseline in non-infarct leads during both exercise and 1 or more minutes of recovery; or
3. Decrease of 10 mm Hg or more in systolic pressure below the baseline blood pressure or the preceding systolic pressure measured during exercise (see 4.00E9e) due to left ventricular dysfunction, despite an increase in workload; or
4. Documented ischemia at an exercise level equivalent to 5 METs or less on appropriate medically acceptable imaging, such as radionuclide perfusion scans or stress echocardiography.
OR
B. Three separate ischemic episodes, each requiring revascularization or not amenable to revascularization (see 4.00E9f), within a consecutive 12-month period (see 4.00A3e).
OR
C. Coronary artery disease, demonstrated by angiography (obtained independent of Social Security disability evaluation) or other appropriate medically acceptable imaging, and in the absence of a timely exercise tolerance test or a timely normal drug-induced stress test, an MC, preferably one experienced in the care of patients with cardiovascular disease, has concluded that performance of exercise tolerance testing would present a significant risk to the individual, with both 1 and 2:
1. Angiographic evidence showing:
a. 50 percent or more narrowing of a nonbypassed left main coronary artery; or
b. 70 percent or more narrowing of another nonbypassed coronary artery; or
c. 50 percent or more narrowing involving a long (greater than 1 cm) segment of a nonbypassed coronary artery; or
d. 50 percent or more narrowing of at least two nonbypassed coronary arteries; or
e. 70 percent or more narrowing of a bypass graft vessel; and
2. Resulting in very serious limitations in the ability to independently initiate, sustain, or complete activities of daily living.
4.05 Recurrent arrhythmias, not related to reversible causes, such as electrolyte abnormalities or digitalis glycoside or antiarrhythmic drug toxicity, resulting in uncontrolled (see 4.00A3f), recurrent (see 4.00A3c) episodes of cardiac syncope or near syncope (see 4.00F3b), despite prescribed treatment (see 4.00B3 if there is no prescribed treatment), and documented by resting or ambulatory (Holter) electrocardiography, or by other appropriate medically acceptable testing, coincident with the occurrence of syncope or near syncope (see 4.00F3c).
4.06 Symptomatic congenital heart disease (cyanotic or acyanotic), documented by appropriate medically acceptable imaging (see 4.00A3d) or cardiac catheterization, with one of the following:
A. Cyanosis at rest, and:
1. Hematocrit of 55 percent or greater; or
2. Arterial O2 saturation of less than 90 percent in room air, or resting arterial PO2 of 60 Torr or less.
OR
B. Intermittent right-to-left shunting resulting in cyanosis on exertion (e.g., Eisenmenger's physiology) and with arterial PO2 of 60 Torr or less at a workload equivalent to 5 METs or less.
OR
C. Secondary pulmonary vascular obstructive disease with pulmonary arterial systolic pressure elevated to at least 70 percent of the systemic arterial systolic pressure.
4.09 Heart transplant. Consider under a disability for 1 year following surgery; thereafter, evaluate residual impairment under the appropriate listing.
4.10 Aneurysm of aorta or major branches, due to any cause (e.g., atherosclerosis, cystic medial necrosis, Marfan syndrome, trauma), demonstrated by appropriate medically acceptable imaging, with dissection not controlled by prescribed treatment (see 4.00H6).
4.11 Chronic venous insufficiency of a lower extremity with incompetency or obstruction of the deep venous system and one of the following:
A. Extensive brawny edema (see 4.00G3) involving at least two-thirds of the leg between the ankle and knee or the distal one-third of the lower extremity between the ankle and hip.
OR
B. Superficial varicosities, stasis dermatitis, and either recurrent ulceration or persistent ulceration that has not healed following at least 3 months of prescribed treatment.
4.12 Peripheral arterial disease, as determined by appropriate medically acceptable imaging (see 4.00A3d, 4.00G2, 4.00G5, and 4.00G6), causing intermittent claudication (see 4.00G1) and one of the following:
A. Resting ankle/brachial systolic blood pressure ratio of less than 0.50.
OR
B. Decrease in systolic blood pressure at the ankle on exercise (see 4.00G7a and 4.00C16-4.00C17) of 50 percent or more of pre-exercise level and requiring 10 minutes or more to return to pre-exercise level.
OR
C. Resting toe systolic pressure of less than 30 mm Hg (see 4.00G7c and 4.00G8).
OR
D. Resting toe/brachial systolic blood pressure ratio of less than 0.40 (see 4.00G7c).
5.00 Digestive System
A. What kinds of disorders do we consider in the digestive system? Disorders of the digestive system include gastrointestinal hemorrhage, hepatic (liver) dysfunction, inflammatory bowel disease, short bowel syndrome, and malnutrition. They may also lead to complications, such as obstruction, or be accompanied by manifestations in other body systems.
B. What documentation do we need? We need a record of your medical evidence, including clinical and laboratory findings. The documentation should include appropriate medically acceptable imaging studies and reports of endoscopy, operations, and pathology, as appropriate to each listing, to document the severity and duration of your digestive disorder. Medically acceptable imaging includes, but is not limited to, x-ray imaging, sonography, computerized axial tomography (CAT scan), magnetic resonance imaging (MRI), and radionuclide scans. Appropriate means that the technique used is the proper one to support the evaluation and diagnosis of the disorder. The findings required by these listings must occur within the period we are considering in connection with your application or continuing disability review.
C. How do we consider the effects of treatment?
1. Digestive disorders frequently respond to medical or surgical treatment; therefore, we generally consider the severity and duration of these disorders within the context of prescribed treatment.
2. We assess the effects of treatment, including medication, therapy, surgery, or any other form of treatment you receive, by determining if there are improvements in the symptoms, signs, and laboratory findings of your digestive disorder. We also assess any side effects of your treatment that may further limit your functioning.
3. To assess the effects of your treatment, we may need information about:
a. The treatment you have been prescribed (for example, the type of medication or therapy, or your use of parenteral (intravenous) nutrition or supplemental enteral nutrition via a gastrostomy);
b. The dosage, method, and frequency of administration;
c. Your response to the treatment;
d. Any adverse effects of such treatment; and
e. The expected duration of the treatment.
4. Because the effects of treatment may be temporary or long-term, in most cases we need information about the impact of your treatment, including its expected duration and side effects, over a sufficient period of time to help us assess its outcome. When adverse effects of treatment contribute to the severity of your impairment(s), we will consider the duration or expected duration of the treatment when we assess the duration of your impairment(s).
5. If you need parenteral (intravenous) nutrition or supplemental enteral nutrition via a gastrostomy to avoid debilitating complications of a digestive disorder, this treatment will not, in itself, indicate that you are unable to do any gainful activity, except under 5.07, short bowel syndrome (see 5.00F).
6. If you have not received ongoing treatment or have not had an ongoing relationship with the medical community despite the existence of a severe impairment(s), we will evaluate the severity and duration of your digestive impairment on the basis of the current medical and other evidence in your case record. If you have not received treatment, you may not be able to show an impairment that meets the criteria of one of the digestive system listings, but your digestive impairment may medically equal a listing or be disabling based on consideration of your residual functional capacity, age, education, and work experience.
D. How do we evaluate chronic liver disease?
1. General. Chronic liver disease is characterized by liver cell necrosis, inflammation, or scarring (fibrosis or cirrhosis), due to any cause, that persists for more than 6 months. Chronic liver disease may result in portal hypertension, cholestasis (suppression of bile flow), extrahepatic manifestations, or liver cancer. (We evaluate liver cancer under 13.19.) Significant loss of liver function may be manifested by hemorrhage from varices or portal hypertensive gastropathy, ascites (accumulation of fluid in the abdominal cavity), hydrothorax (ascitic fluid in the chest cavity), or encephalopathy. There can also be progressive deterioration of laboratory findings that are indicative of liver dysfunction. Liver transplantation is the only definitive cure for end stage liver disease (ESLD).
2. Examples of chronic liver disease include, but are not limited to, chronic hepatitis, alcoholic liver disease, non-alcoholic steatohepatitis (NASH), primary biliary cirrhosis (PBC), primary sclerosing cholangitis (PSC), autoimmune hepatitis, hemochromatosis, drug-induced liver disease, Wilson's disease, and serum alpha-1 antitrypsin deficiency. Acute hepatic injury is frequently reversible, as in viral, drug-induced, toxin-induced, alcoholic, and ischemic hepatitis. In the absence of evidence of a chronic impairment, episodes of acute liver disease do not meet 5.05.
3. Manifestations of chronic liver disease.
a. Symptoms may include, but are not limited to, pruritis (itching), fatigue, nausea, loss of appetite, or sleep disturbances. Symptoms of chronic liver disease may have a poor correlation with the severity of liver disease and functional ability.
b. Signs may include, but are not limited to, jaundice, enlargement of the liver and spleen, ascites, peripheral edema, and altered mental status.
c. Laboratory findings may include, but are not limited to, increased liver enzymes, increased serum total bilirubin, increased ammonia levels, decreased serum albumin, and abnormal coagulation studies, such as increased International Normalized Ratio (INR) or decreased platelet counts. Abnormally low serum albumin or elevated INR levels indicate loss of synthetic liver function, with increased likelihood of cirrhosis and associated complications. However, other abnormal lab tests, such as liver enzymes, serum total bilirubin, or ammonia levels, may have a poor correlation with the severity of liver disease and functional ability. A liver biopsy may demonstrate the degree of liver cell necrosis, inflammation, fibrosis, and cirrhosis. If you have had a liver biopsy, we will make every reasonable effort to obtain the results; however, we will not purchase a liver biopsy. Imaging studies (CAT scan, ultrasound, MRI) may show the size and consistency (fatty liver, scarring) of the liver and document ascites (see 5.00D6).
4. Chronic viral hepatitis infections.
a. General.
(i) Chronic viral hepatitis infections are commonly caused by hepatitis C virus (HCV), and to a lesser extent, hepatitis B virus (HBV). Usually, these are slowly progressive disorders that persist over many years during which the symptoms and signs are typically nonspecific, intermittent, and mild (for example, fatigue, difficulty with concentration, or right upper quadrant pain). Laboratory findings (liver enzymes, imaging studies, liver biopsy pathology) and complications are generally similar in HCV and HBV. The spectrum of these chronic viral hepatitis infections ranges widely and includes an asymptomatic state; insidious disease with mild to moderate symptoms associated with fluctuating liver tests; extrahepatic manifestations; cirrhosis, both compensated and decompensated; ESLD with the need for liver transplantation; and liver cancer. Treatment for chronic viral hepatitis infections varies considerably based on medication tolerance, treatment response, adverse effects of treatment, and duration of the treatment. Comorbid disorders, such as HIV infection, may accelerate the clinical course of viral hepatitis infection(s) or may result in a poorer response to medical treatment.
(ii) We evaluate all types of chronic viral hepatitis infections under 5.05 or any listing in an affected body system(s). If your impairment(s) does not meet or medically equal a listing, we will consider the effects of your hepatitis when we assess your residual functional capacity.
b. Chronic hepatitis B virus (HBV) infection.
(i) Chronic HBV infection can be diagnosed by the detection of hepatitis B surface antigen (HBsAg) or hepatitis B virus DNA (HBV DNA) in the blood for at least 6 months. In addition, detection of the hepatitis B e antigen (HBeAg) suggests an increased likelihood of progression to cirrhosis, ESLD, and hepatocellular carcinoma. (HBeAg may also be referred to as “hepatitis B early antigen” or “hepatitis B envelope antigen.”)
(ii) The therapeutic goal of treatment is to suppress HBV replication and thereby prevent progression to cirrhosis, ESLD, and hepatocellular carcinoma. Treatment usually includes interferon injections, oral antiviral agents, or a combination of both. Common adverse effects of treatment are the same as noted in 5.00D4c(ii) for HCV, and generally end within a few days after treatment is discontinued.
c. Chronic hepatitis C virus (HCV) infection.
(i) Chronic HCV infection is diagnosed by the detection of hepatitis C viral RNA in the blood for at least 6 months. Documentation of the therapeutic response to treatment is also monitored by the quantitative assay of serum HCV RNA (“HCV viral load”). Treatment usually includes a combination of interferon injections and oral ribavirin; whether a therapeutic response has occurred is usually assessed after 12 weeks of treatment by checking the HCV viral load. If there has been a substantial reduction in HCV viral load (also known as early viral response, or EVR), this reduction is predictive of a sustained viral response with completion of treatment. Combined therapy is commonly discontinued after 12 weeks when there is no early viral response, since in that circumstance there is little chance of obtaining a sustained viral response (SVR). Otherwise, treatment is usually continued for a total of 48 weeks.
(ii) Combined interferon and ribavirin treatment may have significant adverse effects that may require dosing reduction, planned interruption of treatment, or discontinuation of treatment. Adverse effects may include: Anemia (ribavirin-induced hemolysis), neutropenia, thrombocytopenia, fever, cough, fatigue, myalgia, arthralgia, nausea, loss of appetite, pruritis, and insomnia. Behavioral side effects may also occur. Influenza-like symptoms are generally worse in the first 4 to 6 hours after each interferon injection and during the first weeks of treatment. Adverse effects generally end within a few days after treatment is discontinued.
d. Extrahepatic manifestations of HBV and HCV. In addition to their hepatic manifestations, both HBV and HCV may have significant extrahepatic manifestations in a variety of body systems. These include, but are not limited to: Keratoconjunctivitis (sicca syndrome), glomerulonephritis, skin disorders (for example, lichen planus, porphyria cutanea tarda), neuropathy, and immune dysfunction (for example, cryoglobulinemia, Sjögren's syndrome, and vasculitis). The extrahepatic manifestations of HBV and HCV may not correlate with the severity of your hepatic impairment. If your impairment(s) does not meet or medically equal a listing in an affected body system(s), we will consider the effects of your extrahepatic manifestations when we assess your residual functional capacity.
5. Gastrointestinal hemorrhage (5.02 and 5.05A). Gastrointestinal hemorrhaging can result in hematemesis (vomiting of blood), melena (tarry stools), or hematochezia (bloody stools). Under 5.02, the required transfusions of at least 2 units of blood must be at least 30 days apart and occur at least three times during a consecutive 6-month period. Under 5.05A, hemodynamic instability is diagnosed with signs such as pallor (pale skin), diaphoresis (profuse perspiration), rapid pulse, low blood pressure, postural hypotension (pronounced fall in blood pressure when arising to an upright position from lying down) or syncope (fainting). Hemorrhaging that results in hemodynamic instability is potentially life-threatening and therefore requires hospitalization for transfusion and supportive care. Under 5.05A, we require only one hospitalization for transfusion of at least 2 units of blood.
6. Ascites or hydrothorax (5.05B) indicates significant loss of liver function due to chronic liver disease. We evaluate ascites or hydrothorax that is not attributable to other causes under 5.05B. The required findings must be present on at least two evaluations at least 60 days apart within a consecutive 6-month period and despite continuing treatment as prescribed.
7. Spontaneous bacterial peritonitis (5.05C) is an infectious complication of chronic liver disease. It is diagnosed by ascitic peritoneal fluid that is documented to contain an absolute neutrophil count of at least 250 cells/mm3. The required finding in 5.05C is satisfied with one evaluation documenting peritoneal fluid infection. We do not evaluate other causes of peritonitis that are unrelated to chronic liver disease, such as tuberculosis, malignancy, and perforated bowel, under this listing. We evaluate these other causes of peritonitis under the appropriate body system listings.
8. Hepatorenal syndrome (5.05D) is defined as functional renal failure associated with chronic liver disease in the absence of underlying kidney pathology. Hepatorenal syndrome is documented by elevation of serum creatinine, marked sodium retention, and oliguria (reduced urine output). The requirements of 5.05D are satisfied with documentation of any one of the three laboratory findings on one evaluation. We do not evaluate known causes of renal dysfunction, such as glomerulonephritis, tubular necrosis, drug-induced renal disease, and renal infections, under this listing. We evaluate these other renal impairments under 6.00ff.
9. Hepatopulmonary syndrome (5.05E) is defined as arterial deoxygenation (hypoxemia) that is associated with chronic liver disease due to intrapulmonary arteriovenous shunting and vasodilatation in the absence of other causes of arterial deoxygenation. Clinical manifestations usually include dyspnea, orthodeoxia (increasing hypoxemia with erect position), platypnea (improvement of dyspnea with flat position), cyanosis, and clubbing. The requirements of 5.05E are satisfied with documentation of any one of the findings on one evaluation. In 5.05E1, we require documentation of the altitude of the testing facility because altitude affects the measurement of arterial oxygenation. We will not purchase the specialized studies described in 5.05E2; however, if you have had these studies at a time relevant to your claim, we will make every reasonable effort to obtain the reports for the purpose of establishing whether your impairment meets 5.05E2.
10. Hepatic encephalopathy (5.05F).
a. General. Hepatic encephalopathy usually indicates severe loss of hepatocellular function. We define hepatic encephalopathy under 5.05F as a recurrent or chronic neuropsychiatric disorder, characterized by abnormal behavior, cognitive dysfunction, altered state of consciousness, and ultimately coma and death. The diagnosis is established by changes in mental status associated with fleeting neurological signs, including “flapping tremor” (asterixis), characteristic electroencephalographic (EEG) abnormalities, or abnormal laboratory values that indicate loss of synthetic liver function. We will not purchase the EEG testing described in 5.05F3b; however, if you have had this test at a time relevant to your claim, we will make every reasonable effort to obtain the report for the purpose of establishing whether your impairment meets 5.05F.
b. Acute encephalopathy. We will not evaluate your acute encephalopathy under 5.05F if it results from conditions other than chronic liver disease, such as vascular events and neoplastic diseases. We will evaluate these other causes of acute encephalopathy under the appropriate body system listings.
11. End stage liver disease (ESLD) documented by scores from the SSA Chronic Liver Disease (SSA CLD) calculation (5.05G).
a. We will use the SSA CLD score to evaluate your ESLD under 5.05G. We explain how we calculate the SSA CLD score in b. through g. of this section.
b. To calculate the SSA CLD score, we use a formula that includes three laboratory values: Serum total bilirubin (mg/dL), serum creatinine (mg/dL), and International Normalized Ratio (INR). The formula for the SSA CLD score calculation is:
9.57 × [Loge(serum creatinine mg/dL)]
+ 3.78 × [Loge(serum total bilirubin mg/dL)]
+ 11.2 × [Loge(INR)]
+ 6.43
c. When we indicate “Loge” in the formula for the SSA CLD score calculation, we mean the “base e logarithm” or “natural logarithm” (ln) of a numerical laboratory value, not the “base 10 logarithm” or “common logarithm” (log) of the laboratory value, and not the actual laboratory value. For example, if an individual has laboratory values of serum creatinine 1.2 mg/dL, serum total bilirubin 2.2 mg/dL, and INR 1.0, we would compute the SSA CLD score as follows:
9.57 × [Loge(serum creatinine 1.2 mg/dL) = 0.182]
+ 3.78 × [Loge(serum total bilirubin 2.2 mg/dL) = 0.788]
+ 11.2 × [Loge(INR 1.0) = 0]
+ 6.43
___
= 1.74 + 2.98 + 0 + 6.43
= 11.15, which is then rounded to an SSA CLD score of 11.
d. For any SSA CLD score calculation, all of the required laboratory values must have been obtained within 30 days of each other. If there are multiple laboratory values within the 30-day interval for any given laboratory test (serum total bilirubin, serum creatinine, or INR), we will use the highest value for the SSA CLD score calculation. We will round all laboratory values less than 1.0 up to 1.0.
e. Listing 5.05G requires two SSA CLD scores. The laboratory values for the second SSA CLD score calculation must have been obtained at least 60 days after the latest laboratory value for the first SSA CLD score and within the required 6-month period. We will consider the date of each SSA CLD score to be the date of the first laboratory value used for its calculation.
f. If you are in renal failure or on dialysis within a week of any serum creatinine test in the period used for the SSA CLD calculation, we will use a serum creatinine of 4, which is the maximum serum creatinine level allowed in the calculation, to calculate your SSA CLD score.
g. If you have the two SSA CLD scores required by 5.05G, we will find that your impairment meets the criteria of the listing from at least the date of the first SSA CLD score.
12. Liver transplantation (5.09) may be performed for metabolic liver disease, progressive liver failure, life-threatening complications of liver disease, hepatic malignancy, and acute fulminant hepatitis (viral, drug-induced, or toxin-induced). We will consider you to be disabled for 1 year from the date of the transplantation. Thereafter, we will evaluate your residual impairment(s) by considering the adequacy of post-transplant liver function, the requirement for post-transplant antiviral therapy, the frequency and severity of rejection episodes, comorbid complications, and all adverse treatment effects.
E. How do we evaluate inflammatory bowel disease (IBD)?
1. Inflammatory bowel disease (5.06) includes, but is not limited to, Crohn's disease and ulcerative colitis. These disorders, while distinct entities, share many clinical, laboratory, and imaging findings, as well as similar treatment regimens. Remissions and exacerbations of variable duration are the hallmark of IBD. Crohn's disease may involve the entire alimentary tract from the mouth to the anus in a segmental, asymmetric fashion. Obstruction, stenosis, fistulization, perineal involvement, and extraintestinal manifestations are common. Crohn's disease is rarely curable and recurrence may be a lifelong problem, even after surgical resection. In contrast, ulcerative colitis only affects the colon. The inflammatory process may be limited to the rectum, extend proximally to include any contiguous segment, or involve the entire colon. Ulcerative colitis may be cured by total colectomy.
2. Symptoms and signs of IBD include diarrhea, fecal incontinence, rectal bleeding, abdominal pain, fatigue, fever, nausea, vomiting, arthralgia, abdominal tenderness, palpable abdominal mass (usually inflamed loops of bowel) and perineal disease. You may also have signs or laboratory findings indicating malnutrition, such as weight loss, edema, anemia, hypoalbuminemia, hypokalemia, hypocalcemia, or hypomagnesemia.
3. IBD may be associated with significant extraintestinal manifestations in a variety of body systems. These include, but are not limited to, involvement of the eye (for example, uveitis, episcleritis, iritis); hepatobiliary disease (for example, gallstones, primary sclerosing cholangitis); urologic disease (for example, kidney stones, obstructive hydronephrosis); skin involvement (for example, erythema nodosum, pyoderma gangrenosum); or non-destructive inflammatory arthritis. You may also have associated thromboembolic disorders or vascular disease. These manifestations may not correlate with the severity of your IBD. If your impairment does not meet any of the criteria of 5.06, we will consider the effects of your extraintestinal manifestations in determining whether you have an impairment(s) that meets or medically equals another listing, and we will also consider the effects of your extraintestinal manifestations when we assess your residual functional capacity.
4. Surgical diversion of the intestinal tract, including ileostomy and colostomy, does not preclude any gainful activity if you are able to maintain adequate nutrition and function of the stoma. However, if you are not able to maintain adequate nutrition, we will evaluate your impairment under 5.08.
F. How do we evaluate short bowel syndrome (SBS)?
1. Short bowel syndrome (5.07) is a disorder that occurs when ischemic vascular insults (for example, volvulus), trauma, or IBD complications require surgical resection of more than one-half of the small intestine, resulting in the loss of intestinal absorptive surface and a state of chronic malnutrition. The management of SBS requires long-term parenteral nutrition via an indwelling central venous catheter (central line); the process is often referred to as hyperalimentation or total parenteral nutrition (TPN). Individuals with SBS can also feed orally, with variable amounts of nutrients being absorbed through their remaining intestine. Over time, some of these individuals can develop additional intestinal absorptive surface, and may ultimately be able to be weaned off their parenteral nutrition.
2. Your impairment will continue to meet 5.07 as long as you remain dependent on daily parenteral nutrition via a central venous catheter for most of your nutritional requirements. Long-term complications of SBS and parenteral nutrition include central line infections (with or without septicemia), thrombosis, hepatotoxicity, gallstones, and loss of venous access sites. Intestinal transplantation is the only definitive treatment for individuals with SBS who remain chronically dependent on parenteral nutrition.
3. To document SBS, we need a copy of the operative report of intestinal resection, the summary of the hospitalization(s) including: Details of the surgical findings, medically appropriate postoperative imaging studies that reflect the amount of your residual small intestine, or if we cannot get one of these reports, other medical reports that include details of the surgical findings. We also need medical documentation that you are dependent on daily parenteral nutrition to provide most of your nutritional requirements.
G. How do we evaluate weight loss due to any digestive disorder?
1. In addition to the impairments specifically mentioned in these listings, other digestive disorders, such as esophageal stricture, pancreatic insufficiency, and malabsorption, may result in significant weight loss. We evaluate weight loss due to any digestive disorder under 5.08 by using the Body Mass Index (BMI). We also provide a criterion in 5.06B for lesser weight loss resulting from IBD.
2. BMI is the ratio of your weight to the square of your height. Calculation and interpretation of the BMI are independent of gender in adults.
a. We calculate BMI using inches and pounds, meters and kilograms, or centimeters and kilograms. We must have measurements of your weight and height without shoes for these calculations.
b. We calculate BMI using one of the following formulas:



H. What do we mean by the phrase “consider under a disability for 1 year”? We use the phrase “consider under a disability for 1 year” following a specific event in 5.02, 5.05A, and 5.09 to explain how long your impairment can meet the requirements of those particular listings. This phrase does not refer to the date on which your disability began, only to the date on which we must reevaluate whether your impairment continues to meet a listing or is otherwise disabling. For example, if you have received a liver transplant, you may have become disabled before the transplant because of chronic liver disease. Therefore, we do not restrict our determination of the onset of disability to the date of the specified event. We will establish an onset date earlier than the date of the specified event if the evidence in your case record supports such a finding.
I. How do we evaluate impairments that do not meet one of the digestive disorder listings?
1. These listings are only examples of common digestive disorders that we consider severe enough to prevent you from doing any gainful activity. If your impairment(s) does not meet the criteria of any of these listings, we must also consider whether you have an impairment(s) that satisfies the criteria of a listing in another body system. For example, if you have hepatitis B or C and you are depressed, we will evaluate your impairment under 12.04.
2. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. (See §§ 404.1526 and 416.926.) If your impairment(s) does not meet or medically equal a listing, you may or may not have the residual functional capacity to engage in substantial gainful activity. In this situation, we will proceed to the fourth, and if necessary, the fifth steps of the sequential evaluation process in §§ 404.1520 and 416.920. When we decide whether you continue to be disabled, we use the rules in §§ 404.1594, 416.994, and 416.994a as appropriate.
5.01 Category of Impairments, Digestive System
5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood per transfusion, and occurring at least three times during a consecutive 6-month period. The transfusions must be at least 30 days apart within the 6-month period. Consider under a disability for 1 year following the last documented transfusion; thereafter, evaluate the residual impairment(s).
5.03-5.04 [Reserved]
5.05 Chronic liver disease, with:
A. Hemorrhaging from esophageal, gastric, or ectopic varices or from portal hypertensive gastropathy, demonstrated by endoscopy, x-ray, or other appropriate medically acceptable imaging, resulting in hemodynamic instability as defined in 5.00D5, and requiring hospitalization for transfusion of at least 2 units of blood. Consider under a disability for 1 year following the last documented transfusion; thereafter, evaluate the residual impairment(s).
OR
B. Ascites or hydrothorax not attributable to other causes, despite continuing treatment as prescribed, present on at least two evaluations at least 60 days apart within a consecutive 6-month period. Each evaluation must be documented by:
1. Paracentesis or thoracentesis; or
2. Appropriate medically acceptable imaging or physical examination and one of the following:
a. Serum albumin of 3.0 g/dL or less; or
b. International Normalized Ratio (INR) of at least 1.5.
OR
C. Spontaneous bacterial peritonitis with peritoneal fluid containing an absolute neutrophil count of at least 250 cells/mm3.
OR
D. Hepatorenal syndrome as described in 5.00D8, with one of the following:
1. Serum creatinine elevation of at least 2 mg/dL; or
2. Oliguria with 24-hour urine output less than 500 mL; or
3. Sodium retention with urine sodium less than 10 mEq per liter.
OR
E. Hepatopulmonary syndrome as described in 5.00D9, with:
1. Arterial oxygenation (PaO2) on room air of:
a. 60 mm Hg or less, at test sites less than 3000 feet above sea level, or
b. 55 mm Hg or less, at test sites from 3000 to 6000 feet, or
c. 50 mm Hg or less, at test sites above 6000 feet; or
2. Documentation of intrapulmonary arteriovenous shunting by contrast-enhanced echocardiography or macroaggregated albumin lung perfusion scan.
OR
F. Hepatic encephalopathy as described in 5.00D10, with 1 and either 2 or 3:
1. Documentation of abnormal behavior, cognitive dysfunction, changes in mental status, or altered state of consciousness (for example, confusion, delirium, stupor, or coma), present on at least two evaluations at least 60 days apart within a consecutive 6-month period; and
2. History of transjugular intrahepatic portosystemic shunt (TIPS) or any surgical portosystemic shunt: or
3. One of the following occurring on at least two evaluations at least 60 days apart within the same consecutive 6-month period as in F1:
a. Asterixis or other fluctuating physical neurological abnormalities; or
b. Electroencephalogram (EEG) demonstrating triphasic slow wave activity; or
c. Serum albumin of 3.0 g/dL or less; or
d. International Normalized Ratio (INR) of 1.5 or greater.
OR
G. End stage liver disease with SSA CLD scores of 22 or greater calculated as described in 5.00D11. Consider under a disability from at least the date of the first score.
5.06 Inflammatory bowel disease (IBD) documented by endoscopy, biopsy, appropriate medically acceptable imaging, or operative findings with:
A. Obstruction of stenotic areas (not adhesions) in the small intestine or colon with proximal dilatation, confirmed by appropriate medically acceptable imaging or in surgery, requiring hospitalization for intestinal decompression or for surgery, and occurring on at least two occasions at least 60 days apart within a consecutive 6-month period;
OR
B. Two of the following despite continuing treatment as prescribed and occurring within the same consecutive 6-month period:
1. Anemia with hemoglobin of less than 10.0 g/dL, present on at least two evaluations at least 60 days apart; or
2. Serum albumin of 3.0 g/dL or less, present on at least two evaluations at least 60 days apart; or
3. Clinically documented tender abdominal mass palpable on physical examination with abdominal pain or cramping that is not completely controlled by prescribed narcotic medication, present on at least two evaluations at least 60 days apart; or
4. Perineal disease with a draining abscess or fistula, with pain that is not completely controlled by prescribed narcotic medication, present on at least two evaluations at least 60 days apart; or
5. Involuntary weight loss of at least 10 percent from baseline, as computed in pounds, kilograms, or BMI, present on at least two evaluations at least 60 days apart; or
6. Need for supplemental daily enteral nutrition via a gastrostomy or daily parenteral nutrition via a central venous catheter.
5.07 Short bowel syndrome (SBS), due to surgical resection of more than one-half of the small intestine, with dependence on daily parenteral nutrition via a central venous catheter (see 5.00F).
5.08 Weight loss due to any digestive disorder despite continuing treatment as prescribed, with BMI of less than 17.50 calculated on at least two evaluations at least 60 days apart within a consecutive 6-month period.
5.09 Liver transplantation. Consider under a disability for 1 year following the date of transplantation; thereafter, evaluate the residual impairment(s) (see 5.00D12 and 5.00H).
6.00 Genitourinary disorders
A. Which disorders do we evaluate under these listings?
We evaluate genitourinary disorders resulting in chronic kidney disease (CKD). Examples of such disorders include chronic glomerulonephritis, hypertensive nephropathy, diabetic nephropathy, chronic obstructive uropathy, and hereditary nephropathies. We also evaluate nephrotic syndrome due to glomerular dysfunction under these listings.
B. What evidence do we need?
1. We need evidence that documents the signs, symptoms, and laboratory findings of your CKD. This evidence should include reports of clinical examinations, treatment records, and documentation of your response to treatment. Laboratory findings, such as serum creatinine or serum albumin levels, may document your kidney function. We generally need evidence covering a period of at least 90 days unless we can make a fully favorable determination or decision without it.
2. Estimated glomerular filtration rate (eGFR). The eGFR is an estimate of the filtering capacity of the kidneys that takes into account serum creatinine concentration and other variables, such as your age, gender, and body size. If your medical evidence includes eGFR findings, we will consider them when we evaluate your CKD under 6.05.
3. Kidney or bone biopsy. If you have had a kidney or bone biopsy, we need a copy of the pathology report. When we cannot get a copy of the pathology report, we will accept a statement from an acceptable medical source verifying that a biopsy was performed and describing the results.
C. What other factors do we consider when we evaluate your genitourinary disorder?
1. Chronic hemodialysis or peritoneal dialysis.
a. Dialysis is a treatment for CKD that uses artificial means to remove toxic metabolic byproducts from the blood. Hemodialysis uses an artificial kidney machine to clean waste products from the blood; peritoneal dialysis uses a dialyzing solution that is introduced into and removed from the abdomen (peritoneal cavity) either continuously or intermittently. Under 6.03, your ongoing dialysis must have lasted or be expected to last for a continuous period of at least 12 months. To satisfy the requirements in 6.03, we will accept a report from an acceptable medical source that describes your CKD and your current dialysis, and indicates that your dialysis will be ongoing.
b. If you are undergoing chronic hemodialysis or peritoneal dialysis, your CKD may meet our definition of disability before you started dialysis. We will determine the onset of your disability based on the facts in your case record.
2. Kidney transplant.
a. If you receive a kidney transplant, we will consider you to be disabled under 6.04 for 1 year from the date of transplant. After that, we will evaluate your residual impairment(s) by considering your post-transplant function, any rejection episodes you have had, complications in other body systems, and any adverse effects related to ongoing treatment.
b. If you received a kidney transplant, your CKD may meet our definition of disability before you received the transplant. We will determine the onset of your disability based on the facts in your case record.
3. Renal osteodystrophy. This condition is the bone degeneration resulting from chronic kidney disease-mineral and bone disorder (CKD-MBD). CKD-MBD occurs when the kidneys are unable to maintain the necessary levels of minerals, hormones, and vitamins required for bone structure and function. Under 6.05B1, “severe bone pain” means frequent or intractable (resistant to treatment) bone pain that interferes with physical activity or mental functioning.
4. Peripheral neuropathy. This disorder results when the kidneys do not adequately filter toxic substances from the blood. These toxins can adversely affect nerve tissue. The resulting neuropathy may affect peripheral motor or sensory nerves, or both, causing pain, numbness, tingling, and muscle weakness in various parts of the body. Under 6.05B2, the peripheral neuropathy must be a severe impairment. (See §§ 404.1520(c), 404.1521, 416.920(c), and 416.921 of this chapter.) It must also have lasted or be expected to last for a continuous period of at least 12 months.
5. Fluid overload syndrome. This condition occurs when excess sodium and water retention in the body due to CKD results in vascular congestion. Under 6.05B3, we need a description of a physical examination that documents signs and symptoms of vascular congestion, such as congestive heart failure, pleural effusion (excess fluid in the chest), ascites (excess fluid in the abdomen), hypertension, fatigue, shortness of breath, or peripheral edema.
6. Anasarca (generalized massive edema or swelling). Under 6.05B3 and 6.06B, we need a description of the extent of edema, including pretibial (in front of the tibia), periorbital (around the eyes), or presacral (in front of the sacrum) edema. We also need a description of any ascites, pleural effusion, or pericardial effusion.
7. Anorexia (diminished appetite) with weight loss. Anorexia is a frequent sign of CKD and can result in weight loss. We will use body mass index (BMI) to determine the severity of your weight loss under 6.05B4. (BMI is the ratio of your measured weight to the square of your measured height.) The formula for calculating BMI is in section 5.00G.
8. Complications of CKD. The hospitalizations in 6.09 may be for different complications of CKD. Examples of complications from CKD that may result in hospitalization include stroke, congestive heart failure, hypertensive crisis, or acute kidney failure requiring a short course of hemodialysis. If the CKD complication occurs during a hospitalization that was initially for a co-occurring condition, we will evaluate it under our rules for determining medical equivalence. (See §§ 404.1526 and 416.926 of this chapter.) We will evaluate co-occurring conditions, including those that result in hospitalizations, under the listings for the affected body system or under our rules for medical equivalence.
D. How do we evaluate disorders that do not meet one of the genitourinary listings?
1. The listed disorders are only examples of common genitourinary disorders that we consider severe enough to prevent you from doing any gainful activity. If your impairment(s) does not meet the criteria of any of these listings, we must also consider whether you have an impairment(s) that satisfies the criteria of a listing in another body system.
2. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. (See §§ 404.1526 and 416.926 of this chapter.) Genitourinary disorders may be associated with disorders in other body systems, and we consider the combined effects of multiple impairments when we determine whether they medically equal a listing. If your impairment(s) does not meet or medically equal the criteria of a listing, you may or may not have the residual functional capacity to engage in substantial gainful activity. We proceed to the fourth and, if necessary, the fifth steps of the sequential evaluation process in §§ 404.1520 and 416.920 of this chapter. We use the rules in §§ 404.1594 and 416.994 of this chapter, as appropriate, when we decide whether you continue to be disabled.
6.01 Category of Impairments, Genitourinary Disorders
6.03 Chronic kidney disease, with chronic hemodialysis or peritoneal dialysis (see 6.00C1).
6.04 Chronic kidney disease, with kidney transplant. Consider under a disability for 1 year following the transplant; thereafter, evaluate the residual impairment (see 6.00C2).
6.05 Chronic kidney disease, with impairment of kidney function, with A and B:
A. Reduced glomerular filtration evidenced by one of the following laboratory findings documented on at least two occasions at least 90 days apart during a consecutive 12-month period:
1. Serum creatinine of 4 mg/dL or greater; or
2. Creatinine clearance of 20 ml/min. or less; or
3. Estimated glomerular filtration rate (eGFR) of 20 ml/min/1.73m2 or less.
AND
B. One of the following:
1. Renal osteodystrophy (see 6.00C3) with severe bone pain and imaging studies documenting bone abnormalities, such as osteitis fibrosa, osteomalacia, or pathologic fractures; or
2. Peripheral neuropathy (see 6.00C4); or
3. Fluid overload syndrome (see 6.00C5) documented by one of the following:
a. Diastolic hypertension greater than or equal to diastolic blood pressure of 110 mm Hg despite at least 90 consecutive days of prescribed therapy, documented by at least two measurements of diastolic blood pressure at least 90 days apart during a consecutive 12-month period; or
b. Signs of vascular congestion or anasarca (see 6.00C6) despite at least 90 consecutive days of prescribed therapy, documented on at least two occasions at least 90 days apart during a consecutive 12-month period; or
4. Anorexia with weight loss (see 6.00C7) determined by body mass index (BMI) of 18.0 or less, calculated on at least two occasions at least 90 days apart during a consecutive 12-month period.
6.06 Nephrotic syndrome, with A and B:
A. Laboratory findings as described in 1 or 2, documented on at least two occasions at least 90 days apart during a consecutive 12-month period:
1. Proteinuria of 10.0 g or greater per 24 hours; or
2. Serum albumin of 3.0 g/dL or less, and
a. Proteinuria of 3.5 g or greater per 24 hours; or
b. Urine total-protein-to-creatinine ratio of 3.5 or greater.
AND
B. Anasarca (see 6.00C6) persisting for at least 90 days despite prescribed treatment.
6.09 Complications of chronic kidney disease (see 6.00C8) requiring at least three hospitalizations within a consecutive 12-month period and occurring at least 30 days apart. Each hospitalization must last at least 48 hours, including hours in a hospital emergency department immediately before the hospitalization.
7.00 Hematological Disorders
A. What hematological disorders do we evaluate under these listings?
1. We evaluate non-malignant (non-cancerous) hematological disorders, such as hemolytic anemias (7.05), disorders of thrombosis and hemostasis (7.08), and disorders of bone marrow failure (7.10). These disorders disrupt the normal development and function of white blood cells, red blood cells, platelets, and clotting-factor proteins (factors).
2. We evaluate malignant (cancerous) hematological disorders, such as lymphoma, leukemia, and multiple myeloma, under the appropriate listings in 13.00, except for two lymphomas associated with human immunodeficiency virus (HIV) infection. We evaluate primary central nervous system lymphoma associated with HIV infection under 14.11B, and primary effusion lymphoma associated with HIV infection under 14.11C.
B. What evidence do we need to document that you have a hematological disorder?
We need the following evidence to document that you have a hematological disorder:
1. A laboratory report of a definitive test that establishes a hematological disorder, signed by a physician; or
2. A laboratory report of a definitive test that establishes a hematological disorder that is not signed by a physician and a report from a physician that states you have the disorder; or
3. When we do not have a laboratory report of a definitive test, a persuasive report from a physician that a diagnosis of your hematological disorder was confirmed by appropriate laboratory analysis or other diagnostic method(s). To be persuasive, this report must state that you had the appropriate definitive laboratory test or tests for diagnosing your disorder and provide the results, or explain how your diagnosis was established by other diagnostic method(s) consistent with the prevailing state of medical knowledge and clinical practice.
4. We will make every reasonable effort to obtain the results of appropriate laboratory testing you have had. We will not purchase complex, costly, or invasive tests, such as tests of clotting-factor proteins, and bone marrow aspirations.
C. What are hemolytic anemias, and how do we evaluate them under 7.05?
1. Hemolytic anemias, both congenital and acquired, are disorders that result in premature destruction of red blood cells (RBCs). Hemolytic disorders include abnormalities of hemoglobin structure (hemoglobinopathies), abnormal RBC enzyme content and function, and RBC membrane (envelope) defects that are congenital or acquired. The diagnosis of hemolytic anemia is based on hemoglobin electrophoresis or analysis of the contents of the RBC (enzymes) and membrane. Examples of congenital hemolytic anemias include sickle cell disease, thalassemia and their variants, and hereditary spherocytosis. Acquired hemolytic anemias may result from autoimmune disease (for example, systemic lupus erythematosus) or mechanical devices (for example, heart valves, intravascular patches).
2. The hospitalizations in 7.05B do not all have to be for the same complication of the hemolytic anemia. They may be for three different complications of the disorder. Examples of complications of hemolytic anemia that may result in hospitalization include osteomyelitis, painful (vaso-occlusive) crisis, pulmonary infections or infarctions, acute chest syndrome, pulmonary hypertension, chronic heart failure, gallbladder disease, hepatic (liver) failure, renal (kidney) failure, nephrotic syndrome, aplastic crisis, and stroke. We will count the hours you receive emergency treatment in a comprehensive sickle cell disease center immediately before the hospitalization if this treatment is comparable to the treatment provided in a hospital emergency department.
3. For 7.05C, we do not require hemoglobin to be measured during a period in which you are free of pain or other symptoms of your disorder. We will accept hemoglobin measurements made while you are experiencing complications of your hemolytic anemia.
4. 7.05D refers to the most serious type of beta thalassemia major in which the bone marrow cannot produce sufficient numbers of normal RBCs to maintain life. The only available treatments for beta thalassemia major are life-long RBC transfusions (sometimes called hypertransfusion) or bone marrow transplantation. For purposes of 7.05D, we do not consider prophylactic RBC transfusions to prevent strokes or other complications in sickle cell disease and its variants to be of equal significance to life-saving RBC transfusions for beta thalassemia major. However, we will consider the functional limitations associated with prophylactic RBC transfusions and any associated side effects (for example, iron overload) under 7.18 and any affected body system(s). We will also evaluate strokes and resulting complications under 11.00 and 12.00.
D. What are disorders of thrombosis and hemostasis, and how do we evaluate them under 7.08?
1. Disorders of thrombosis and hemostasis include both clotting and bleeding disorders, and may be congenital or acquired. These disorders are characterized by abnormalities in blood clotting that result in hypercoagulation (excessive blood clotting) or hypocoagulation (inadequate blood clotting). The diagnosis of a thrombosis or hemostasis disorder is based on evaluation of plasma clotting-factor proteins (factors) and platelets. Protein C or protein S deficiency and Factor V Leiden are examples of hypercoagulation disorders. Hemophilia, von Willebrand disease, and thrombocytopenia are examples of hypocoagulation disorders. Acquired excessive blood clotting may result from blood protein defects and acquired inadequate blood clotting (for example, acquired hemophilia A) may be associated with inhibitor autoantibodies.
2. The hospitalizations in 7.08 do not all have to be for the same complication of a disorder of thrombosis and hemostasis. They may be for three different complications of the disorder. Examples of complications that may result in hospitalization include anemias, thromboses, embolisms, and uncontrolled bleeding requiring multiple factor concentrate infusions or platelet transfusions. We will also consider any surgery that you have, even if it is not related to your hematological disorder, to be a complication of your disorder of thrombosis and hemostasis if you require treatment with clotting-factor proteins (for example, factor VIII or factor IX) or anticoagulant medication to control bleeding or coagulation in connection with your surgery. We will count the hours you receive emergency treatment in a comprehensive hemophilia treatment center immediately before the hospitalization if this treatment is comparable to the treatment provided in a hospital emergency department.
E. What are disorders of bone marrow failure, and how do we evaluate them under 7.10?
1. Disorders of bone marrow failure may be congenital or acquired, characterized by bone marrow that does not make enough healthy RBCs, platelets, or granulocytes (specialized types of white blood cells); there may also be a combined failure of these bone marrow-produced cells. The diagnosis is based on peripheral blood smears and bone marrow aspiration or bone marrow biopsy, but not peripheral blood smears alone. Examples of these disorders are myelodysplastic syndromes, aplastic anemia, granulocytopenia, and myelofibrosis. Acquired disorders of bone marrow failure may result from viral infections, chemical exposure, or immunologic disorders.
2. The hospitalizations in 7.10A do not all have to be for the same complication of bone marrow failure. They may be for three different complications of the disorder. Examples of complications that may result in hospitalization include uncontrolled bleeding, anemia, and systemic bacterial, viral, or fungal infections.
3. For 7.10B, the requirement of life-long RBC transfusions to maintain life in myelodysplastic syndromes or aplastic anemias has the same meaning as it does for beta thalassemia major. (See 7.00C4.)
F. How do we evaluate bone marrow or stem cell transplantation under 7.17?
We will consider you to be disabled for 12 months from the date of bone marrow or stem cell transplantation, or we may consider you to be disabled for a longer period if you are experiencing any serious post-transplantation complications, such as graft-versus-host (GVH) disease, frequent infections after immunosuppressive therapy, or significant deterioration of organ systems. We do not restrict our determination of the onset of disability to the date of the transplantation in 7.17. We may establish an earlier onset date of disability due to your transplantation if evidence in your case record supports such a finding.
G. How do we use the functional criteria in 7.18?
1. When we use the functional criteria in 7.18, we consider all relevant information in your case record to determine the impact of your hematological disorder on your ability to function independently, appropriately, effectively, and on a sustained basis in a work setting. Factors we will consider when we evaluate your functioning under 7.18 include, but are not limited to: Your symptoms, the frequency and duration of complications of your hematological disorder, periods of exacerbation and remission, and the functional impact of your treatment, including the side effects of your medication.
2. Repeated complications means that the complications occur on an average of three times a year, or once every 4 months, each lasting 2 weeks or more; or the complications do not last for 2 weeks but occur substantially more frequently than three times in a year or once every 4 months; or they occur less frequently than an average of three times a year or once every 4 months but last substantially longer than 2 weeks. Your impairment will satisfy this criterion regardless of whether you have the same kind of complication repeatedly, all different complications, or any other combination of complications; for example, two of the same kind of complication and a different one. You must have the required number of complications with the frequency and duration required in this section. Additionally, the complications must occur within the period we are considering in connection with your application or continuing disability review.
3. To satisfy the functional criteria in 7.18, your hematological disorder must result in a “marked” level of limitation in one of three general areas of functioning: Activities of daily living, social functioning, or difficulties in completing tasks due to deficiencies in concentration, persistence, or pace. Functional limitations may result from the impact of the disease process itself on your mental functioning, physical functioning, or both your mental and physical functioning. This limitation could result from persistent or intermittent symptoms, such as pain, severe fatigue, or malaise, resulting in a limitation of your ability to do a task, to concentrate, to persevere at a task, or to perform the task at an acceptable rate of speed. (Severe fatigue means a frequent sense of exhaustion that results in significant reduced physical activity or mental function. Malaise means frequent feelings of illness, bodily discomfort, or lack of well-being that result in significantly reduced physical activity or mental function.) You may also have limitations because of your treatment and its side effects.
4. Marked limitation means that the symptoms and signs of your hematological disorder interfere seriously with your ability to function. Although we do not require the use of such a scale, “marked” would be the fourth point on a five-point scale consisting of no limitation, mild limitation, moderate limitation, marked limitation, and extreme limitation. We do not define “marked” by a specific number of different activities of daily living or different behaviors in which your social functioning is impaired, or a specific number of tasks that you are able to complete, but by the nature and overall degree of interference with your functioning. You may have a marked limitation when several activities or functions are impaired, or even when only one is impaired. Additionally, you need not be totally precluded from performing an activity to have a marked limitation, as long as the degree of limitation interferes seriously with your ability to function independently, appropriately, and effectively. The term “marked” does not imply that you must be confined to bed, hospitalized, or in a nursing home.
5. Activities of daily living include, but are not limited to, such activities as doing household chores, grooming and hygiene, using a post office, taking public transportation, or paying bills. We will find that you have a “marked” limitation in activities of daily living if you have a serious limitation in your ability to maintain a household or take public transportation because of symptoms such as pain, severe fatigue, anxiety, or difficulty concentrating, caused by your hematological disorder (including complications of the disorder) or its treatment, even if you are able to perform some self-care activities.
6. Social functioning includes the capacity to interact with others independently, appropriately, effectively, and on a sustained basis. It includes the ability to communicate effectively with others. We will find that you have a “marked” limitation in maintaining social functioning if you have a serious limitation in social interaction on a sustained basis because of symptoms such as pain, severe fatigue, anxiety, or difficulty concentrating, or a pattern of exacerbation and remission, caused by your hematological disorder (including complications of the disorder) or its treatment, even if you are able to communicate with close friends or relatives.
7. Completing tasks in a timely manner involves the ability to sustain concentration, persistence, or pace to permit timely completion of tasks commonly found in work settings. We will find that you have a “marked” limitation in completing tasks if you have a serious limitation in your ability to sustain concentration or pace adequate to complete work-related tasks because of symptoms, such as pain, severe fatigue, anxiety, or difficulty concentrating caused by your hematological disorder (including complications of the disorder) or its treatment, even if you are able to do some routine activities of daily living.
H. How do we consider your symptoms, including your pain, severe fatigue, and malaise?
Your symptoms, including pain, severe fatigue, and malaise, may be important factors in our determination whether your hematological disorder(s) meets or medically equals a listing, or in our determination whether you are otherwise able to work. We cannot consider your symptoms unless you have medical signs or laboratory findings showing the existence of a medically determinable impairment(s) that could reasonably be expected to produce the symptoms. If you have such an impairment(s), we will evaluate the intensity, persistence, and functional effects of your symptoms using the rules throughout 7.00 and in our other regulations. (See sections 404.1521, 404.1529, 416.921, and 416.929 of this chapter.) Additionally, when we assess the credibility of your complaints about your symptoms and their functional effects, we will not draw any inferences from the fact that you do not receive treatment or that you are not following treatment without considering all of the relevant evidence in your case record, including any explanations you provide that may explain why you are not receiving or following treatment.
I. How do we evaluate episodic events in hematological disorders?
Some of the listings in this body system require a specific number of events within a consecutive 12-month period. (See 7.05, 7.08, and 7.10A.) When we use such criteria, a consecutive 12-month period means a period of 12 consecutive months, all or part of which must occur within the period we are considering in connection with your application or continuing disability review. These events must occur at least 30 days apart to ensure that we are evaluating separate events.
J. How do we evaluate hematological disorders that do not meet one of these listings?
1. These listings are only common examples of hematological disorders that we consider severe enough to prevent a person from doing any gainful activity. If your disorder does not meet the criteria of any of these listings, we must consider whether you have a disorder that satisfies the criteria of a listing in another body system. For example, we will evaluate hemophilic joint deformity or bone or joint pain from myelofibrosis under 1.00; polycythemia vera under 3.00, 4.00, or 11.00; chronic iron overload resulting from repeated RBC transfusion (transfusion hemosiderosis) under 3.00, 4.00, or 5.00; and the effects of intracranial bleeding or stroke under 11.00 or 12.00.
2. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. (See sections 404.1526 and 416.926 of this chapter.) Hematological disorders may be associated with disorders in other body systems, and we consider the combined effects of multiple impairments when we determine whether they medically equal a listing. If your impairment(s) does not medically equal a listing, you may or may not have the residual functional capacity to engage in substantial gainful activity. We proceed to the fourth, and, if necessary, the fifth steps of the sequential evaluation process in sections 404.1520 and 416.920. We use the rules in sections 404.1594, 416.994, and 416.994a of this chapter, as appropriate, when we decide whether you continue to be disabled.
7.01 Category of Impairments, Hematological Disorders
7.05 Hemolytic anemias, including sickle cell disease, thalassemia, and their variants (see 7.00C), with:
A. Documented painful (vaso-occlusive) crises requiring parenteral (intravenous or intramuscular) narcotic medication, occurring at least six times within a 12-month period with at least 30 days between crises.
OR
B. Complications of hemolytic anemia requiring at least three hospitalizations within a 12-month period and occurring at least 30 days apart. Each hospitalization must last at least 48 hours, which can include hours in a hospital emergency department or comprehensive sickle cell disease center immediately before the hospitalization (see 7.00C2).
OR
C. Hemoglobin measurements of 7.0 grams per deciliter (g/dL) or less, occurring at least three times within a 12-month period with at least 30 days between measurements.
OR
D. Beta thalassemia major requiring life-long RBC transfusions at least once every 6 weeks to maintain life (see 7.00C4).
7.08 Disorders of thrombosis and hemostasis, including hemophilia and thrombocytopenia (see 7.00D), with complications requiring at least three hospitalizations within a 12-month period and occurring at least 30 days apart. Each hospitalization must last at least 48 hours, which can include hours in a hospital emergency department or comprehensive hemophilia treatment center immediately before the hospitalization (see 7.00D2).
7.10 Disorders of bone marrow failure, including myelodysplastic syndromes, aplastic anemia, granulocytopenia, and myelofibrosis (see 7.00E), with:
A. Complications of bone marrow failure requiring at least three hospitalizations within a 12-month period and occurring at least 30 days apart. Each hospitalization must last at least 48 hours, which can include hours in a hospital emergency department immediately before the hospitalization (see 7.00E2).
OR
B. Myelodysplastic syndromes or aplastic anemias requiring life-long RBC transfusions at least once every 6 weeks to maintain life (see 7.00E3).
7.17 Hematological disorders treated by bone marrow or stem cell transplantation (see 7.00F). Consider under a disability for at least 12 consecutive months from the date of transplantation. After that, evaluate any residual impairment(s) under the criteria for the affected body system.
7.18 Repeated complications of hematological disorders (see 7.00G2), including those complications listed in 7.05, 7.08, and 7.10 but without the requisite findings for those listings, or other complications (for example, anemia, osteonecrosis, retinopathy, skin ulcers, silent central nervous system infarction, cognitive or other mental limitation, or limitation of joint movement), resulting in significant, documented symptoms or signs (for example, pain, severe fatigue, malaise, fever, night sweats, headaches, joint or muscle swelling, or shortness of breath), and one of the following at the marked level (see 7.00G4):
A. Limitation of activities of daily living (see 7.00G5).
B. Limitation in maintaining social functioning (see 7.00G6).
C. Limitation in completing tasks in a timely manner due to deficiencies in concentration, persistence, or pace (see 7.00G7).
8.00 Skin Disorders
A. What skin disorders do we evaluate with these listings? We use these listings to evaluate skin disorders that may result from hereditary, congenital, or acquired pathological processes. The kinds of impairments covered by these listings are: Ichthyosis, bullous diseases, chronic infections of the skin or mucous membranes, dermatitis, hidradenitis suppurativa, genetic photosensitivity disorders, and burns.
B. What documentation do we need? When we evaluate the existence and severity of your skin disorder, we generally need information about the onset, duration, frequency of flareups, and prognosis of your skin disorder; the location, size, and appearance of lesions; and, when applicable, history of exposure to toxins, allergens, or irritants, familial incidence, seasonal variation, stress factors, and your ability to function outside of a highly protective environment. To confirm the diagnosis, we may need laboratory findings (for example, results of a biopsy obtained independently of Social Security disability evaluation or blood tests) or evidence from other medically acceptable methods consistent with the prevailing state of medical knowledge and clinical practice.
C. How do we assess the severity of your skin disorder(s)? We generally base our assessment of severity on the extent of your skin lesions, the frequency of flareups of your skin lesions, how your symptoms (including pain) limit you, the extent of your treatment, and how your treatment affects you.
1. Extensive skin lesions. Extensive skin lesions are those that involve multiple body sites or critical body areas, and result in a very serious limitation. Examples of extensive skin lesions that result in a very serious limitation include but are not limited to:
a. Skin lesions that interfere with the motion of your joints and that very seriously limit your use of more than one extremity; that is, two upper extremities, two lower extremities, or one upper and one lower extremity.
b. Skin lesions on the palms of both hands that very seriously limit your ability to do fine and gross motor movements.
c. Skin lesions on the soles of both feet, the perineum, or both inguinal areas that very seriously limit your ability to ambulate.
2. Frequency of flareups. If you have skin lesions, but they do not meet the requirements of any of the listings in this body system, you may still have an impairment that prevents you from doing any gainful activity when we consider your condition over time, especially if your flareups result in extensive skin lesions, as defined in C1 of this section. Therefore, if you have frequent flareups, we may find that your impairment(s) is medically equal to one of these listings even though you have some periods during which your condition is in remission. We will consider how frequent and serious your flareups are, how quickly they resolve, and how you function between flareups to determine whether you have been unable to do any gainful activity for a continuous period of at least 12 months or can be expected to be unable to do any gainful activity for a continuous period of at least 12 months. We will also consider the frequency of your flareups when we determine whether you have a severe impairment and when we need to assess your residual functional capacity.
3. Symptoms (including pain). Symptoms (including pain) may be important factors contributing to the severity of your skin disorder(s). We assess the impact of symptoms as explained in §§ 404.1521, 404.1529, 416.921, and 416.929 of this chapter.
4. Treatment. We assess the effects of medication, therapy, surgery, and any other form of treatment you receive when we determine the severity and duration of your impairment(s). Skin disorders frequently respond to treatment; however, response to treatment can vary widely, with some impairments becoming resistant to treatment. Some treatments can have side effects that can in themselves result in limitations.
a. We assess the effects of continuing treatment as prescribed by determining if there is improvement in the symptoms, signs, and laboratory findings of your disorder, and if you experience side effects that result in functional limitations. To assess the effects of your treatment, we may need information about:
i. The treatment you have been prescribed (for example, the type, dosage, method, and frequency of administration of medication or therapy);
ii. Your response to the treatment;
iii. Any adverse effects of the treatment; and
iv. The expected duration of the treatment.
b. Because treatment itself or the effects of treatment may be temporary, in most cases sufficient time must elapse to allow us to evaluate the impact and expected duration of treatment and its side effects. Except under 8.07 and 8.08, you must follow continuing treatment as prescribed for at least 3 months before your impairment can be determined to meet the requirements of a skin disorder listing. (See 8.00H if you are not undergoing treatment or did not have treatment for 3 months.) We consider your specific response to treatment when we evaluate the overall severity of your impairment.
D. How do we assess impairments that may affect the skin and other body systems? When your impairment affects your skin and has effects in other body systems, we first evaluate the predominant feature of your impairment under the appropriate body system. Examples include, but are not limited to the following.
1. Tuberous sclerosis primarily affects the brain. The predominant features are seizures, which we evaluate under the neurological listings in 11.00, and developmental delays or other mental disorders, which we evaluate under the mental disorders listings in 12.00.
2. Malignant tumors of the skin (for example, malignant melanomas) are cancers, or neoplastic diseases, which we evaluate under the listings in 13.00.
3. Autoimmune disorders and other immune system disorders (for example, systemic lupus erythematosus (SLE), scleroderma, human immunodeficiency virus (HIV) infection, and Sjögren's syndrome) often involve more than one body system. We first evaluate these disorders under the immune system disorders listings in 14.00. We evaluate SLE under 14.02, scleroderma under 14.04, Sjögren's syndrome under 14.10, and HIV infection under 14.11.
4. Disfigurement or deformity resulting from skin lesions may result in loss of sight, hearing, speech, and the ability to chew (mastication). We evaluate these impairments and their effects under the special senses and speech listings in 2.00 and the digestive system listings in 5.00. Facial disfigurement or other physical deformities may also have effects we evaluate under the mental disorders listings in 12.00, such as when they affect mood or social functioning.
E. How do we evaluate genetic photosensitivity disorders?
1. Xeroderma pigmentosum (XP). When you have XP, your impairment meets the requirements of 8.07A if you have clinical and laboratory findings showing that you have the disorder. (See 8.00E3.) People who have XP have a lifelong hypersensitivity to all forms of ultraviolet light and generally lead extremely restricted lives in highly protective environments in order to prevent skin cancers from developing. Some people with XP also experience problems with their eyes, neurological problems, mental disorders, and problems in other body systems.
2. Other genetic photosensitivity disorders. Other genetic photosensitivity disorders may vary in their effects on different people, and may not result in an inability to engage in any gainful activity for a continuous period of at least 12 months. Therefore, if you have a genetic photosensitivity disorder other than XP (established by clinical and laboratory findings as described in 8.00E3), you must show that you have either extensive skin lesions or an inability to function outside of a highly protective environment to meet the requirements of 8.07B. You must also show that your impairment meets the duration requirement. By inability to function outside of a highly protective environment we mean that you must avoid exposure to ultraviolet light (including sunlight passing through windows and light from unshielded fluorescent bulbs), wear protective clothing and eyeglasses, and use opaque broad-spectrum sunscreens in order to avoid skin cancer or other serious effects. Some genetic photosensitivity disorders can have very serious effects in other body systems, especially special senses and speech (2.00), neurological (11.00), mental (12.00), and neoplastic (13.00). We will evaluate the predominant feature of your impairment under the appropriate body system, as explained in 8.00D.
3. Clinical and laboratory findings.
a. General. We need documentation from an acceptable medical source to establish that you have a medically determinable impairment. In general, we must have evidence of appropriate laboratory testing showing that you have XP or another genetic photosensitivity disorder. We will find that you have XP or another genetic photosensitivity disorder based on a report from an acceptable medical source indicating that you have the impairment, supported by definitive genetic laboratory studies documenting appropriate chromosomal changes, including abnormal DNA repair or another DNA or genetic abnormality specific to your type of photosensitivity disorder.
b. What we will accept as medical evidence instead of the actual laboratory report. When we do not have the actual laboratory report, we need evidence from an acceptable medical source that includes appropriate clinical findings for your impairment and that is persuasive that a positive diagnosis has been confirmed by appropriate laboratory testing at some time prior to our evaluation. To be persuasive, the report must state that the appropriate definitive genetic laboratory study was conducted and that the results confirmed the diagnosis. The report must be consistent with other evidence in your case record.
F. How do we evaluate burns? Electrical, chemical, or thermal burns frequently affect other body systems; for example, musculoskeletal, special senses and speech, respiratory, cardiovascular, renal, neurological, or mental. Consequently, we evaluate burns the way we evaluate other disorders that can affect the skin and other body systems, using the listing for the predominant feature of your impairment. For example, if your soft tissue injuries are under continuing surgical management (as defined in 1.00M), we will evaluate your impairment under 1.08. However, if your burns do not meet the requirements of 1.08 and you have extensive skin lesions that result in a very serious limitation (as defined in 8.00C1) that has lasted or can be expected to last for a continuous period of at least 12 months, we will evaluate them under 8.08.
G. How do we determine if your skin disorder(s) will continue at a disabling level of severity in order to meet the duration requirement? For all of these skin disorder listings except 8.07 and 8.08, we will find that your impairment meets the duration requirement if your skin disorder results in extensive skin lesions that persist for at least 3 months despite continuing treatment as prescribed. By persist, we mean that the longitudinal clinical record shows that, with few exceptions, your lesions have been at the level of severity specified in the listing. For 8.07A, we will presume that you meet the duration requirement. For 8.07B and 8.08, we will consider all of the relevant medical and other information in your case record to determine whether your skin disorder meets the duration requirement.
H. How do we assess your skin disorder(s) if your impairment does not meet the requirements of one of these listings?
1. These listings are only examples of common skin disorders that we consider severe enough to prevent you from engaging in any gainful activity. For most of these listings, if you do not have continuing treatment as prescribed, if your treatment has not lasted for at least 3 months, or if you do not have extensive skin lesions that have persisted for at least 3 months, your impairment cannot meet the requirements of these skin disorder listings. (This provision does not apply to 8.07 and 8.08.) However, we may still find that you are disabled because your impairment(s) meets the requirements of a listing in another body system or medically equals the severity of a listing. (See §§ 404.1526 and 416.926 of this chapter.) We may also find you disabled at the last step of the sequential evaluation process.
2. If you have not received ongoing treatment or do not have an ongoing relationship with the medical community despite the existence of a severe impairment(s), or if your skin lesions have not persisted for at least 3 months but you are undergoing continuing treatment as prescribed, you may still have an impairment(s) that meets a listing in another body system or that medically equals a listing. If you do not have an impairment(s) that meets or medically equals a listing, we will assess your residual functional capacity and proceed to the fourth and, if necessary, the fifth step of the sequential evaluation process in §§ 404.1520 and 416.920 of this chapter. When we decide whether you continue to be disabled, we use the rules in §§ 404.1594 and 416.994 of this chapter.
8.01 Category of Impairments, Skin Disorders
8.02 Ichthyosis, with extensive skin lesions that persist for at least 3 months despite continuing treatment as prescribed.
8.03 Bullous disease (for example, pemphigus, erythema multiforme bullosum, epidermolysis bullosa, bullous pemphigoid, dermatitis herpetiformis), with extensive skin lesions that persist for at least 3 months despite continuing treatment as prescribed.
8.04 Chronic infections of the skin or mucous membranes, with extensive fungating or extensive ulcerating skin lesions that persist for at least 3 months despite continuing treatment as prescribed.
8.05 Dermatitis (for example, psoriasis, dyshidrosis, atopic dermatitis, exfoliative dermatitis, allergic contact dermatitis), with extensive skin lesions that persist for at least 3 months despite continuing treatment as prescribed.
8.06 Hidradenitis suppurativa, with extensive skin lesions involving both axillae, both inguinal areas or the perineum that persist for at least 3 months despite continuing treatment as prescribed.
8.07 Genetic photosensitivity disorders, established as described in 8.00E.
A. Xeroderma pigmentosum. Consider the individual disabled from birth.
B. Other genetic photosensitivity disorders, with:
1. Extensive skin lesions that have lasted or can be expected to last for a continuous period of at least 12 months, or
2. Inability to function outside of a highly protective environment for a continuous period of at least 12 months (see 8.00E2).
8.08 Burns, with extensive skin lesions that have lasted or can be expected to last for a continuous period of at least 12 months (see 8.00F).
9.00 Endocrine Disorders
A. What is an endocrine disorder?
An endocrine disorder is a medical condition that causes a hormonal imbalance. When an endocrine gland functions abnormally, producing either too much of a specific hormone (hyperfunction) or too little (hypofunction), the hormonal imbalance can cause various complications in the body. The major glands of the endocrine system are the pituitary, thyroid, parathyroid, adrenal, and pancreas.
B. How do we evaluate the effects of endocrine disorders? We evaluate impairments that result from endocrine disorders under the listings for other body systems. For example:
1. Pituitary gland disorders can disrupt hormone production and normal functioning in other endocrine glands and in many body systems. The effects of pituitary gland disorders vary depending on which hormones are involved. For example, when pituitary hypofunction affects water and electrolyte balance in the kidney and leads to diabetes insipidus, we evaluate the effects of recurrent dehydration under 6.00.
2. Thyroid gland disorders affect the sympathetic nervous system and normal metabolism. We evaluate thyroid-related changes in blood pressure and heart rate that cause arrhythmias or other cardiac dysfunction under 4.00; thyroid-related weight loss under 5.00; hypertensive cerebrovascular accidents (strokes) under 11.00; and cognitive limitations, mood disorders, and anxiety under 12.00.
3. Parathyroid gland disorders affect calcium levels in bone, blood, nerves, muscle, and other body tissues. We evaluate parathyroid-related osteoporosis and fractures under 1.00; abnormally elevated calcium levels in the blood (hypercalcemia) that lead to cataracts under 2.00; kidney failure under 6.00; and recurrent abnormally low blood calcium levels (hypocalcemia) that lead to increased excitability of nerves and muscles, such as tetany and muscle spasms, under 11.00.
4. Adrenal gland disorders affect bone calcium levels, blood pressure, metabolism, and mental status. We evaluate adrenal-related osteoporosis with fractures that compromises the ability to walk or to use the upper extremities under 1.00; adrenal-related hypertension that worsens heart failure or causes recurrent arrhythmias under 4.00; adrenal-related weight loss under 5.00; and mood disorders under 12.00.
5. Diabetes mellitus and other pancreatic gland disorders disrupt the production of several hormones, including insulin, that regulate metabolism and digestion. Insulin is essential to the absorption of glucose from the bloodstream into body cells for conversion into cellular energy. The most common pancreatic gland disorder is diabetes mellitus (DM). There are two major types of DM: type 1 and type 2. Both type 1 and type 2 DM are chronic disorders that can have serious disabling complications that meet the duration requirement. Type 1 DM - previously known as “juvenile diabetes” or “insulin-dependent diabetes mellitus” (IDDM) - is an absolute deficiency of insulin production that commonly begins in childhood and continues throughout adulthood. Treatment of type 1 DM always requires lifelong daily insulin. With type 2 DM - previously known as “adult-onset diabetes mellitus” or “non-insulin-dependent diabetes mellitus” (NIDDM) - the body's cells resist the effects of insulin, impairing glucose absorption and metabolism. Treatment of type 2 DM generally requires lifestyle changes, such as increased exercise and dietary modification, and sometimes insulin in addition to other medications. While both type 1 and type 2 DM are usually controlled, some persons do not achieve good control for a variety of reasons including, but not limited to, hypoglycemia unawareness, other disorders that can affect blood glucose levels, inability to manage DM due to a mental disorder, or inadequate treatment.
a. Hyperglycemia. Both types of DM cause hyperglycemia, which is an abnormally high level of blood glucose that may produce acute and long-term complications. Acute complications of hyperglycemia include diabetic ketoacidosis. Long-term complications of chronic hyperglycemia include many conditions affecting various body systems.
(i) Diabetic ketoacidosis (DKA). DKA is an acute, potentially life-threatening complication of DM in which the chemical balance of the body becomes dangerously hyperglycemic and acidic. It results from a severe insulin deficiency, which can occur due to missed or inadequate daily insulin therapy or in association with an acute illness. It usually requires hospital treatment to correct the acute complications of dehydration, electrolyte imbalance, and insulin deficiency. You may have serious complications resulting from your treatment, which we evaluate under the affected body system. For example, we evaluate cardiac arrhythmias under 4.00, intestinal necrosis under 5.00, and cerebral edema and seizures under 11.00. Recurrent episodes of DKA may result from mood or eating disorders, which we evaluate under 12.00.
(ii) Chronic hyperglycemia. Chronic hyperglycemia, which is longstanding abnormally high levels of blood glucose, leads to long-term diabetic complications by disrupting nerve and blood vessel functioning. This disruption can have many different effects in other body systems. For example, we evaluate diabetic peripheral neurovascular disease that leads to gangrene and subsequent amputation of an extremity under 1.00; diabetic retinopathy under 2.00; coronary artery disease and peripheral vascular disease under 4.00; diabetic gastroparesis that results in abnormal gastrointestinal motility under 5.00; diabetic nephropathy under 6.00; poorly healing bacterial and fungal skin infections under 8.00; diabetic peripheral and sensory neuropathies under 11.00; and cognitive impairments, depression, and anxiety under 12.00.
b. Hypoglycemia. Persons with DM may experience episodes of hypoglycemia, which is an abnormally low level of blood glucose. Most adults recognize the symptoms of hypoglycemia and reverse them by consuming substances containing glucose; however, some do not take this step because of hypoglycemia unawareness. Severe hypoglycemia can lead to complications, including seizures or loss of consciousness, which we evaluate under 11.00, or altered mental status and cognitive deficits, which we evaluate under 12.00.
C. How do we evaluate endocrine disorders that do not have effects that meet or medically equal the criteria of any listing in other body systems? If your impairment(s) does not meet or medically equal a listing in another body system, you may or may not have the residual functional capacity to engage in substantial gainful activity. In this situation, we proceed to the fourth and, if necessary, the fifth steps of the sequential evaluation process in §§ 404.1520 and 416.920. When we decide whether you continue to be disabled, we use the rules in §§ 404.1594, 416.994, and 416.994a.
10.00 Congenital Disorders that Affect Multiple Body Systems
A. Which disorder do we evaluate under this body system? Although Down syndrome exists in non-mosaic and mosaic forms, we evaluate only non-mosaic Down syndrome under this body system.
B. What is non-mosaic Down syndrome? Non-mosaic Down syndrome is a genetic disorder. Most people with non-mosaic Down syndrome have three copies of chromosome 21 in all of their cells (chromosome 21 trisomy); some have an extra copy of chromosome 21 attached to a different chromosome in all of their cells (chromosome 21 translocation). Virtually all people with non-mosaic Down syndrome have characteristic facial or other physical features, delayed physical development, and intellectual disability. People with non-mosaic Down syndrome may also have congenital heart disease, impaired vision, hearing problems, and other disorders. We evaluate non-mosaic Down syndrome under 10.06. If you have non-mosaic Down syndrome documented as described in 10.00C, we consider you disabled from birth.
C. What evidence do we need to document non-mosaic Down syndrome under 10.06?
1. Under 10.06A, we will find you disabled based on laboratory findings.
a. To find that your disorder meets 10.06A, we need a copy of the laboratory report of karyotype analysis, which is the definitive test to establish non-mosaic Down syndrome. We will not purchase karyotype analysis. We will not accept a fluorescence in situ hybridization (FISH) test because it does not distinguish between the mosaic and non-mosaic forms of Down syndrome.
b. If a physician (see §§ 404.1513(a)(1) and 416.913(a)(1) of this chapter) has not signed the laboratory report of karyotype analysis, the evidence must also include a physician's statement that you have Down syndrome.
c. For purposes of 10.06A, we do not require additional evidence stating that you have the distinctive facial or other physical features of Down syndrome.
2. If we do not have a laboratory report of karyotype analysis showing that you have non-mosaic Down syndrome, we may find you disabled under 10.06B or 10.06C.
a. Under 10.06B, we need a physician's report stating: (i) your karyotype diagnosis or evidence that documents your type of Down syndrome is consistent with prior karyotype analysis (for example, reference to a diagnosis of “trisomy 21”), and (ii) that you have the distinctive facial or other physical features of Down syndrome. We do not require a detailed description of the facial or other physical features of the disorder. However, we will not find that your disorder meets 10.06B if we have evidence - such as evidence of functioning inconsistent with the diagnosis - that indicates that you do not have non-mosaic Down syndrome.
b. If we do not have evidence of prior karyotype analysis (you did not have testing, or you had testing but we do not have information from a physician about the test results), we will find that your disorder meets 10.06C if we have: (i) a physician's report stating that you have the distinctive facial or other physical features of Down syndrome, and (ii) evidence that your functioning is consistent with a diagnosis of non-mosaic Down syndrome. This evidence may include medical or nonmedical information about your physical and mental abilities, including information about your education, work history, or the results of psychological testing. However, we will not find that your disorder meets 10.06C if we have evidence - such as evidence of functioning inconsistent with the diagnosis - that indicates that you do not have non-mosaic Down syndrome.
D. How do we evaluate mosaic Down syndrome and other congenital disorders that affect multiple body systems?
1. Mosaic Down syndrome. Approximately 2 percent of people with Down syndrome have the mosaic form. In mosaic Down syndrome, there are some cells with an extra copy of chromosome 21 and other cells with the normal two copies of chromosome 21. Mosaic Down syndrome can be so slight as to be undetected clinically, but it can also be profound and disabling, affecting various body systems.
2. Other congenital disorders that affect multiple body systems. Other congenital disorders, such as congenital anomalies, chromosomal disorders, dysmorphic syndromes, inborn metabolic syndromes, and perinatal infectious diseases, can cause deviation from, or interruption of, the normal function of the body or can interfere with development. Examples of these disorders include both the juvenile and late-onset forms of Tay-Sachs disease, trisomy X syndrome (XXX syndrome), fragile X syndrome, phenylketonuria (PKU), caudal regression syndrome, and fetal alcohol syndrome. For these disorders and other disorders like them, the degree of deviation, interruption, or interference, as well as the resulting functional limitations and their progression, may vary widely from person to person and may affect different body systems.
3. Evaluating the effects of mosaic Down syndrome or another congenital disorder under the listings. When the effects of mosaic Down syndrome or another congenital disorder that affects multiple body systems are sufficiently severe we evaluate the disorder under the appropriate affected body system(s), such as musculoskeletal, special senses and speech, neurological, or mental disorders. Otherwise, we evaluate the specific functional limitations that result from the disorder under our other rules described in 10.00E.
E. What if your disorder does not meet a listing?
If you have a severe medically determinable impairment(s) that does not meet a listing, we will consider whether your impairment(s) medically equals a listing. See §§ 404.1526 and 416.926 of this chapter. If your impairment(s) does not meet or medically equal a listing, you may or may not have the residual functional capacity to engage in substantial gainful activity. We proceed to the fourth, and if necessary, the fifth steps of the sequential evaluation process in §§ 404.1520 and 416.920 of this chapter. We use the rules in §§ 404.1594 and 416.994 of this chapter, as appropriate, when we decide whether you continue to be disabled.
10.01 Category of Impairments, Congenital Disorders That Affect Multiple Body Systems
10.06 Non-mosaic Down syndrome (chromosome 21 trisomy or chromosome 21 translocation), documented by:
A. A laboratory report of karyotype analysis signed by a physician, or both a laboratory report of karyotype analysis not signed by a physician and a statement by a physician that you have Down syndrome (see 10.00C1), or
B. A physician's report stating that you have chromosome 21 trisomy or chromosome 21 translocation consistent with prior karyotype analysis with the distinctive facial or other physical features of Down syndrome (see 10.00C2a), or
C. A physician's report stating that you have Down syndrome with the distinctive facial or other physical features and evidence demonstrating that you function at a level consistent with non-mosaic Down syndrome (see 10.00C2b).
11.00 Neurological Disorders
A. Which neurological disorders do we evaluate under these listings? We evaluate epilepsy, amyotrophic lateral sclerosis, coma or persistent vegetative state (PVS), and neurological disorders that cause disorganization of motor function, bulbar and neuromuscular dysfunction, communication impairment, or a combination of limitations in physical and mental functioning. We evaluate neurological disorders that may manifest in a combination of limitations in physical and mental functioning. For example, if you have a neurological disorder that causes mental limitations, such as Huntington's disease or early-onset Alzheimer's disease, which may limit executive functioning (e.g., regulating attention, planning, inhibiting responses, decision-making), we evaluate your limitations using the functional criteria under these listings (see 11.00G). Under this body system, we evaluate the limitations resulting from the impact of the neurological disease process itself. If your neurological disorder results in only mental impairment or if you have a co-occurring mental condition that is not caused by your neurological disorder (for example, dementia), we will evaluate your mental impairment under the mental disorders body system, 12.00.
B. What evidence do we need to document your neurological disorder?
1. We need both medical and non-medical evidence (signs, symptoms, and laboratory findings) to assess the effects of your neurological disorder. Medical evidence should include your medical history, examination findings, relevant laboratory tests, and the results of imaging. Imaging refers to medical imaging techniques, such as x-ray, computerized tomography (CT), magnetic resonance imaging (MRI), and electroencephalography (EEG). The imaging must be consistent with the prevailing state of medical knowledge and clinical practice as the proper technique to support the evaluation of the disorder. In addition, the medical evidence may include descriptions of any prescribed treatment and your response to it. We consider non-medical evidence such as statements you or others make about your impairments, your restrictions, your daily activities, or your efforts to work.
2. We will make every reasonable effort to obtain the results of your laboratory and imaging evidence. When the results of any of these tests are part of the existing evidence in your case record, we will evaluate the test results and all other relevant evidence. We will not purchase imaging, or other diagnostic tests, or laboratory tests that are complex, may involve significant risk, or that are invasive. We will not routinely purchase tests that are expensive or not readily available.
C. How do we consider adherence to prescribed treatment in neurological disorders? In 11.02 (Epilepsy), 11.06 (Parkinsonian syndrome), and 11.12 (Myasthenia gravis), we require that limitations from these neurological disorders exist despite adherence to prescribed treatment. “Despite adherence to prescribed treatment” means that you have taken medication(s) or followed other treatment procedures for your neurological disorder(s) as prescribed by a physician for three consecutive months but your impairment continues to meet the other listing requirements despite this treatment. You may receive your treatment at a health care facility that you visit regularly, even if you do not see the same physician on each visit.
D. What do we mean by disorganization of motor function?
1. Disorganization of motor function means interference, due to your neurological disorder, with movement of two extremities; i.e., the lower extremities, or upper extremities (including fingers, wrists, hands, arms, and shoulders). By two extremities we mean both lower extremities, or both upper extremities, or one upper extremity and one lower extremity. All listings in this body system, except for 11.02 (Epilepsy), 11.10 (Amyotrophic lateral sclerosis), and 11.20 (Coma and persistent vegetative state), include criteria for disorganization of motor function that results in an extreme limitation in your ability to:
a. Stand up from a seated position; or
b. Balance while standing or walking; or
c. Use the upper extremities (including fingers, wrists, hands, arms, and shoulders).
2. Extreme limitation means the inability to stand up from a seated position, maintain balance in a standing position and while walking, or use your upper extremities to independently initiate, sustain, and complete work-related activities. The assessment of motor function depends on the degree of interference with standing up; balancing while standing or walking; or using the upper extremities (including fingers, hands, arms, and shoulders).
a. Inability to stand up from a seated position means that once seated you are unable to stand and maintain an upright position without the assistance of another person or the use of an assistive device, such as a walker, two crutches, or two canes.
b. Inability to maintain balance in a standing position means that you are unable to maintain an upright position while standing or walking without the assistance of another person or an assistive device, such as a walker, two crutches, or two canes.
c. Inability to use your upper extremities means that you have a loss of function of both upper extremities (including fingers, wrists, hands, arms, and shoulders) that very seriously limits your ability to independently initiate, sustain, and complete work-related activities involving fine and gross motor movements. Inability to perform fine and gross motor movements could include not being able to pinch, manipulate, and use your fingers; or not being able to use your hands, arms, and shoulders to perform gross motor movements, such as handling, gripping, grasping, holding, turning, and reaching; or not being able to engage in exertional movements such a lifting, carrying, pushing, and pulling.
E. How do we evaluate communication impairments under these listings? We must have a description of a recent comprehensive evaluation including all areas of communication, performed by an acceptable medical source, to document a communication impairment associated with a neurological disorder. A communication impairment may occur when a medically determinable neurological impairment results in dysfunction in the parts of the brain responsible for speech and language. We evaluate communication impairments associated with neurological disorders under 11.04A, 11.07C, or 11.11B. We evaluate communication impairments due to non-neurological disorders under 2.09.
1. Under 11.04A, we need evidence documenting that your central nervous system vascular accident or insult (CVA) and sensory or motor aphasia have resulted in ineffective speech or communication. Ineffective speech or communication means there is an extreme limitation in your ability to understand or convey your message in simple spoken language resulting in your inability to demonstrate basic communication skills, such as following one-step commands or telling someone about your basic personal needs without assistance.
2. Under 11.07C, we need evidence documenting that your cerebral palsy has resulted in significant interference in your ability to speak, hear, or see. We will find you have “significant interference” in your ability to speak, hear, or see if your signs, such as aphasia, strabismus, or sensorineural hearing loss, seriously limit your ability to communicate on a sustained basis.
3. Under 11.11B, we need evidence documenting that your post-polio syndrome has resulted in the inability to produce intelligible speech.
F. What do we mean by bulbar and neuromuscular dysfunction? The bulbar region of the brain is responsible for controlling the bulbar muscles in the throat, tongue, jaw, and face. Bulbar and neuromuscular dysfunction refers to weakness in these muscles, resulting in breathing, swallowing, and speaking impairments. Listings 11.11 (Post-polio syndrome), 11.12 (Myasthenia gravis), and 11.22 (Motor neuron disorders other than ALS) include criteria for evaluating bulbar and neuromuscular dysfunction. If your neurological disorder has resulted in a breathing disorder, we may evaluate that condition under the respiratory system, 3.00.
G. How do we evaluate limitations in physical and mental functioning under these listings?
1. Neurological disorders may manifest in a combination of limitations in physical and mental functioning. We consider all relevant information in your case record to determine the effects of your neurological disorder on your physical and mental functioning. To satisfy the requirement described under 11.00G, your neurological disorder must result in a marked limitation in physical functioning and a marked limitation in at least one of four areas of mental functioning: Understanding, remembering, or applying information; interacting with others; concentrating, persisting, or maintaining pace; or adapting or managing oneself. If your neurological disorder results in an extreme limitation in at least one of the four areas of mental functioning, or results in marked limitation in at least two of the four areas of mental functioning, but you do not have at least a marked limitation in your physical functioning, we will consider whether your condition meets or medically equals one of the mental disorders body system listings, 12.00.
2. Marked Limitation. To satisfy the requirements of the functional criteria, your neurological disorder must result in a marked limitation in physical functioning and a marked limitation in one of the four areas of mental functioning (see 11.00G3). Although we do not require the use of such a scale, “marked” would be the fourth point on a five-point scale consisting of no limitation, mild limitation, moderate limitation, marked limitation, and extreme limitation. We consider the nature and overall degree of interference with your functioning. The term “marked” does not require that you must be confined to bed, hospitalized, or in a nursing home.
a. Marked limitation and physical functioning. For this criterion, a marked limitation means that, due to the signs and symptoms of your neurological disorder, you are seriously limited in the ability to independently initiate, sustain, and complete work-related physical activities (see 11.00G3). You may have a marked limitation in your physical functioning when your neurological disease process causes persistent or intermittent symptoms that affect your abilities to independently initiate, sustain, and complete work-related activities, such as standing, balancing, walking, using both upper extremities for fine and gross movements, or results in limitations in using one upper and one lower extremity. The persistent and intermittent symptoms must result in a serious limitation in your ability to do a task or activity on a sustained basis. We do not define “marked” by a specific number of different physical activities or tasks that demonstrate your ability, but by the overall effects of your neurological symptoms on your ability to perform such physical activities on a consistent and sustained basis. You need not be totally precluded from performing a function or activity to have a marked limitation, as long as the degree of limitation seriously limits your ability to independently initiate, sustain, and complete work-related physical activities.
b. Marked limitation and mental functioning. For this criterion, a marked limitation means that, due to the signs and symptoms of your neurological disorder, you are seriously limited in the ability to function independently, appropriately, effectively, and on a sustained basis in work settings (see 11.03G3). We do not define “marked” by a specific number of mental activities, such as: The number of activities that demonstrate your ability to understand, remember, and apply information; the number of tasks that demonstrate your ability to interact with others; a specific number of tasks that demonstrate you are able to concentrate, persist or maintain pace; or a specific number of tasks that demonstrate you are able to manage yourself. You may have a marked limitation in your mental functioning when several activities or functions are impaired, or even when only one is impaired. You need not be totally precluded from performing an activity to have a marked limitation, as long as the degree of limitation seriously limits your ability to function independently, appropriately, and effectively on a sustained basis, and complete work-related mental activities.
3. Areas of physical and mental functioning.
a. Physical functioning. Examples of this criterion include specific motor abilities, such as independently initiating, sustaining, and completing the following activities: Standing up from a seated position, balancing while standing or walking, or using both your upper extremities for fine and gross movements (see 11.00D). Physical functioning may also include functions of the body that support motor abilities, such as the abilities to see, breathe, and swallow (see 11.00E and 11.00F). Examples of when your limitation in seeing, breathing, or swallowing may, on its own, rise to a “marked” limitation include: Prolonged and uncorrectable double vision causing difficulty with balance; prolonged difficulty breathing requiring the use of a prescribed assistive breathing device, such as a portable continuous positive airway pressure machine; or repeated instances, occurring at least weekly, of aspiration without causing aspiration pneumonia. Alternatively, you may have a combination of limitations due to your neurological disorder that together rise to a “marked” limitation in physical functioning. We may also find that you have a “marked” limitation in this area if, for example, your symptoms, such as pain or fatigue (see 11.00T), as documented in your medical record, and caused by your neurological disorder or its treatment, seriously limit your ability to independently initiate, sustain, and complete these work-related motor functions, or the other physical functions or physiological processes that support those motor functions. We may also find you seriously limited in an area if, while you retain some ability to perform the function, you are unable to do so consistently and on a sustained basis. The limitation in your physical functioning must last or be expected to last at least 12 months. These examples illustrate the nature of physical functioning. We do not require documentation of all of the examples.
b. Mental functioning.
(i) Understanding, remembering, or applying information. This area of mental functioning refers to the abilities to learn, recall, and use information to perform work activities. Examples include: Understanding and learning terms, instructions, procedures; following one- or two-step oral instructions to carry out a task; describing work activity to someone else; asking and answering questions and providing explanations; recognizing a mistake and correcting it; identifying and solving problems; sequencing multi-step activities; and using reason and judgment to make work-related decisions. These examples illustrate the nature of this area of mental functioning. We do not require documentation of all of the examples.
(ii) Interacting with others. This area of mental functioning refers to the abilities to relate to and work with supervisors, co-workers, and the public. Examples include: Cooperating with others; asking for help when needed; handling conflicts with others; stating your own point of view; initiating or sustaining conversation; understanding and responding to social cues (physical, verbal, emotional); responding to requests, suggestions, criticism, correction, and challenges; and keeping social interactions free of excessive irritability, sensitivity, argumentativeness, or suspiciousness. These examples illustrate the nature of this area of mental functioning. We do not require documentation of all of the examples.
(iii) Concentrating, persisting, or maintaining pace. This area of mental functioning refers to the abilities to focus attention on work activities and to stay on-task at a sustained rate. Examples include: Initiating and performing a task that you understand and know how to do; working at an appropriate and consistent pace; completing tasks in a timely manner; ignoring or avoiding distractions while working; changing activities or work settings without being disruptive; working close to or with others without interrupting or distracting them; sustaining an ordinary routine and regular attendance at work; and working a full day without needing more than the allotted number or length of rest periods during the day. These examples illustrate the nature of this area of mental functioning. We do not require documentation of all of the examples.
(iv) Adapting or managing oneself. This area of mental functioning refers to the abilities to regulate emotions, control behavior, and maintain well-being in a work setting. Examples include: Responding to demands; adapting to changes; managing your psychologically based symptoms; distinguishing between acceptable and unacceptable work performance; setting realistic goals; making plans for yourself independently of others; maintaining personal hygiene and attire appropriate to a work setting; and being aware of normal hazards and taking appropriate precautions. These examples illustrate the nature of this area of mental functioning. We do not require documentation of all of the examples.
4. Signs and symptoms of your disorder and the effects of treatment.
a. We will consider your signs and symptoms and how they affect your ability to function in the work place. When we evaluate your functioning, we will consider whether your signs and symptoms are persistent or intermittent, how frequently they occur and how long they last, their intensity, and whether you have periods of exacerbation and remission.
b. We will consider the effectiveness of treatment in improving the signs, symptoms, and laboratory findings related to your neurological disorder, as well as any aspects of treatment that may interfere with your ability to function. We will consider, for example: The effects of medications you take (including side effects); the time-limited efficacy of some medications; the intrusiveness, complexity, and duration of your treatment (for example, the dosing schedule or need for injections); the effects of treatment, including medications, therapy, and surgery, on your functioning; the variability of your response to treatment; and any drug interactions.
H. What is epilepsy, and how do we evaluate it under 11.02?
1. Epilepsy is a pattern of recurrent and unprovoked seizures that are manifestations of abnormal electrical activity in the brain. There are various types of generalized and “focal” or partial seizures. However, psychogenic nonepileptic seizures and pseudoseizures are not epileptic seizures for the purpose of 11.02. We evaluate psychogenic seizures and pseudoseizures under the mental disorders body system, 12.00. In adults, the most common potentially disabling seizure types are generalized tonic-clonic seizures and dyscognitive seizures (formerly complex partial seizures).
a. Generalized tonic-clonic seizures are characterized by loss of consciousness accompanied by a tonic phase (sudden muscle tensing causing the person to lose postural control) followed by a clonic phase (rapid cycles of muscle contraction and relaxation, also called convulsions). Tongue biting and incontinence may occur during generalized tonic-clonic seizures, and injuries may result from falling.
b. Dyscognitive seizures are characterized by alteration of consciousness without convulsions or loss of muscle control. During the seizure, blank staring, change of facial expression, and automatisms (such as lip smacking, chewing or swallowing, or repetitive simple actions, such as gestures or verbal utterances) may occur. During its course, a dyscognitive seizure may progress into a generalized tonic-clonic seizure (see 11.00H1a).
2. Description of seizure. We require at least one detailed description of your seizures from someone, preferably a medical professional, who has observed at least one of your typical seizures. If you experience more than one type of seizure, we require a description of each type.
3. Serum drug levels. We do not require serum drug levels; therefore, we will not purchase them. However, if serum drug levels are available in your medical records, we will evaluate them in the context of the other evidence in your case record.
4. Counting seizures. The period specified in 11.02A, B, C, or D cannot begin earlier than one month after you began prescribed treatment. The required number of seizures must occur within the period we are considering in connection with your application or continuing disability review. When we evaluate the frequency of your seizures, we also consider your adherence to prescribed treatment (see 11.00C). When we determine the number of seizures you have had in the specified period, we will:
a. Count multiple seizures occurring in a 24-hour period as one seizure.
b. Count status epilepticus (a continuous series of seizures without return to consciousness between seizures) as one seizure.
c. Count a dyscognitive seizure that progresses into a generalized tonic-clonic seizure as one generalized tonic-clonic seizure.
d. We do not count seizures that occur during a period when you are not adhering to prescribed treatment without good reason. When we determine that you had good reason for not adhering to prescribed treatment, we will consider your physical, mental, educational, and communicative limitations (including any language barriers). We will consider you to have good reason for not following prescribed treatment if, for example, the treatment is very risky for you due to its consequences or unusual nature, or if you are unable to afford prescribed treatment that you are willing to accept, but for which no free community resources are available. We will follow guidelines found in our policy, such as §§ 404.1530(c) and 416.930(c) of this chapter, when we determine whether you have a good reason for not adhering to prescribed treatment.
e. We do not count psychogenic nonepileptic seizures or pseudoseizures under 11.02. We evaluate these seizures under the mental disorders body system, 12.00.
5. Electroencephalography (EEG) testing. We do not require EEG test results; therefore, we will not purchase them. However, if EEG test results are available in your medical records, we will evaluate them in the context of the other evidence in your case record.
I. What is vascular insult to the brain, and how do we evaluate it under 11.04?
1. Vascular insult to the brain (cerebrum, cerebellum, or brainstem), commonly referred to as stroke or cerebrovascular accident (CVA), is brain cell death caused by an interruption of blood flow within or leading to the brain, or by a hemorrhage from a ruptured blood vessel or aneurysm in the brain. If you have a vision impairment resulting from your vascular insult, we may evaluate that impairment under the special senses body system, 2.00.
2. We need evidence of sensory or motor aphasia that results in ineffective speech or communication under 11.04A (see 11.00E). We may evaluate your communication impairment under listing 11.04C if you have marked limitation in physical functioning and marked limitation in one of the four areas of mental functioning.
3. We generally need evidence from at least 3 months after the vascular insult to evaluate whether you have disorganization of motor functioning under 11.04B, or the impact that your disorder has on your physical and mental functioning under 11.04C. In some cases, evidence of your vascular insult is sufficient to allow your claim within 3 months post-vascular insult. If we are unable to allow your claim within 3 months after your vascular insult, we will defer adjudication of the claim until we obtain evidence of your neurological disorder at least 3 months post-vascular insult.
J. What are benign brain tumors, and how do we evaluate them under 11.05? Benign brain tumors are noncancerous (nonmalignant) abnormal growths of tissue in or on the brain that invade healthy brain tissue or apply pressure on the brain or cranial nerves. We evaluate their effects on your functioning as discussed in 11.00D and 11.00G. We evaluate malignant brain tumors under the cancer body system in 13.00. If you have a vision impairment resulting from your benign brain tumor, we may evaluate that impairment under the special senses body system, 2.00.
K. What is Parkinsonian syndrome, and how do we evaluate it under 11.06? Parkinsonian syndrome is a term that describes a group of chronic, progressive movement disorders resulting from loss or decline in the function of dopamine-producing brain cells. Dopamine is a neurotransmitter that regulates muscle movement throughout the body. When we evaluate your Parkinsonian syndrome, we will consider your adherence to prescribed treatment (see 11.00C).
L. What is cerebral palsy, and how do we evaluate it under 11.07?
1. Cerebral palsy (CP) is a term that describes a group of static, nonprogressive disorders caused by abnormalities within the brain that disrupt the brain's ability to control movement, muscle coordination, and posture. The resulting motor deficits manifest very early in a person's development, with delayed or abnormal progress in attaining developmental milestones. Deficits may become more obvious as the person grows and matures over time.
2. We evaluate your signs and symptoms, such as ataxia, spasticity, flaccidity, athetosis, chorea, and difficulty with precise movements when we determine your ability to stand up, balance, walk, or perform fine and gross motor movements. We will also evaluate your signs, such as dysarthria and apraxia of speech, and receptive and expressive language problems when we determine your ability to communicate.
3. We will consider your other impairments or signs and symptoms that develop secondary to the disorder, such as post-impairment syndrome (a combination of pain, fatigue, and weakness due to muscle abnormalities); overuse syndromes (repetitive motion injuries); arthritis; abnormalities of proprioception (perception of the movements and position of the body); abnormalities of stereognosis (perception and identification of objects by touch); learning problems; anxiety; and depression.
M. What are spinal cord disorders, and how do we evaluate them under 11.08?
1. Spinal cord disorders may be congenital or caused by injury to the spinal cord. Motor signs and symptoms of spinal cord disorders include paralysis, flaccidity, spasticity, and weakness.
2. Spinal cord disorders with complete loss of function (11.08A) addresses spinal cord disorders that result in a complete lack of motor, sensory, and autonomic function of the affected part(s) of the body.
3. Spinal cord disorders with disorganization of motor function (11.08B) addresses spinal cord disorders that result in less than a complete loss of function of the affected part(s) of the body, reducing, but not eliminating, motor, sensory, and autonomic function.
4. When we evaluate your spinal cord disorder, we generally need evidence from at least 3 months after your symptoms began in order to evaluate your disorganization of motor function. In some cases, evidence of your spinal cord disorder may be sufficient to allow your claim within 3 months after the spinal cord disorder. If the medical evidence demonstrates total cord transection causing a loss of motor and sensory functions below the level of injury, we will not wait 3 months but will make the allowance decision immediately.
N. What is multiple sclerosis, and how do we evaluate it under 11.09?
1. Multiple sclerosis (MS) is a chronic, inflammatory, degenerative disorder that damages the myelin sheath surrounding the nerve fibers in the brain and spinal cord. The damage disrupts the normal transmission of nerve impulses within the brain and between the brain and other parts of the body, causing impairment in muscle coordination, strength, balance, sensation, and vision. There are several forms of MS, ranging from mildly to highly aggressive. Milder forms generally involve acute attacks (exacerbations) with partial or complete recovery from signs and symptoms (remissions). Aggressive forms generally exhibit a steady progression of signs and symptoms with few or no remissions. The effects of all forms vary from person to person.
2. We evaluate your signs and symptoms, such as flaccidity, spasticity, spasms, incoordination, imbalance, tremor, physical fatigue, muscle weakness, dizziness, tingling, and numbness when we determine your ability to stand up, balance, walk, or perform fine and gross motor movements. When determining whether you have limitations of physical and mental functioning, we will consider your other impairments or signs and symptoms that develop secondary to the disorder, such as fatigue; visual loss; trouble sleeping; impaired attention, concentration, memory, or judgment; mood swings; and depression. If you have a vision impairment resulting from your MS, we may evaluate that impairment under the special senses body system, 2.00.
O. What is amyotrophic lateral sclerosis, and how do we evaluate it under 11.10? Amyotrophic lateral sclerosis (ALS) is a type of motor neuron disorder that rapidly and progressively attacks the nerve cells responsible for controlling voluntary muscles. We establish ALS under 11.10 when you have a documented diagnosis of ALS. We require documentation based on generally accepted methods consistent with the prevailing state of medical knowledge and clinical practice. We require laboratory testing to establish the diagnosis when the clinical findings of upper and lower motor neuron disease are not present in three or more regions. Electrophysiological studies, such as nerve conduction velocity studies and electromyography (EMG), may support your diagnosis of ALS; however, we will not purchase these studies.
P. What are neurodegenerative disorders of the central nervous system, such as Huntington's disease, Friedreich's ataxia, and spinocerebellar degeneration, and how do we evaluate them under 11.17? Neurodegenerative disorders of the central nervous system are disorders characterized by progressive and irreversible degeneration of neurons or their supporting cells. Over time, these disorders impair many of the body's motor, cognitive, and other mental functions. We consider neurodegenerative disorders of the central nervous system under 11.17 that we do not evaluate elsewhere in section 11.00, such as Huntington's disease (HD), Friedreich's ataxia, spinocerebellar degeneration, Creutzfeldt-Jakob disease (CJD), progressive supranuclear palsy (PSP), early-onset Alzheimer's disease, and frontotemporal dementia (Pick's disease). When these disorders result in solely cognitive and other mental function effects, we will evaluate the disorder under the mental disorder listings.
Q. What is traumatic brain injury, and how do we evaluate it under 11.18?
1. Traumatic brain injury (TBI) is damage to the brain resulting from skull fracture, collision with an external force leading to a closed head injury, or penetration by an object that enters the skull and makes contact with brain tissue. We evaluate TBI that results in coma or persistent vegetative state (PVS) under 11.20.
2. We generally need evidence from at least 3 months after the TBI to evaluate whether you have disorganization of motor function under 11.18A or the impact that your disorder has on your physical and mental functioning under 11.18B. In some cases, evidence of your TBI is sufficient to determine disability within 3 months post-TBI. If we are unable to allow your claim within 3 months post-TBI, we will defer adjudication of the claim until we obtain evidence of your neurological disorder at least 3 months post-TBI. If a finding of disability still is not possible at that time, we will again defer adjudication of the claim until we obtain evidence at least 6 months after your TBI.
R. What are coma and persistent vegetative state, and how do we evaluate them under 11.20? Coma is a state of unconsciousness in which a person does not exhibit a sleep/wake cycle, and is unable to perceive or respond to external stimuli. People who do not fully emerge from coma may progress into a persistent vegetative state (PVS). PVS is a condition of partial arousal in which a person may have a low level of consciousness but is still unable to react to external stimuli. In contrast to coma, a person in a PVS retains sleep/wake cycles and may exhibit some key lower brain functions, such as spontaneous movement, opening and moving eyes, and grimacing. Coma or PVS may result from TBI, a nontraumatic insult to the brain (such as a vascular insult, infection, or brain tumor), or a neurodegenerative or metabolic disorder. Medically induced comas are not considered under 11.20 and should be considered under the section pertaining to the underlying reason the coma was medically induced and not under this section.
S. What are motor neuron disorders, other than ALS, and how do we evaluate them under 11.22? Motor neuron disorders such as progressive bulbar palsy, primary lateral sclerosis (PLS), and spinal muscular atrophy (SMA) are progressive neurological disorders that destroy the cells that control voluntary muscle activity, such as walking, breathing, swallowing, and speaking. We evaluate the effects of these disorders on motor functioning, bulbar and neuromuscular functioning, oral communication, or limitations in physical and mental functioning.
T. How do we consider symptoms of fatigue in these listings? Fatigue is one of the most common and limiting symptoms of some neurological disorders, such as multiple sclerosis, post-polio syndrome, and myasthenia gravis. These disorders may result in physical fatigue (lack of muscle strength) or mental fatigue (decreased awareness or attention). When we evaluate your fatigue, we will consider the intensity, persistence, and effects of fatigue on your functioning. This may include information such as the clinical and laboratory data and other objective evidence concerning your neurological deficit, a description of fatigue considered characteristic of your disorder, and information about your functioning. We consider the effects of physical fatigue on your ability to stand up, balance, walk, or perform fine and gross motor movements using the criteria described in 11.00D. We consider the effects of physical and mental fatigue when we evaluate your physical and mental functioning described in 11.00G.
U. How do we evaluate your neurological disorder when it does not meet one of these listings?
1. If your neurological disorder does not meet the criteria of any of these listings, we must also consider whether your impairment(s) meets the criteria of a listing in another body system. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. See §§ 404.1526 and 416.926 of this chapter.
2. If your impairment(s) does not meet or medically equal the criteria of a listing, you may or may not have the residual functional capacity to perform your past relevant work or adjust to other work that exists in significant numbers in the national economy, which we determine at the fourth and, if necessary, the fifth steps of the sequential evaluation process in §§ 404.1520 and 416.920 of this chapter.
3. We use the rules in §§ 404.1594 and 416.994 of this chapter, as appropriate, when we decide whether you continue to be disabled.
11.01 Category of Impairments, Neurological Disorders
11.02 Epilepsy, documented by a detailed description of a typical seizure and characterized by A, B, C, or D:
A. Generalized tonic-clonic seizures (see 11.00H1a), occurring at least once a month for at least 3 consecutive months (see 11.00H4) despite adherence to prescribed treatment (see 11.00C); or
B. Dyscognitive seizures (see 11.00H1b), occurring at least once a week for at least 3 consecutive months (see 11.00H4) despite adherence to prescribed treatment (see 11.00C); or
C. Generalized tonic-clonic seizures (see 11.00H1a), occurring at least once every 2 months for at least 4 consecutive months (see 11.00H4) despite adherence to prescribed treatment (see 11.00C); and a marked limitation in one of the following:
1. Physical functioning (see 11.00G3a); or
2. Understanding, remembering, or applying information (see 11.00G3b(i)); or
3. Interacting with others (see 11.00G3b(ii)); or
4. Concentrating, persisting, or maintaining pace (see 11.00G3b(iii)); or
5. Adapting or managing oneself (see 11.00G3b(iv)); or
D. Dyscognitive seizures (see 11.00H1b), occurring at least once every 2 weeks for at least 3 consecutive months (see 11.00H4) despite adherence to prescribed treatment (see 11.00C); and a marked limitation in one of the following:
1. Physical functioning (see 11.00G3a); or
2. Understanding, remembering, or applying information (see 11.00G3b(i)); or
3. Interacting with others (see 11.00G3b(ii)); or
4. Concentrating, persisting, or maintaining pace (see 11.00G3b(iii)); or
5. Adapting or managing oneself (see 11.00G3b(iv)).
11.03 [Reserved]
11.04 Vascular insult to the brain, characterized by A, B, or C:
A. Sensory or motor aphasia resulting in ineffective speech or communication (see 11.00E1) persisting for at least 3 consecutive months after the insult; or
B. Disorganization of motor function in two extremities (see 11.00D1), resulting in an extreme limitation (see 11.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities, persisting for at least 3 consecutive months after the insult; or
C. Marked limitation (see 11.00G2) in physical functioning (see 11.00G3a) and in one of the following areas of mental functioning, both persisting for at least 3 consecutive months after the insult:
1. Understanding, remembering, or applying information (see 11.00G3b(i)); or
2. Interacting with others (see 11.00G3b(ii)); or
3. Concentrating, persisting, or maintaining pace (see 11.00G3b(iii)); or
4. Adapting or managing oneself (see 11.00G3b(iv)).
11.05 Benign brain tumors, characterized by A or B:
A. Disorganization of motor function in two extremities (see 11.00D1), resulting in an extreme limitation (see 11.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities; or
B. Marked limitation (see 11.00G2) in physical functioning (see 11.00G3a), and in one of the following:
1. Understanding, remembering, or applying information (see 11.00G3b(i)); or
2. Interacting with others (see 11.00G3b(ii)); or
3. Concentrating, persisting, or maintaining pace (see 11.00G3b(iii)); or
4. Adapting or managing oneself (see 11.00G3b(iv)).
11.06 Parkinsonian syndrome, characterized by A or B despite adherence to prescribed treatment for at least 3 consecutive months (see 11.00C):
A. Disorganization of motor function in two extremities (see 11.00D1), resulting in an extreme limitation (see 11.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities; or
B. Marked limitation (see 11.00G2) in physical functioning (see 11.00G3a), and in one of the following:
1. Understanding, remembering, or applying information (see 11.00G3b(i)); or
2. Interacting with others (see 11.00G3b(ii)); or
3. Concentrating, persisting, or maintaining pace (see 11.00G3b(iii)); or
4. Adapting or managing oneself (see 11.00G3b(iv)).
11.07 Cerebral palsy, characterized by A, B, or C:
A. Disorganization of motor function in two extremities (see 11.00D1), resulting in an extreme limitation (see 11.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities; or
B. Marked limitation (see 11.00G2) in physical functioning (see 11.00G3a), and in one of the following:
1. Understanding, remembering, or applying information (see 11.00G3b(i)); or
2. Interacting with others (see 11.00G3b(ii)); or
3. Concentrating, persisting, or maintaining pace (see 11.00G3b(iii)); or
4. Adapting or managing oneself (see 11.00G3b(iv)); or
C. Significant interference in communication due to speech, hearing, or visual deficit (see 11.00E2).
11.08 Spinal cord disorders, characterized by A, B, or C:
A. Complete loss of function, as described in 11.00M2, persisting for 3 consecutive months after the disorder (see 11.00M4); or
B. Disorganization of motor function in two extremities (see 11.00D1), resulting in an extreme limitation (see 11.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities persisting for 3 consecutive months after the disorder (see 11.00M4); or
C. Marked limitation (see 11.00G2) in physical functioning (see 11.00G3a) and in one of the following areas of mental functioning, both persisting for 3 consecutive months after the disorder (see 11.00M4):
1. Understanding, remembering, or applying information (see 11.00G3b(i)); or
2. Interacting with others (see 11.00G3b(ii)); or
3. Concentrating, persisting, or maintaining pace (see 11.00G3b(iii)); or
4. Adapting or managing oneself (see 11.00G3b(iv)).
11.09 Multiple sclerosis, characterized by A or B:
A. Disorganization of motor function in two extremities (see 11.00D1), resulting in an extreme limitation (see 11.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities; or
B. Marked limitation (see 11.00G2) in physical functioning (see 11.00G3a), and in one of the following:
1. Understanding, remembering, or applying information (see 11.00G3b(i)); or
2. Interacting with others (see 11.00G3b(ii)); or
3. Concentrating, persisting, or maintaining pace (see 11.00G3b(iii)); or
4. Adapting or managing oneself (see 11.00G3b(iv)).
11.10 Amyotrophic lateral sclerosis (ALS) established by clinical and laboratory findings (see 11.00O).
11.11 Post-polio syndrome, characterized by A, B, C, or D:
A. Disorganization of motor function in two extremities (see 11.00D1), resulting in an extreme limitation (see 11.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities; or
B. Unintelligible speech (see 11.00E3); or
C. Bulbar and neuromuscular dysfunction (see 11.00F), resulting in:
1. Acute respiratory failure requiring mechanical ventilation; or
2. Need for supplemental enteral nutrition via a gastrostomy or parenteral nutrition via a central venous catheter; or
D. Marked limitation (see 11.00G2) in physical functioning (see 11.00G3a), and in one of the following:
1. Understanding, remembering, or applying information (see 11.00G3b(i)); or
2. Interacting with others (see 11.00G3b(ii)); or
3. Concentrating, persisting, or maintaining pace (see 11.00G3b(iii)); or
4. Adapting or managing oneself (see 11.00G3b(iv)).
11.12 Myasthenia gravis, characterized by A, B, or C despite adherence to prescribed treatment for at least 3 months (see 11.00C):
A. Disorganization of motor function in two extremities (see 11.00D1), resulting in an extreme limitation (see 11.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities; or
B. Bulbar and neuromuscular dysfunction (see 11.00F), resulting in:
1. One myasthenic crisis requiring mechanical ventilation; or
2. Need for supplemental enteral nutrition via a gastrostomy or parenteral nutrition via a central venous catheter; or
C. Marked limitation (see 11.00G2) in physical functioning (see 11.00G3a), and in one of the following:
1. Understanding, remembering, or applying information (see 11.00G3b(i)); or
2. Interacting with others (see 11.00G3b(ii)); or
3. Concentrating, persisting, or maintaining pace (see 11.00G3b(iii)); or
4. Adapting or managing oneself (see 11.00G3b(iv)).
11.13 Muscular dystrophy, characterized by A or B:
A. Disorganization of motor function in two extremities (see 11.00D1), resulting in an extreme limitation (see 11.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities; or
B. Marked limitation (see 11.00G2) in physical functioning (see 11.00G3a), and in one of the following:
1. Understanding, remembering, or applying information (see 11.00G3b(i)); or
2. Interacting with others (see 11.00G3b(ii)); or
3. Concentrating, persisting, or maintaining pace (see 11.00G3b(iii)); or
4. Adapting or managing oneself (see 11.00G3b(iv)).
11.14 Peripheral neuropathy, characterized by A or B:
A. Disorganization of motor function in two extremities (see 11.00D1), resulting in an extreme limitation (see 11.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities; or
B. Marked limitation (see 11.00G2) in physical functioning (see 11.00G3a), and in one of the following:
1. Understanding, remembering, or applying information (see 11.00G3b(i)); or
2. Interacting with others (see 11.00G3b(ii)); or
3. Concentrating, persisting, or maintaining pace (see 11.00G3b(iii)); or
4. Adapting or managing oneself (see 11.00G3b(iv)).
11.15 [Reserved]
11.16 [Reserved]
11.17 Neurodegenerative disorders of the central nervous system, such as Huntington's disease, Friedreich's ataxia, and spinocerebellar degeneration, characterized by A or B:
A. Disorganization of motor function in two extremities (see 11.00D1), resulting in an extreme limitation (see 11.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities; or
B. Marked limitation (see 11.00G2) in physical functioning (see 11.00G3a), and in one of the following:
1. Understanding, remembering, or applying information (see 11.00G3b(i)); or
2. Interacting with others (see 11.00G3b(ii)); or
3. Concentrating, persisting, or maintaining pace (see 11.00G3b(iii)); or
4. Adapting or managing oneself (see 11.00G3b(iv)).
11.18 Traumatic brain injury, characterized by A or B:
A. Disorganization of motor function in two extremities (see 11.00D1), resulting in an extreme limitation (see 11.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities, persisting for at least 3 consecutive months after the injury; or
B. Marked limitation (see 11.00G2) in physical functioning (see 11.00G3a), and in one of the following areas of mental functioning, persisting for at least 3 consecutive months after the injury:
1. Understanding, remembering, or applying information (see 11.00G3b(i)); or
2. Interacting with others (see 11.00G3b(ii)); or
3. Concentrating, persisting, or maintaining pace (see 11.00G3b(iii)); or
4. Adapting or managing oneself (see 11.00G3b(iv)).
11.19 [Reserved]
11.20 Coma or persistent vegetative state, persisting for at least 1 month.
11.21 [Reserved]
11.22 Motor neuron disorders other than ALS, characterized by A, B, or C:
A. Disorganization of motor function in two extremities (see 11.00D1), resulting in an extreme limitation (see 11.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities; or
B. Bulbar and neuromuscular dysfunction (see 11.00F), resulting in:
1. Acute respiratory failure requiring invasive mechanical ventilation; or
2. Need for supplemental enteral nutrition via a gastrostomy or parenteral nutrition via a central venous catheter; or
C. Marked limitation (see 11.00G2) in physical functioning (see 11.00G3a), and in one of the following:
1. Understanding, remembering, or applying information (see 11.00G3b(i)); or
2. Interacting with others (see 11.00G3b(ii)); or
3. Concentrating, persisting, or maintaining pace (see 11.00G3b(iii)); or
4. Adapting or managing oneself (see 11.00G3b(iv)).
12.00 Mental Disorders
A. How are the listings for mental disorders arranged, and what do they require?
1. The listings for mental disorders are arranged in 11 categories: Neurocognitive disorders (12.02); schizophrenia spectrum and other psychotic disorders (12.03); depressive, bipolar and related disorders (12.04); intellectual disorder (12.05); anxiety and obsessive-compulsive disorders (12.06); somatic symptom and related disorders (12.07); personality and impulse-control disorders (12.08); autism spectrum disorder (12.10); neurodevelopmental disorders (12.11); eating disorders (12.13); and trauma- and stressor-related disorders (12.15).
2. Listings 12.07, 12.08, 12.10, 12.11, and 12.13 have two paragraphs, designated A and B; your mental disorder must satisfy the requirements of both paragraphs A and B. Listings 12.02, 12.03, 12.04, 12.06, and 12.15 have three paragraphs, designated A, B, and C; your mental disorder must satisfy the requirements of both paragraphs A and B, or the requirements of both paragraphs A and C. Listing 12.05 has two paragraphs that are unique to that listing (see 12.00A3); your mental disorder must satisfy the requirements of either paragraph A or paragraph B.
a. Paragraph A of each listing (except 12.05) includes the medical criteria that must be present in your medical evidence.
b. Paragraph B of each listing (except 12.05) provides the functional criteria we assess, in conjunction with a rating scale (see 12.00E and 12.00F), to evaluate how your mental disorder limits your functioning. These criteria represent the areas of mental functioning a person uses in a work setting. They are: Understand, remember, or apply information; interact with others; concentrate, persist, or maintain pace; and adapt or manage oneself. We will determine the degree to which your medically determinable mental impairment affects the four areas of mental functioning and your ability to function independently, appropriately, effectively, and on a sustained basis (see §§ 404.1520a(c)(2) and 416.920a(c)(2) of this chapter). To satisfy the paragraph B criteria, your mental disorder must result in “extreme” limitation of one, or “marked” limitation of two, of the four areas of mental functioning. (When we refer to “paragraph B criteria” or “area[s] of mental functioning” in the introductory text of this body system, we mean the criteria in paragraph B of every listing except 12.05.)
c. Paragraph C of listings 12.02, 12.03, 12.04, 12.06, and 12.15 provides the criteria we use to evaluate “serious and persistent mental disorders.” To satisfy the paragraph C criteria, your mental disorder must be “serious and persistent”; that is, there must be a medically documented history of the existence of the disorder over a period of at least 2 years, and evidence that satisfies the criteria in both C1 and C2 (see 12.00G). (When we refer to “paragraph C” or “the paragraph C criteria” in the introductory text of this body system, we mean the criteria in paragraph C of listings 12.02, 12.03, 12.04, 12.06, and 12.15.)
3. Listing 12.05 has two paragraphs, designated A and B, that apply to only intellectual disorder. Each paragraph requires that you have significantly subaverage general intellectual functioning; significant deficits in current adaptive functioning; and evidence that demonstrates or supports (is consistent with) the conclusion that your disorder began prior to age 22.
B. Which mental disorders do we evaluate under each listing category?
1. Neurocognitive disorders (12.02).
a. These disorders are characterized by a clinically significant decline in cognitive functioning. Symptoms and signs may include, but are not limited to, disturbances in memory, executive functioning (that is, higher-level cognitive processes; for example, regulating attention, planning, inhibiting responses, decision-making), visual-spatial functioning, language and speech, perception, insight, judgment, and insensitivity to social standards.
b. Examples of disorders that we evaluate in this category include major neurocognitive disorder; dementia of the Alzheimer type; vascular dementia; dementia due to a medical condition such as a metabolic disease (for example, late-onset Tay-Sachs disease), human immunodeficiency virus infection, vascular malformation, progressive brain tumor, neurological disease (for example, multiple sclerosis, Parkinsonian syndrome, Huntington disease), or traumatic brain injury; or substance-induced cognitive disorder associated with drugs of abuse, medications, or toxins. (We evaluate neurological disorders under that body system (see 11.00). We evaluate cognitive impairments that result from neurological disorders under 12.02 if they do not satisfy the requirements in 11.00 (see 11.00G).)
c. This category does not include the mental disorders that we evaluate under intellectual disorder (12.05), autism spectrum disorder (12.10), and neurodevelopmental disorders (12.11).
2. Schizophrenia spectrum and other psychotic disorders (12.03).
a. These disorders are characterized by delusions, hallucinations, disorganized speech, or grossly disorganized or catatonic behavior, causing a clinically significant decline in functioning. Symptoms and signs may include, but are not limited to, inability to initiate and persist in goal-directed activities, social withdrawal, flat or inappropriate affect, poverty of thought and speech, loss of interest or pleasure, disturbances of mood, odd beliefs and mannerisms, and paranoia.
b. Examples of disorders that we evaluate in this category include schizophrenia, schizoaffective disorder, delusional disorder, and psychotic disorder due to another medical condition.
3. Depressive, bipolar and related disorders (12.04).
a. These disorders are characterized by an irritable, depressed, elevated, or expansive mood, or by a loss of interest or pleasure in all or almost all activities, causing a clinically significant decline in functioning. Symptoms and signs may include, but are not limited to, feelings of hopelessness or guilt, suicidal ideation, a clinically significant change in body weight or appetite, sleep disturbances, an increase or decrease in energy, psychomotor abnormalities, disturbed concentration, pressured speech, grandiosity, reduced impulse control, sadness, euphoria, and social withdrawal.
b. Examples of disorders that we evaluate in this category include bipolar disorders (I or II), cyclothymic disorder, major depressive disorder, persistent depressive disorder (dysthymia), and bipolar or depressive disorder due to another medical condition.
4. Intellectual disorder (12.05).
a. This disorder is characterized by significantly subaverage general intellectual functioning, significant deficits in current adaptive functioning, and manifestation of the disorder before age 22. Signs may include, but are not limited to, poor conceptual, social, or practical skills evident in your adaptive functioning.
b. The disorder that we evaluate in this category may be described in the evidence as intellectual disability, intellectual developmental disorder, or historically used terms such as “mental retardation.”
c. This category does not include the mental disorders that we evaluate under neurocognitive disorders (12.02), autism spectrum disorder (12.10), or neurodevelopmental disorders (12.11).
5. Anxiety and obsessive-compulsive disorders (12.06).
a. These disorders are characterized by excessive anxiety, worry, apprehension, and fear, or by avoidance of feelings, thoughts, activities, objects, places, or people. Symptoms and signs may include, but are not limited to, restlessness, difficulty concentrating, hyper-vigilance, muscle tension, sleep disturbance, fatigue, panic attacks, obsessions and compulsions, constant thoughts and fears about safety, and frequent physical complaints.
b. Examples of disorders that we evaluate in this category include social anxiety disorder, panic disorder, generalized anxiety disorder, agoraphobia, and obsessive-compulsive disorder.
c. This category does not include the mental disorders that we evaluate under trauma- and stressor-related disorders (12.15).
6. Somatic symptom and related disorders (12.07).
a. These disorders are characterized by physical symptoms or deficits that are not intentionally produced or feigned, and that, following clinical investigation, cannot be fully explained by a general medical condition, another mental disorder, the direct effects of a substance, or a culturally sanctioned behavior or experience. These disorders may also be characterized by a preoccupation with having or acquiring a serious medical condition that has not been identified or diagnosed. Symptoms and signs may include, but are not limited to, pain and other abnormalities of sensation, gastrointestinal symptoms, fatigue, a high level of anxiety about personal health status, abnormal motor movement, pseudoseizures, and pseudoneurological symptoms, such as blindness or deafness.
b. Examples of disorders that we evaluate in this category include somatic symptom disorder, illness anxiety disorder, and conversion disorder.
7. Personality and impulse-control disorders (12.08).
a. These disorders are characterized by enduring, inflexible, maladaptive, and pervasive patterns of behavior. Onset typically occurs in adolescence or young adulthood. Symptoms and signs may include, but are not limited to, patterns of distrust, suspiciousness, and odd beliefs; social detachment, discomfort, or avoidance; hypersensitivity to negative evaluation; an excessive need to be taken care of; difficulty making independent decisions; a preoccupation with orderliness, perfectionism, and control; and inappropriate, intense, impulsive anger and behavioral expression grossly out of proportion to any external provocation or psychosocial stressors.
b. Examples of disorders that we evaluate in this category include paranoid, schizoid, schizotypal, borderline, avoidant, dependent, obsessive-compulsive personality disorders, and intermittent explosive disorder.
8. Autism spectrum disorder (12.10).
a. These disorders are characterized by qualitative deficits in the development of reciprocal social interaction, verbal and nonverbal communication skills, and symbolic or imaginative activity; restricted repetitive and stereotyped patterns of behavior, interests, and activities; and stagnation of development or loss of acquired skills early in life. Symptoms and signs may include, but are not limited to, abnormalities and unevenness in the development of cognitive skills; unusual responses to sensory stimuli; and behavioral difficulties, including hyperactivity, short attention span, impulsivity, aggressiveness, or self-injurious actions.
b. Examples of disorders that we evaluate in this category include autism spectrum disorder with or without accompanying intellectual impairment, and autism spectrum disorder with or without accompanying language impairment.
c. This category does not include the mental disorders that we evaluate under neurocognitive disorders (12.02), intellectual disorder (12.05), and neurodevelopmental disorders (12.11).
9. Neurodevelopmental disorders (12.11).
a. These disorders are characterized by onset during the developmental period, that is, during childhood or adolescence, although sometimes they are not diagnosed until adulthood. Symptoms and signs may include, but are not limited to, underlying abnormalities in cognitive processing (for example, deficits in learning and applying verbal or nonverbal information, visual perception, memory, or a combination of these); deficits in attention or impulse control; low frustration tolerance; excessive or poorly planned motor activity; difficulty with organizing (time, space, materials, or tasks); repeated accidental injury; and deficits in social skills. Symptoms and signs specific to tic disorders include sudden, rapid, recurrent, non-rhythmic, motor movement or vocalization.
b. Examples of disorders that we evaluate in this category include specific learning disorder, borderline intellectual functioning, and tic disorders (such as Tourette syndrome).
c. This category does not include the mental disorders that we evaluate under neurocognitive disorders (12.02), autism spectrum disorder (12.10), or personality and impulse-control disorders (12.08).
10. Eating disorders (12.13).
a. These disorders are characterized by disturbances in eating behavior and preoccupation with, and excessive self-evaluation of, body weight and shape. Symptoms and signs may include, but are not limited to, restriction of energy consumption when compared with individual requirements; recurrent episodes of binge eating or behavior intended to prevent weight gain, such as self-induced vomiting, excessive exercise, or misuse of laxatives; mood disturbances, social withdrawal, or irritability; amenorrhea; dental problems; abnormal laboratory findings; and cardiac abnormalities.
b. Examples of disorders that we evaluate in this category include anorexia nervosa, bulimia nervosa, binge-eating disorder, and avoidant/restrictive food disorder.
11. Trauma- and stressor-related disorders (12.15).
a. These disorders are characterized by experiencing or witnessing a traumatic or stressful event, or learning of a traumatic event occurring to a close family member or close friend, and the psychological aftermath of clinically significant effects on functioning. Symptoms and signs may include, but are not limited to, distressing memories, dreams, and flashbacks related to the trauma or stressor; avoidant behavior; diminished interest or participation in significant activities; persistent negative emotional states (for example, fear, anger) or persistent inability to experience positive emotions (for example, satisfaction, affection); anxiety; irritability; aggression; exaggerated startle response; difficulty concentrating; and sleep disturbance.
b. Examples of disorders that we evaluate in this category include posttraumatic stress disorder and other specified trauma- and stressor-related disorders (such as adjustment-like disorders with prolonged duration without prolonged duration of stressor).
c. This category does not include the mental disorders that we evaluate under anxiety and obsessive-compulsive disorders (12.06), and cognitive impairments that result from neurological disorders, such as a traumatic brain injury, which we evaluate under neurocognitive disorders (12.02).
C. What evidence do we need to evaluate your mental disorder?
1. General. We need objective medical evidence from an acceptable medical source to establish that you have a medically determinable mental disorder. We also need evidence to assess the severity of your mental disorder and its effects on your ability to function in a work setting. We will determine the extent and kinds of evidence we need from medical and nonmedical sources based on the individual facts about your disorder. For additional evidence requirements for intellectual disorder (12.05), see 12.00H. For our basic rules on evidence, see §§ 404.1512, 404.1513, 404.1520b, 416.912, 416.913, and 416.920b of this chapter. For our rules on evaluating medical opinions, see §§ 404.1520c, 404.1527, 416.920c, and 416.927 of this chapter. For our rules on evidence about your symptoms, see §§ 404.1529 and 416.929 of this chapter.
2. Evidence from medical sources. We will consider all relevant medical evidence about your disorder from your physician, psychologist, and other medical sources, which include health care providers such as physician assistants, psychiatric nurse practitioners, licensed clinical social workers, and clinical mental health counselors. Evidence from your medical sources may include:
a. Your reported symptoms.
b. Your medical, psychiatric, and psychological history.
c. The results of physical or mental status examinations, structured clinical interviews, psychiatric or psychological rating scales, measures of adaptive functioning, or other clinical findings.
d. Psychological testing, imaging results, or other laboratory findings.
e. Your diagnosis.
f. The type, dosage, and beneficial effects of medications you take.
g. The type, frequency, duration, and beneficial effects of therapy you receive.
h. Side effects of medication or other treatment that limit your ability to function.
i. Your clinical course, including changes in your medication, therapy, or other treatment, and the time required for therapeutic effectiveness.
j. Observations and descriptions of how you function during examinations or therapy.
k. Information about sensory, motor, or speech abnormalities, or about your cultural background (for example, language or customs) that may affect an evaluation of your mental disorder.
l. The expected duration of your symptoms and signs and their effects on your functioning, both currently and in the future.
3. Evidence from you and people who know you. We will consider all relevant evidence about your mental disorder and your daily functioning that we receive from you and from people who know you. We will ask about your symptoms, your daily functioning, and your medical treatment. We will ask for information from third parties who can tell us about your mental disorder, but you must give us permission to do so. This evidence may include information from your family, caregivers, friends, neighbors, clergy, case managers, social workers, shelter staff, or other community support and outreach workers. We will consider whether your statements and the statements from third parties are consistent with the medical and other evidence we have.
4. Evidence from school, vocational training, work, and work-related programs.
a. School. You may have recently attended or may still be attending school, and you may have received or may still be receiving special education services. If so, we will try to obtain information from your school sources when we need it to assess how your mental disorder affects your ability to function. Examples of this information include your Individualized Education Programs (IEPs), your Section 504 plans, comprehensive evaluation reports, school-related therapy progress notes, information from your teachers about how you function in a classroom setting, and information about any special services or accommodations you receive at school.
b. Vocational training, work, and work-related programs. You may have recently participated in or may still be participating in vocational training, work-related programs, or work activity. If so, we will try to obtain information from your training program or your employer when we need it to assess how your mental disorder affects your ability to function. Examples of this information include training or work evaluations, modifications to your work duties or work schedule, and any special supports or accommodations you have required or now require in order to work. If you have worked or are working through a community mental health program, sheltered or supported work program, rehabilitation program, or transitional employment program, we will consider the type and degree of support you have received or are receiving in order to work (see 12.00D).
5. Need for longitudinal evidence.
a. General. Longitudinal medical evidence can help us learn how you function over time, and help us evaluate any variations in the level of your functioning. We will request longitudinal evidence of your mental disorder when your medical providers have records concerning you and your mental disorder over a period of months or perhaps years (see §§ 404.1512(d) and 416.912(d) of this chapter).
b. Non-medical sources of longitudinal evidence. Certain situations, such as chronic homelessness, may make it difficult for you to provide longitudinal medical evidence. If you have a severe mental disorder, you will probably have evidence of its effects on your functioning over time, even if you have not had an ongoing relationship with the medical community or are not currently receiving treatment. For example, family members, friends, neighbors, former employers, social workers, case managers, community support staff, outreach workers, or government agencies may be familiar with your mental health history. We will ask for information from third parties who can tell us about your mental disorder, but you must give us permission to do so.
c. Absence of longitudinal evidence. In the absence of longitudinal evidence, we will use current objective medical evidence and all other relevant evidence available to us in your case record to evaluate your mental disorder. If we purchase a consultative examination to document your disorder, the record will include the results of that examination (see §§ 404.1514 and 416.914 of this chapter). We will take into consideration your medical history, symptoms, clinical and laboratory findings, and medical source opinions. If you do not have longitudinal evidence, the current evidence alone may not be sufficient or appropriate to show that you have a disorder that meets the criteria of one of the mental disorders listings. In that case, we will follow the rules in 12.00J.
6. Evidence of functioning in unfamiliar situations or supportive situations.
a. Unfamiliar situations. We recognize that evidence about your functioning in unfamiliar situations does not necessarily show how you would function on a sustained basis in a work setting. In one-time, time-limited, or other unfamiliar situations, you may function differently than you do in familiar situations. In unfamiliar situations, you may appear more, or less, limited than you do on a daily basis and over time.
b. Supportive situations. Your ability to complete tasks in settings that are highly structured, or that are less demanding or more supportive than typical work settings does not necessarily demonstrate your ability to complete tasks in the context of regular employment during a normal workday or work week.
c. Our assessment. We must assess your ability to complete tasks by evaluating all the evidence, such as reports about your functioning from you and third parties who are familiar with you, with an emphasis on how independently, appropriately, and effectively you are able to complete tasks on a sustained basis.
D. How do we consider psychosocial supports, structured settings, living arrangements, and treatment?
1. General. Psychosocial supports, structured settings, and living arrangements, including assistance from your family or others, may help you by reducing the demands made on you. In addition, treatment you receive may reduce your symptoms and signs and possibly improve your functioning, or may have side effects that limit your functioning. Therefore, when we evaluate the effects of your mental disorder and rate the limitation of your areas of mental functioning, we will consider the kind and extent of supports you receive, the characteristics of any structured setting in which you spend your time, and the effects of any treatment. This evidence may come from reports about your functioning from you or third parties who are familiar with you, and other third-party statements or information. Following are some examples of the supports you may receive:
a. You receive help from family members or other people who monitor your daily activities and help you to function. For example, family members administer your medications, remind you to eat, shop for you and pay your bills, or change their work hours so you are never home alone.
b. You participate in a special education or vocational training program, or a psychosocial rehabilitation day treatment or community support program, where you receive training in daily living and entry-level work skills.
c. You participate in a sheltered, supported, or transitional work program, or in a competitive employment setting with the help of a job coach or supervisor.
d. You receive comprehensive “24/7 wrap-around” mental health services while living in a group home or transitional housing, while participating in a semi-independent living program, or while living in individual housing (for example, your own home or apartment).
e. You live in a hospital or other institution with 24-hour care.
f. You receive assistance from a crisis response team, social workers, or community mental health workers who help you meet your physical needs, and who may also represent you in dealings with government or community social services.
g. You live alone and do not receive any psychosocial support(s); however, you have created a highly structured environment by eliminating all but minimally necessary contact with the world outside your living space.
2. How we consider different levels of support and structure in psychosocial rehabilitation programs.
a. Psychosocial rehabilitation programs are based on your specific needs. Therefore, we cannot make any assumptions about your mental disorder based solely on the fact that you are associated with such a program. We must know the details of the program(s) in which you are involved and the pattern(s) of your involvement over time.
b. The kinds and levels of supports and structures in psychosocial rehabilitation programs typically occur on a scale of “most restrictive” to “least restrictive.” Participation in a psychosocial rehabilitation program at the most restrictive level would suggest greater limitation of your areas of mental functioning than would participation at a less restrictive level. The length of time you spend at different levels in a program also provides information about your functioning. For example, you could begin participation at the most restrictive crisis intervention level but gradually improve to the point of readiness for a lesser level of support and structure and possibly some form of employment.
3. How we consider the help or support you receive.
a. We will consider the complete picture of your daily functioning, including the kinds, extent, and frequency of help and support you receive, when we evaluate your mental disorder and determine whether you are able to use the four areas of mental functioning in a work setting. The fact that you have done, or currently do, some routine activities without help or support does not necessarily mean that you do not have a mental disorder or that you are not disabled. For example, you may be able to take care of your personal needs, cook, shop, pay your bills, live by yourself, and drive a car. You may demonstrate both strengths and deficits in your daily functioning.
b. You may receive various kinds of help and support from others that enable you to do many things that, because of your mental disorder, you might not be able to do independently. Your daily functioning may depend on the special contexts in which you function. For example, you may spend your time among only familiar people or surroundings, in a simple and steady routine or an unchanging environment, or in a highly structured setting. However, this does not necessarily show how you would function in a work setting on a sustained basis, throughout a normal workday and workweek. (See 12.00H for further discussion of these issues regarding significant deficits in adaptive functioning for the purpose of 12.05.)
4. How we consider treatment. We will consider the effect of any treatment on your functioning when we evaluate your mental disorder. Treatment may include medication(s), psychotherapy, or other forms of intervention, which you receive in a doctor's office, during a hospitalization, or in a day program at a hospital or outpatient treatment program. With treatment, you may not only have your symptoms and signs reduced, but may also be able to function in a work setting. However, treatment may not resolve all of the limitations that result from your mental disorder, and the medications you take or other treatment you receive for your disorder may cause side effects that limit your mental or physical functioning. For example, you may experience drowsiness, blunted affect, memory loss, or abnormal involuntary movements.
E. What are the paragraph B criteria?
1. Understand, remember, or apply information (paragraph B1). This area of mental functioning refers to the abilities to learn, recall, and use information to perform work activities. Examples include: Understanding and learning terms, instructions, procedures; following one- or two-step oral instructions to carry out a task; describing work activity to someone else; asking and answering questions and providing explanations; recognizing a mistake and correcting it; identifying and solving problems; sequencing multi-step activities; and using reason and judgment to make work-related decisions. These examples illustrate the nature of this area of mental functioning. We do not require documentation of all of the examples.
2. Interact with others (paragraph B2). This area of mental functioning refers to the abilities to relate to and work with supervisors, co-workers, and the public. Examples include: cooperating with others; asking for help when needed; handling conflicts with others; stating own point of view; initiating or sustaining conversation; understanding and responding to social cues (physical, verbal, emotional); responding to requests, suggestions, criticism, correction, and challenges; and keeping social interactions free of excessive irritability, sensitivity, argumentativeness, or suspiciousness. These examples illustrate the nature of this area of mental functioning. We do not require documentation of all of the examples.
3. Concentrate, persist, or maintain pace (paragraph B3). This area of mental functioning refers to the abilities to focus attention on work activities and stay on task at a sustained rate. Examples include: Initiating and performing a task that you understand and know how to do; working at an appropriate and consistent pace; completing tasks in a timely manner; ignoring or avoiding distractions while working; changing activities or work settings without being disruptive; working close to or with others without interrupting or distracting them; sustaining an ordinary routine and regular attendance at work; and working a full day without needing more than the allotted number or length of rest periods during the day. These examples illustrate the nature of this area of mental functioning. We do not require documentation of all of the examples.
4. Adapt or manage oneself (paragraph B4). This area of mental functioning refers to the abilities to regulate emotions, control behavior, and maintain well-being in a work setting. Examples include: Responding to demands; adapting to changes; managing your psychologically based symptoms; distinguishing between acceptable and unacceptable work performance; setting realistic goals; making plans for yourself independently of others; maintaining personal hygiene and attire appropriate to a work setting; and being aware of normal hazards and taking appropriate precautions. These examples illustrate the nature of this area of mental functioning. We do not require documentation of all of the examples.
F. How do we use the paragraph B criteria to evaluate your mental disorder?
1. General. We use the paragraph B criteria, in conjunction with a rating scale (see 12.00F2), to rate the degree of your limitations. We consider only the limitations that result from your mental disorder(s). We will determine whether you are able to use each of the paragraph B areas of mental functioning in a work setting. We will consider, for example, the kind, degree, and frequency of difficulty you would have; whether you could function without extra help, structure, or supervision; and whether you would require special conditions with regard to activities or other people (see 12.00D).
2. The five-point rating scale. We evaluate the effects of your mental disorder on each of the four areas of mental functioning based on a five-point rating scale consisting of none, mild, moderate, marked, and extreme limitation. To satisfy the paragraph B criteria, your mental disorder must result in extreme limitation of one, or marked limitation of two, paragraph B areas of mental functioning. Under these listings, the five rating points are defined as follows:
a. No limitation (or none). You are able to function in this area independently, appropriately, effectively, and on a sustained basis.
b. Mild limitation. Your functioning in this area independently, appropriately, effectively, and on a sustained basis is slightly limited.
c. Moderate limitation. Your functioning in this area independently, appropriately, effectively, and on a sustained basis is fair.
d. Marked limitation. Your functioning in this area independently, appropriately, effectively, and on a sustained basis is seriously limited.
e. Extreme limitation. You are not able to function in this area independently, appropriately, effectively, and on a sustained basis.
3. Rating the limitations of your areas of mental functioning.
a. General. We use all of the relevant medical and non-medical evidence in your case record to evaluate your mental disorder: The symptoms and signs of your disorder, the reported limitations in your activities, and any help and support you receive that is necessary for you to function. The medical evidence may include descriptors regarding the diagnostic stage or level of your disorder, such as “mild” or “moderate.” Clinicians may use these terms to characterize your medical condition. However, these terms will not always be the same as the degree of your limitation in a paragraph B area of mental functioning.
b. Areas of mental functioning in daily activities. You use the same four areas of mental functioning in daily activities at home and in the community that you would use to function at work. With respect to a particular task or activity, you may have trouble using one or more of the areas. For example, you may have difficulty understanding and remembering what to do; or concentrating and staying on task long enough to do it; or engaging in the task or activity with other people; or trying to do the task without becoming frustrated and losing self-control. Information about your daily functioning can help us understand whether your mental disorder limits one or more of these areas; and, if so, whether it also affects your ability to function in a work setting.
c. Areas of mental functioning in work settings. If you have difficulty using an area of mental functioning from day-to-day at home or in your community, you may also have difficulty using that area to function in a work setting. On the other hand, if you are able to use an area of mental functioning at home or in your community, we will not necessarily assume that you would also be able to use that area to function in a work setting where the demands and stressors differ from those at home. We will consider all evidence about your mental disorder and daily functioning before we reach a conclusion about your ability to work.
d. Overall effect of limitations. Limitation of an area of mental functioning reflects the overall degree to which your mental disorder interferes with that area. The degree of limitation is how we document our assessment of your limitation when using the area of mental functioning independently, appropriately, effectively, and on a sustained basis. It does not necessarily reflect a specific type or number of activities, including activities of daily living, that you have difficulty doing. In addition, no single piece of information (including test results) can establish the degree of limitation of an area of mental functioning.
e. Effects of support, supervision, structure on functioning. The degree of limitation of an area of mental functioning also reflects the kind and extent of supports or supervision you receive and the characteristics of any structured setting where you spend your time, which enable you to function. The more extensive the support you need from others or the more structured the setting you need in order to function, the more limited we will find you to be (see 12.00D).
f. Specific instructions for paragraphs B1, B3, and B4. For paragraphs B1, B3, and B4, the greatest degree of limitation of any part of the area of mental functioning directs the rating of limitation of that whole area of mental functioning.
(i) To do a work-related task, you must be able to understand and remember and apply information required by the task. Similarly, you must be able to concentrate and persist and maintain pace in order to complete the task, and adapt and manage yourself in the workplace. Limitation in any one of these parts (understand or remember or apply; concentrate or persist or maintain pace; adapt or manage oneself) may prevent you from completing a work-related task.
(ii) We will document the rating of limitation of the whole area of mental functioning, not each individual part. We will not add ratings of the parts together. For example, with respect to paragraph B3, if you have marked limitation in maintaining pace, and mild or moderate limitations in concentrating and persisting, we will find that you have marked limitation in the whole paragraph B3 area of mental functioning.
(iii) Marked limitation in more than one part of the same paragraph B area of mental functioning does not satisfy the requirement to have marked limitation in two paragraph B areas of mental functioning.
4. How we evaluate mental disorders involving exacerbations and remissions.
a. When we evaluate the effects of your mental disorder, we will consider how often you have exacerbations and remissions, how long they last, what causes your mental disorder to worsen or improve, and any other relevant information. We will assess any limitation of the affected paragraph B area(s) of mental functioning using the rating scale for the paragraph B criteria. We will consider whether you can use the area of mental functioning on a regular and continuing basis (8 hours a day, 5 days a week, or an equivalent work schedule). We will not find that you are able to work solely because you have a period(s) of improvement (remission), or that you are disabled solely because you have a period of worsening (exacerbation), of your mental disorder.
b. If you have a mental disorder involving exacerbations and remissions, you may be able to use the four areas of mental functioning to work for a few weeks or months. Recurrence or worsening of symptoms and signs, however, can interfere enough to render you unable to sustain the work.
G. What are the paragraph C criteria, and how do we use them to evaluate your mental disorder?
1. General. The paragraph C criteria are an alternative to the paragraph B criteria under listings 12.02, 12.03, 12.04, 12.06, and 12.15. We use the paragraph C criteria to evaluate mental disorders that are “serious and persistent.” In the paragraph C criteria, we recognize that mental health interventions may control the more obvious symptoms and signs of your mental disorder.
2. Paragraph C criteria.
a. We find a mental disorder to be “serious and persistent” when there is a medically documented history of the existence of the mental disorder in the listing category over a period of at least 2 years, and evidence shows that your disorder satisfies both C1 and C2.
b. The criterion in C1 is satisfied when the evidence shows that you rely, on an ongoing basis, upon medical treatment, mental health therapy, psychosocial support(s), or a highly structured setting(s), to diminish the symptoms and signs of your mental disorder (see 12.00D). We consider that you receive ongoing medical treatment when the medical evidence establishes that you obtain medical treatment with a frequency consistent with accepted medical practice for the type of treatment or evaluation required for your medical condition. We will consider periods of inconsistent treatment or lack of compliance with treatment that may result from your mental disorder. If the evidence indicates that the inconsistent treatment or lack of compliance is a feature of your mental disorder, and it has led to an exacerbation of your symptoms and signs, we will not use it as evidence to support a finding that you have not received ongoing medical treatment as required by this paragraph.
c. The criterion in C2 is satisfied when the evidence shows that, despite your diminished symptoms and signs, you have achieved only marginal adjustment. “Marginal adjustment” means that your adaptation to the requirements of daily life is fragile; that is, you have minimal capacity to adapt to changes in your environment or to demands that are not already part of your daily life. We will consider that you have achieved only marginal adjustment when the evidence shows that changes or increased demands have led to exacerbation of your symptoms and signs and to deterioration in your functioning; for example, you have become unable to function outside of your home or a more restrictive setting, without substantial psychosocial supports (see 12.00D). Such deterioration may have necessitated a significant change in medication or other treatment. Similarly, because of the nature of your mental disorder, evidence may document episodes of deterioration that have required you to be hospitalized or absent from work, making it difficult for you to sustain work activity over time.
H. How do we document and evaluate intellectual disorder under 12.05?
1. General. Listing 12.05 is based on the three elements that characterize intellectual disorder: Significantly subaverage general intellectual functioning; significant deficits in current adaptive functioning; and the disorder manifested before age 22.
2. Establishing significantly subaverage general intellectual functioning.
a. Definition. Intellectual functioning refers to the general mental capacity to learn, reason, plan, solve problems, and perform other cognitive functions. Under 12.05A, we identify significantly subaverage general intellectual functioning by the cognitive inability to function at a level required to participate in standardized intelligence testing. Our findings under 12.05A are based on evidence from an acceptable medical source. Under 12.05B, we identify significantly subaverage general intellectual functioning by an IQ score(s) on an individually administered standardized test of general intelligence that meets program requirements and has a mean of 100 and a standard deviation of 15. A qualified specialist (see 12.00H2c) must administer the standardized intelligence testing.
b. Psychometric standards. We will find standardized intelligence test results usable for the purposes of 12.05B1 when the measure employed meets contemporary psychometric standards for validity, reliability, normative data, and scope of measurement; and a qualified specialist has individually administered the test according to all pre-requisite testing conditions.
c. Qualified specialist. A “qualified specialist” is currently licensed or certified at the independent level of practice in the State where the test was performed, and has the training and experience to administer, score, and interpret intelligence tests. If a psychological assistant or paraprofessional administered the test, a supervisory qualified specialist must interpret the test findings and co-sign the examination report.
d. Responsibility for conclusions based on testing. We generally presume that your obtained IQ score(s) is an accurate reflection of your general intellectual functioning, unless evidence in the record suggests otherwise. Examples of this evidence include: a statement from the test administrator indicating that your obtained score is not an accurate reflection of your general intellectual functioning, prior or internally inconsistent IQ scores, or information about your daily functioning. Only qualified specialists, Federal and State agency medical and psychological consultants, and other contracted medical and psychological experts may conclude that your obtained IQ score(s) is not an accurate reflection of your general intellectual functioning. This conclusion must be well supported by appropriate clinical and laboratory diagnostic techniques and must be based on relevant evidence in the case record, such as:
(i) The data obtained in testing;
(ii) Your developmental history, including when your signs and symptoms began;
(iii) Information about how you function on a daily basis in a variety of settings; and
(iv) Clinical observations made during the testing period, such as your ability to sustain attention, concentration, and effort; to relate appropriately to the examiner; and to perform tasks independently without prompts or reminders.
3. Establishing significant deficits in adaptive functioning.
a. Definition. Adaptive functioning refers to how you learn and use conceptual, social, and practical skills in dealing with common life demands. It is your typical functioning at home and in the community, alone or among others. Under 12.05A, we identify significant deficits in adaptive functioning based on your dependence on others to care for your personal needs, such as eating and bathing. We will base our conclusions about your adaptive functioning on evidence from a variety of sources (see 12.00H3b) and not on your statements alone. Under 12.05B2, we identify significant deficits in adaptive functioning based on whether there is extreme limitation of one, or marked limitation of two, of the paragraph B criteria (see 12.00E; 12.00F).
b. Evidence. Evidence about your adaptive functioning may come from:
(i) Medical sources, including their clinical observations;
(ii) Standardized tests of adaptive functioning (see 12.00H3c);
(iii) Third party information, such as a report of your functioning from a family member or friend;
(iv) School records, if you were in school recently;
(v) Reports from employers or supervisors; and
(vi) Your own statements about how you handle all of your daily activities.
c. Standardized tests of adaptive functioning. We do not require the results of an individually administered standardized test of adaptive functioning. If your case record includes these test results, we will consider the results along with all other relevant evidence; however, we will use the guidelines in 12.00E and F to evaluate and determine the degree of your deficits in adaptive functioning, as required under 12.05B2.
d. How we consider common everyday activities.
(i) The fact that you engage in common everyday activities, such as caring for your personal needs, preparing simple meals, or driving a car, will not always mean that you do not have deficits in adaptive functioning as required by 12.05B2. You may demonstrate both strengths and deficits in your adaptive functioning. However, a lack of deficits in one area does not negate the presence of deficits in another area. When we assess your adaptive functioning, we will consider all of your activities and your performance of them.
(ii) Our conclusions about your adaptive functioning rest on whether you do your daily activities independently, appropriately, effectively, and on a sustained basis. If you receive help in performing your activities, we need to know the kind, extent, and frequency of help you receive in order to perform them. We will not assume that your ability to do some common everyday activities, or to do some things without help or support, demonstrates that your mental disorder does not meet the requirements of 12.05B2. (See 12.00D regarding the factors we consider when we evaluate your functioning, including how we consider any help or support you receive.)
e. How we consider work activity. The fact that you have engaged in work activity, or that you work intermittently or steadily in a job commensurate with your abilities, will not always mean that you do not have deficits in adaptive functioning as required by 12.05B2. When you have engaged in work activity, we need complete information about the work, and about your functioning in the work activity and work setting, before we reach any conclusions about your adaptive functioning. We will consider all factors involved in your work history before concluding whether your impairment satisfies the criteria for intellectual disorder under 12.05B. We will consider your prior and current work history, if any, and various other factors influencing how you function. For example, we consider whether the work was in a supported setting, whether you required more supervision than other employees, how your job duties compared to others in the same job, how much time it took you to learn the job duties, and the reason the work ended, if applicable.
4. Establishing that the disorder began before age 22. We require evidence that demonstrates or supports (is consistent with) the conclusion that your mental disorder began prior to age 22. We do not require evidence that your impairment met all of the requirements of 12.05A or 12.05B prior to age 22. Also, we do not require you to have met our statutory definition of disability prior to age 22. When we do not have evidence that was recorded before you attained age 22, we need evidence about your current intellectual and adaptive functioning and the history of your disorder that supports the conclusion that the disorder began before you attained age 22. Examples of evidence that can demonstrate or support this conclusion include:
a. Tests of intelligence or adaptive functioning;
b. School records indicating a history of special education services based on your intellectual functioning;
c. An Individualized Education Program (IEP), including your transition plan;
d. Reports of your academic performance and functioning at school;
e. Medical treatment records;
f. Interviews or reports from employers;
g. Statements from a supervisor in a group home or a sheltered workshop; and
h. Statements from people who have known you and can tell us about your functioning in the past and currently.
I. How do we evaluate substance use disorders? If we find that you are disabled and there is medical evidence in your case record establishing that you have a substance use disorder, we will determine whether your substance use disorder is a contributing factor material to the determination of disability (see §§ 404.1535 and 416.935 of this chapter).
J. How do we evaluate mental disorders that do not meet one of the mental disorders listings?
1. These listings include only examples of mental disorders that we consider serious enough to prevent you from doing any gainful activity. If your severe mental disorder does not meet the criteria of any of these listings, we will consider whether you have an impairment(s) that meets the criteria of a listing in another body system. You may have another impairment(s) that is secondary to your mental disorder. For example, if you have an eating disorder and develop a cardiovascular impairment because of it, we will evaluate your cardiovascular impairment under the listings for the cardiovascular body system.
2. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing (see §§ 404.1526 and 416.926 of this chapter).
3. If your impairment(s) does not meet or medically equal a listing, we will assess your residual functional capacity for engaging in substantial gainful activity (see §§ 404.1545 and 416.945 of this chapter). When we assess your residual functional capacity, we consider all of your impairment-related mental and physical limitations. For example, the side effects of some medications may reduce your general alertness, concentration, or physical stamina, affecting your residual functional capacity for non-exertional or exertional work activities. Once we have determined your residual functional capacity, we proceed to the fourth, and if necessary, the fifth steps of the sequential evaluation process in §§ 404.1520 and 416.920 of this chapter. We use the rules in §§ 404.1594 and 416.994 of this chapter, as appropriate, when we decide whether you continue to be disabled.
12.01 Category of Impairments, Mental Disorders
12.02 Neurocognitive disorders (see 12.00B1), satisfied by A and B, or A and C:
A. Medical documentation of a significant cognitive decline from a prior level of functioning in one or more of the cognitive areas:
1. Complex attention;
2. Executive function;
3. Learning and memory;
4. Language;
5. Perceptual-motor; or
6. Social cognition.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 12.00F):
1. Understand, remember, or apply information (see 12.00E1).
2. Interact with others (see 12.00E2).
3. Concentrate, persist, or maintain pace (see 12.00E3).
4. Adapt or manage oneself (see 12.00E4).
OR
C. Your mental disorder in this listing category is “serious and persistent;” that is, you have a medically documented history of the existence of the disorder over a period of at least 2 years, and there is evidence of both:
1. Medical treatment, mental health therapy, psychosocial support(s), or a highly structured setting(s) that is ongoing and that diminishes the symptoms and signs of your mental disorder (see 12.00G2b); and
2. Marginal adjustment, that is, you have minimal capacity to adapt to changes in your environment or to demands that are not already part of your daily life (see 12.00G2c).
12.03 Schizophrenia spectrum and other psychotic disorders (see 12.00B2), satisfied by A and B, or A and C:
A. Medical documentation of one or more of the following:
1. Delusions or hallucinations;
2. Disorganized thinking (speech); or
3. Grossly disorganized behavior or catatonia.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 12.00F):
1. Understand, remember, or apply information (see 12.00E1).
2. Interact with others (see 12.00E2).
3. Concentrate, persist, or maintain pace (see 12.00E3).
4. Adapt or manage oneself (see 12.00E4).
OR
C. Your mental disorder in this listing category is “serious and persistent;” that is, you have a medically documented history of the existence of the disorder over a period of at least 2 years, and there is evidence of both:
1. Medical treatment, mental health therapy, psychosocial support(s), or a highly structured setting(s) that is ongoing and that diminishes the symptoms and signs of your mental disorder (see 12.00G2b); and
2. Marginal adjustment, that is, you have minimal capacity to adapt to changes in your environment or to demands that are not already part of your daily life (see 12.00G2c).
12.04 Depressive, bipolar and related disorders (see 12.00B3), satisfied by A and B, or A and C:
A. Medical documentation of the requirements of paragraph 1 or 2:
1. Depressive disorder, characterized by five or more of the following:
a. Depressed mood;
b. Diminished interest in almost all activities;
c. Appetite disturbance with change in weight;
d. Sleep disturbance;
e. Observable psychomotor agitation or retardation;
f. Decreased energy;
g. Feelings of guilt or worthlessness;
h. Difficulty concentrating or thinking; or
i. Thoughts of death or suicide.
2. Bipolar disorder, characterized by three or more of the following:
a. Pressured speech;
b. Flight of ideas;
c. Inflated self-esteem;
d. Decreased need for sleep;
e. Distractibility;
f. Involvement in activities that have a high probability of painful consequences that are not recognized; or
g. Increase in goal-directed activity or psychomotor agitation.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 12.00F):
1. Understand, remember, or apply information (see 12.00E1).
2. Interact with others (see 12.00E2).
3. Concentrate, persist, or maintain pace (see 12.00E3).
4. Adapt or manage oneself (see 12.00E4).
OR
C. Your mental disorder in this listing category is “serious and persistent;” that is, you have a medically documented history of the existence of the disorder over a period of at least 2 years, and there is evidence of both:
1. Medical treatment, mental health therapy, psychosocial support(s), or a highly structured setting(s) that is ongoing and that diminishes the symptoms and signs of your mental disorder (see 12.00G2b); and
2. Marginal adjustment, that is, you have minimal capacity to adapt to changes in your environment or to demands that are not already part of your daily life (see 12.00G2c).
12.05 Intellectual disorder (see 12.00B4), satisfied by A or B:
A. Satisfied by 1, 2, and 3 (see 12.00H):
1. Significantly subaverage general intellectual functioning evident in your cognitive inability to function at a level required to participate in standardized testing of intellectual functioning; and
2. Significant deficits in adaptive functioning currently manifested by your dependence upon others for personal needs (for example, toileting, eating, dressing, or bathing); and
3. The evidence about your current intellectual and adaptive functioning and about the history of your disorder demonstrates or supports the conclusion that the disorder began prior to your attainment of age 22.
OR
B. Satisfied by 1, 2, and 3 (see 12.00H):
1. Significantly subaverage general intellectual functioning evidenced by a or b:
a. A full scale (or comparable) IQ score of 70 or below on an individually administered standardized test of general intelligence; or
b. A full scale (or comparable) IQ score of 71-75 accompanied by a verbal or performance IQ score (or comparable part score) of 70 or below on an individually administered standardized test of general intelligence; and
2. Significant deficits in adaptive functioning currently manifested by extreme limitation of one, or marked limitation of two, of the following areas of mental functioning:
a. Understand, remember, or apply information (see 12.00E1); or
b. Interact with others (see 12.00E2); or
c. Concentrate, persist, or maintain pace (see 12.00E3); or
d. Adapt or manage oneself (see 12.00E4); and
3. The evidence about your current intellectual and adaptive functioning and about the history of your disorder demonstrates or supports the conclusion that the disorder began prior to your attainment of age 22.
12.06 Anxiety and obsessive-compulsive disorders (see 12.00B5), satisfied by A and B, or A and C:
A. Medical documentation of the requirements of paragraph 1, 2, or 3:
1. Anxiety disorder, characterized by three or more of the following;
a. Restlessness;
b. Easily fatigued;
c. Difficulty concentrating;
d. Irritability;
e. Muscle tension; or
f. Sleep disturbance.
2. Panic disorder or agoraphobia, characterized by one or both:
a. Panic attacks followed by a persistent concern or worry about additional panic attacks or their consequences; or
b. Disproportionate fear or anxiety about at least two different situations (for example, using public transportation, being in a crowd, being in a line, being outside of your home, being in open spaces).
3. Obsessive-compulsive disorder, characterized by one or both:
a. Involuntary, time-consuming preoccupation with intrusive, unwanted thoughts; or
b. Repetitive behaviors aimed at reducing anxiety.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 12.00F):
1. Understand, remember, or apply information (see 12.00E1).
2. Interact with others (see 12.00E2).
3. Concentrate, persist, or maintain pace (see 12.00E3).
4. Adapt or manage oneself (see 12.00E4).
OR
C. Your mental disorder in this listing category is “serious and persistent;” that is, you have a medically documented history of the existence of the disorder over a period of at least 2 years, and there is evidence of both:
1. Medical treatment, mental health therapy, psychosocial support(s), or a highly structured setting(s) that is ongoing and that diminishes the symptoms and signs of your mental disorder (see 12.00G2b); and
2. Marginal adjustment, that is, you have minimal capacity to adapt to changes in your environment or to demands that are not already part of your daily life (see 12.00G2c).
12.07 Somatic symptom and related disorders (see 12.00B6), satisfied by A and B:
A. Medical documentation of one or more of the following:
1. Symptoms of altered voluntary motor or sensory function that are not better explained by another medical or mental disorder;
2. One or more somatic symptoms that are distressing, with excessive thoughts, feelings, or behaviors related to the symptoms; or
3. Preoccupation with having or acquiring a serious illness without significant symptoms present.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 12.00F):
1. Understand, remember, or apply information (see 12.00E1).
2. Interact with others (see 12.00E2).
3. Concentrate, persist, or maintain pace (see 12.00E3).
4. Adapt or manage oneself (see 12.00E4).
12.08 Personality and impulse-control disorders (see 12.00B7), satisfied by A and B:
A. Medical documentation of a pervasive pattern of one or more of the following:
1. Distrust and suspiciousness of others;
2. Detachment from social relationships;
3. Disregard for and violation of the rights of others;
4. Instability of interpersonal relationships;
5. Excessive emotionality and attention seeking;
6. Feelings of inadequacy;
7. Excessive need to be taken care of;
8. Preoccupation with perfectionism and orderliness; or
9. Recurrent, impulsive, aggressive behavioral outbursts.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 12.00F):
1. Understand, remember, or apply information (see 12.00E1).
2. Interact with others (see 12.00E2).
3. Concentrate, persist, or maintain pace (see 12.00E3).
4. Adapt or manage oneself (see 12.00E4).
12.09 [Reserved]
12.10 Autism spectrum disorder (see 12.00B8), satisfied by A and B:
A. Medical documentation of both of the following:
1. Qualitative deficits in verbal communication, nonverbal communication, and social interaction; and
2. Significantly restricted, repetitive patterns of behavior, interests, or activities.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 12.00F):
1. Understand, remember, or apply information (see 12.00E1).
2. Interact with others (see 12.00E2).
3. Concentrate, persist, or maintain pace (see 12.00E3).
4. Adapt or manage oneself (see 12.00E4).
12.11 Neurodevelopmental disorders (see 12.00B9), satisfied by A and B:
A. Medical documentation of the requirements of paragraph 1, 2, or 3:
1. One or both of the following:
a. Frequent distractibility, difficulty sustaining attention, and difficulty organizing tasks; or
b. Hyperactive and impulsive behavior (for example, difficulty remaining seated, talking excessively, difficulty waiting, appearing restless, or behaving as if being “driven by a motor”).
2. Significant difficulties learning and using academic skills; or
3. Recurrent motor movement or vocalization.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 12.00F):
1. Understand, remember, or apply information (see 12.00E1).
2. Interact with others (see 12.00E2).
3. Concentrate, persist, or maintain pace (see 12.00E3).
4. Adapt or manage oneself (see 12.00E4).
12.12 [Reserved]
12.13 Eating disorders (see 12.00B10), satisfied by A and B:
A. Medical documentation of a persistent alteration in eating or eating-related behavior that results in a change in consumption or absorption of food and that significantly impairs physical or psychological health.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 12.00F):
1. Understand, remember, or apply information (see 12.00E1).
2. Interact with others (see 12.00E2).
3. Concentrate, persist, or maintain pace (see 12.00E3).
4. Adapt or manage oneself (see 12.00E4).
12.15 Trauma- and stressor-related disorders (see 12.00B11), satisfied by A and B, or A and C:
A. Medical documentation of all of the following:
1. Exposure to actual or threatened death, serious injury, or violence;
2. Subsequent involuntary re-experiencing of the traumatic event (for example, intrusive memories, dreams, or flashbacks);
3. Avoidance of external reminders of the event;
4. Disturbance in mood and behavior; and
5. Increases in arousal and reactivity (for example, exaggerated startle response, sleep disturbance).
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 12.00F):
1. Understand, remember, or apply information (see 12.00E1).
2. Interact with others (see 12.00E2).
3. Concentrate, persist, or maintain pace (see 12.00E3).
4. Adapt or manage oneself (see 12.00E4).
OR
C. Your mental disorder in this listing category is “serious and persistent;” that is, you have a medically documented history of the existence of the disorder over a period of at least 2 years, and there is evidence of both:
1. Medical treatment, mental health therapy, psychosocial support(s), or a highly structured setting(s) that is ongoing and that diminishes the symptoms and signs of your mental disorder (see 12.00G2b); and
2. Marginal adjustment, that is, you have minimal capacity to adapt to changes in your environment or to demands that are not already part of your daily life (see 12.00G2c).
13.00 Cancer (Malignant Neoplastic Diseases)
A. What impairments do these listings cover? We use these listings to evaluate all cancers (malignant neoplastic diseases) except certain cancers associated with human immunodeficiency virus (HIV) infection. We use the criteria in 14.11B to evaluate primary central nervous system lymphoma, 14.11C to evaluate primary effusion lymphoma, and 14.11E to evaluate pulmonary Kaposi sarcoma if you also have HIV infection. We evaluate all other cancers associated with HIV infection, for example, Hodgkin lymphoma or non-pulmonary Kaposi sarcoma, under this body system or under 14.11F-I in the immune system disorders body system.
B. What do we consider when we evaluate cancer under these listings? We will consider factors including:
1. Origin of the cancer.
2. Extent of involvement.
3. Duration, frequency, and response to anticancer therapy.
4. Effects of any post-therapeutic residuals.
C. How do we apply these listings? We apply the criteria in a specific listing to a cancer originating from that specific site.
D. What evidence do we need?
1. We need medical evidence that specifies the type, extent, and site of the primary, recurrent, or metastatic lesion. When the primary site cannot be identified, we will use evidence documenting the site(s) of metastasis to evaluate the impairment under 13.27.
2. For operative procedures, including a biopsy or a needle aspiration, we generally need a copy of both the:
a. Operative note, and
b. Pathology report.
3. When we cannot get these documents, we will accept the summary of hospitalization(s) or other medical reports. This evidence should include details of the findings at surgery and, whenever appropriate, the pathological findings.
4. In some situations, we may also need evidence about recurrence, persistence, or progression of the cancer, the response to therapy, and any significant residuals. (See 13.00G.)
E. When do we need longitudinal evidence?
1. Cancer with distant metastases. We generally do not need longitudinal evidence for cancer that has metastasized beyond the regional lymph nodes because this cancer usually meets the requirements of a listing. Exceptions are for cancer with distant metastases that we expect to respond to anticancer therapy. For these exceptions, we usually need a longitudinal record of 3 months after therapy starts to determine whether the therapy achieved its intended effect, and whether this effect is likely to persist.
2. Other cancers. When there are no distant metastases, many of the listings require that we consider your response to initial anticancer therapy; that is, the initial planned treatment regimen. This therapy may consist of a single modality or a combination of modalities; that is, multimodal therapy. (See 13.00I4.)
3. Types of treatment.
a. Whenever the initial planned therapy is a single modality, enough time must pass to allow a determination about whether the therapy will achieve its intended effect. If the treatment fails, the failure often happens within 6 months after treatment starts, and there will often be a change in the treatment regimen.
b. Whenever the initial planned therapy is multimodal, we usually cannot make a determination about the effectiveness of the therapy until we can determine the effects of all the planned modalities. In some cases, we may need to defer adjudication until we can assess the effectiveness of therapy. However, we do not need to defer adjudication to determine whether the therapy will achieve its intended effect if we can make a fully favorable determination or decision based on the length and effects of therapy, or the residuals of the cancer or therapy (see 13.00G).
c. We need evidence under 13.02E, 13.11D, and 13.14C to establish that your treating source initiated multimodal anticancer therapy. We do not need to make a determination about the length or effectiveness of your therapy. Multimodal therapy has been initiated, and satisfies the requirements in 13.02E, 13.11D, and 13.14C, when your treating source starts the first modality. We may defer adjudication if your treating source plans multimodal therapy and has not yet initiated it.
F. How do we evaluate impairments that do not meet one of the cancer listings?
1. These listings are only examples of cancer that we consider severe enough to prevent you from doing any gainful activity. If your severe impairment(s) does not meet the criteria of any of these listings, we must also consider whether you have an impairment(s) that meets the criteria of a listing in another body system.
2. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. (See §§ 404.1526 and 416.926 of this chapter.) If your impairment(s) does not meet or medically equal a listing, you may or may not have the residual functional capacity to engage in substantial gainful activity. In that situation, we proceed to the fourth, and, if necessary, the fifth steps of the sequential evaluation process in §§ 404.1520 and 416.920 of this chapter. We use the rules in §§ 404.1594 and 416.994 of this chapter, as appropriate, when we decide whether you continue to be disabled.
G. How do we consider the effects of anticancer therapy?
1. How we consider the effects of anticancer therapy under the listings. In many cases, cancers meet listing criteria only if the therapy is not effective and the cancer persists, progresses, or recurs. However, as explained in the following paragraphs, we will not delay adjudication if we can make a fully favorable determination or decision based on the evidence in the case record.
2. Effects can vary widely.
a. We consider each case on an individual basis because the therapy and its toxicity may vary widely. We will request a specific description of the therapy, including these items:
i. Drugs given.
ii. Dosage.
iii. Frequency of drug administration.
iv. Plans for continued drug administration.
v. Extent of surgery.
vi. Schedule and fields of radiation therapy.
b. We will also request a description of the complications or adverse effects of therapy, such as the following:
i. Continuing gastrointestinal symptoms.
ii. Persistent weakness.
iii. Neurological complications.
iv. Cardiovascular complications.
v. Reactive mental disorders.
3. Effects of therapy may change. The severity of the adverse effects of anticancer therapy may change during treatment; therefore, enough time must pass to allow us to evaluate the therapy's effect. The residual effects of treatment are temporary in most instances; however, on occasion, the effects may be disabling for a consecutive period of at least 12 months. In some situations, very serious adverse effects may interrupt and prolong multimodal anticancer therapy for a continuous period of almost 12 months. In these situations, we may determine there is an expectation that your impairment will preclude you from engaging in any gainful activity for at least 12 months.
4. When the initial anticancer therapy is effective. We evaluate any post-therapeutic residual impairment(s) not included in these listings under the criteria for the affected body system. We must consider any complications of therapy. When the residual impairment(s) does not meet or medically equal a listing, we must consider its effect on your ability to do substantial gainful activity.
H. How long do we consider your impairment to be disabling?
1. In some listings, we specify that we will consider your impairment to be disabling until a particular point in time (for example, until at least 12 months from the date of transplantation). We may consider your impairment to be disabling beyond this point when the medical and other evidence justifies it.
2. When a listing does not contain such a specification, we will consider an impairment(s) that meets or medically equals a listing in this body system to be disabling until at least 3 years after onset of complete remission. When the impairment(s) has been in complete remission for at least 3 years, that is, the original tumor or a recurrence (or relapse) and any metastases have not been evident for at least 3 years, the impairment(s) will no longer meet or medically equal the criteria of a listing in this body system.
3. Following the appropriate period, we will consider any residuals, including residuals of the cancer or therapy (see 13.00G), in determining whether you are disabled. If you have a recurrence or relapse of your cancer, your impairment may meet or medically equal one of the listings in this body system again.
I. What do we mean by the following terms?
1. Anticancer therapy means surgery, radiation, chemotherapy, hormones, immunotherapy, or bone marrow or stem cell transplantation. When we refer to surgery as an anticancer treatment, we mean surgical excision for treatment, not for diagnostic purposes.
2. Inoperable means surgery is thought to be of no therapeutic value or the surgery cannot be performed; for example, when you cannot tolerate anesthesia or surgery because of another impairment(s), or you have a cancer that is too large or that has invaded crucial structures. This term does not include situations in which your cancer could have been surgically removed but another method of treatment was chosen; for example, an attempt at organ preservation. Your physician may determine whether the cancer is inoperable before or after you receive neoadjuvant therapy. Neoadjuvant therapy is anticancer therapy, such as chemotherapy or radiation, given before surgery in order to reduce the size of the cancer.
3. Metastases means the spread of cancer cells by blood, lymph, or other body fluid. This term does not include the spread of cancer cells by direct extension of the cancer to other tissues or organs.
4. Multimodal therapy means anticancer therapy that is a combination of at least two types of treatment given in close proximity as a unified whole and usually planned before any treatment has begun. There are three types of treatment modalities: surgery, radiation, and systemic drug therapy (chemotherapy, hormone therapy, and immunotherapy or biological modifier therapy). Examples of multimodal therapy include:
a. Surgery followed by chemotherapy or radiation.
b. Chemotherapy followed by surgery.
c. Chemotherapy and concurrent radiation.
5. Persistent means the planned initial anticancer therapy failed to achieve a complete remission of your cancer; that is, your cancer is evident, even if smaller, after the therapy has ended.
6. Progressive means the cancer becomes more extensive after treatment; that is, there is evidence that your cancer is growing after you have completed at least half of your planned initial anticancer therapy.
7. Recurrent or relapse means the cancer that was in complete remission or entirely removed by surgery has returned.
8. Unresectable means surgery or surgeries did not completely remove the cancer. This term includes situations in which your cancer is incompletely resected or the surgical margins are positive. It does not include situations in which there is a finding of a positive margin(s) if additional surgery obtains a margin(s) that is clear. It also does not include situations in which the cancer is completely resected but you are receiving adjuvant therapy. Adjuvant therapy is anticancer therapy, such as chemotherapy or radiation, given after surgery in order to eliminate any remaining cancer cells or lessen the chance of recurrence.
J. Can we establish the existence of a disabling impairment prior to the date of the evidence that shows the cancer satisfies the criteria of a listing? Yes. We will consider factors such as:
1. The type of cancer and its location.
2. The extent of involvement when the cancer was first demonstrated.
3. Your symptoms.
K. How do we evaluate specific cancers?
1. Lymphoma.
a. Many indolent (non-aggressive) lymphomas are controlled by well-tolerated treatment modalities, although the lymphomas may produce intermittent symptoms and signs. We may defer adjudicating these cases for an appropriate period after therapy is initiated to determine whether the therapy will achieve its intended effect, which is usually to stabilize the disease process. (See 13.00E3.) Once your disease stabilizes, we will assess severity based on the extent of involvement of other organ systems and residuals from therapy.
b. A change in therapy for indolent lymphomas is usually an indicator that the therapy is not achieving its intended effect. However, your impairment will not meet the requirements of 13.05A2 if your therapy is changed solely because you or your physician chooses to change it and not because of a failure to achieve stability.
c. We consider Hodgkin lymphoma that recurs more than 12 months after completing initial anticancer therapy to be a new disease rather than a recurrence.
2. Leukemia.
a. Acute leukemia. The initial diagnosis of acute leukemia, including the accelerated or blast phase of chronic myelogenous (granulocytic) leukemia, is based on definitive bone marrow examination. Additional diagnostic information is based on chromosomal analysis, cytochemical and surface marker studies on the abnormal cells, or other methods consistent with the prevailing state of medical knowledge and clinical practice. Recurrent disease must be documented by peripheral blood, bone marrow, or cerebrospinal fluid examination, or by testicular biopsy. The initial and follow-up pathology reports should be included.
b. Chronic myelogenous leukemia (CML). We need a diagnosis of CML based on documented granulocytosis, including immature forms such as differentiated or undifferentiated myelocytes and myeloblasts, and a chromosomal analysis that demonstrates the Philadelphia chromosome. In the absence of a chromosomal analysis, or if the Philadelphia chromosome is not present, the diagnosis may be made by other methods consistent with the prevailing state of medical knowledge and clinical practice. The requirement for CML in the accelerated or blast phase is met in 13.06B if laboratory findings show the proportion of blast (immature) cells in the peripheral blood or bone marrow is 10 percent or greater.
c. Chronic lymphocytic leukemia.
i. We require the diagnosis of chronic lymphocytic leukemia (CLL) to be documented by evidence of a chronic lymphocytosis of at least 10,000 cells/mm3 for 3 months or longer, or other acceptable diagnostic techniques consistent with the prevailing state of medical knowledge and clinical practice.
ii. We evaluate the complications and residual impairment(s) from CLL under the appropriate listings, such as 13.05A2 or the hematological listings (7.00).
d. Elevated white cell count. In cases of chronic leukemia (either myelogenous or lymphocytic), an elevated white cell count, in itself, is not a factor in determining the severity of the impairment.
3. Macroglobulinemia or heavy chain disease. We require the diagnosis of these diseases to be confirmed by protein electrophoresis or immunoelectrophoresis. We evaluate the resulting impairment(s) under the appropriate listings, such as 13.05A2 or the hematological listings (7.00).
4. Primary breast cancer.
a. We evaluate bilateral primary breast cancer (synchronous or metachronous) under 13.10A, which covers local primary disease, and not as a primary disease that has metastasized.
b. We evaluate secondary lymphedema that results from anticancer therapy for breast cancer under 13.10E if the lymphedema is treated by surgery to salvage or restore the functioning of an upper extremity. Secondary lymphedema is edema that results from obstruction or destruction of normal lymphatic channels. We may not restrict our determination of the onset of disability to the date of the surgery; we may establish an earlier onset date of disability if the evidence in your case record supports such a finding.
5. Carcinoma-in-situ. Carcinoma-in-situ, or preinvasive carcinoma, usually responds to treatment. When we use the term “carcinoma” in these listings, it does not include carcinoma-in-situ.
6. Primary central nervous system (CNS) cancers. We use the criteria in 13.13 to evaluate cancers that originate within the CNS (that is, brain and spinal cord cancers).
a. The CNS cancers listed in 13.13A1 are highly malignant and respond poorly to treatment, and therefore we do not require additional criteria to evaluate them. We do not list pituitary gland cancer (for example, pituitary gland carcinoma) in 13.13A1, although this CNS cancer is highly malignant and responds poorly to treatment. We evaluate pituitary gland cancer under 13.13A1 and do not require additional criteria to evaluate it.
b. We consider a CNS tumor to be malignant if it is classified as Grade II, Grade III, or Grade IV under the World Health Organization (WHO) classification of tumors of the CNS (WHO Classification of Tumours of the Central Nervous System, 2007).
c. We evaluate benign (for example, WHO Grade I) CNS tumors under 11.05. We evaluate metastasized CNS cancers from non-CNS sites under the primary cancers (see 13.00C). We evaluate any complications of CNS cancers, such as resultant neurological or psychological impairments, under the criteria for the affected body system.
7. Primary peritoneal carcinoma. We use the criteria in 13.23E to evaluate primary peritoneal carcinoma in women because this cancer is often indistinguishable from ovarian cancer and is generally treated the same way as ovarian cancer. We use the criteria in 13.15A to evaluate primary peritoneal carcinoma in men because many of these cases are similar to malignant mesothelioma.
8. Prostate cancer. We exclude “biochemical recurrence” in 13.24A, which is defined as an increase in the serum prostate-specific antigen (PSA) level following the completion of the hormonal intervention therapy. We need corroborating evidence to document recurrence, such as radiological studies or findings on physical examination.
9. Melanoma. We evaluate malignant melanoma that affects the skin (cutaneous melanoma), eye (ocular melanoma), or mucosal membranes (mucosal melanoma) under 13.29. We evaluate melanoma that is not malignant that affects the skin (benign melanocytic tumor) under the listings in 8.00 or other affected body systems.
L. How do we evaluate cancer treated by bone marrow or stem cell transplantation, including transplantation using stem cells from umbilical cord blood? Bone marrow or stem cell transplantation is performed for a variety of cancers. We require the transplantation to occur before we evaluate it under these listings. We do not need to restrict our determination of the onset of disability to the date of the transplantation (13.05, 13.06, or 13.07) or the date of first treatment under the treatment plan that includes transplantation (13.28). We may be able to establish an earlier onset date of disability due to your transplantation if the evidence in your case record supports such a finding.
1. Acute leukemia (including T-cell lymphoblastic lymphoma) or accelerated or blast phase of CML. If you undergo bone marrow or stem cell transplantation for any of these disorders, we will consider you to be disabled until at least 24 months from the date of diagnosis or relapse, or at least 12 months from the date of transplantation, whichever is later.
2. Lymphoma, multiple myeloma, or chronic phase of CML. If you undergo bone marrow or stem cell transplantation for any of these disorders, we will consider you to be disabled until at least 12 months from the date of transplantation.
3. Other cancers. We will evaluate any other cancer treated with bone marrow or stem cell transplantation under 13.28, regardless of whether there is another listing that addresses that impairment. The length of time we will consider you to be disabled depends on whether you undergo allogeneic or autologous transplantation.
a. Allogeneic bone marrow or stem cell transplantation. If you undergo allogeneic transplantation (transplantation from an unrelated donor or a related donor other than an identical twin), we will consider you to be disabled until at least 12 months from the date of transplantation.
b. Autologous bone marrow or stem cell transplantation. If you undergo autologous transplantation (transplantation of your own cells or cells from your identical twin (syngeneic transplantation)), we will consider you to be disabled until at least 12 months from the date of the first treatment under the treatment plan that includes transplantation. The first treatment usually refers to the initial therapy given to prepare you for transplantation.
4. Evaluating disability after the appropriate time period has elapsed. We consider any residual impairment(s), such as complications arising from:
a. Graft-versus-host (GVH) disease.
b. Immunosuppressant therapy, such as frequent infections.
c. Significant deterioration of other organ systems.
13.01 Category of Impairments, Malignant Neoplastic Diseases
13.02 Soft tissue cancers of the head and neck (except salivary glands - 13.08 - and thyroid gland - 13.09).
A. Inoperable or unresectable.
OR
B. Persistent or recurrent disease following initial anticancer therapy, except persistence or recurrence in the true vocal cord.
OR
C. With metastases beyond the regional lymph nodes.
OR
D. Small-cell (oat cell) carcinoma.
OR
E. Soft tissue cancers originating in the head and neck treated with multimodal anticancer therapy (see 13.00E3c). Consider under a disability until at least 18 months from the date of diagnosis. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
13.03 Skin.
A. Sarcoma or carcinoma with metastases to or beyond the regional lymph nodes.
OR
B. Carcinoma invading deep extradermal structures (for example, skeletal muscle, cartilage, or bone).
13.04 Soft tissue sarcoma.
A. With regional or distant metastases.
OR
B. Persistent or recurrent following initial anticancer therapy.
13.05 Lymphoma (including mycosis fungoides, but excluding T-cell lymphoblastic lymphoma - 13.06). (See 13.00K1 and 13.00K2c.)
A. Non-Hodgkin's lymphoma, as described in 1 or 2:
1. Aggressive lymphoma (including diffuse large B-cell lymphoma) persistent or recurrent following initial anticancer therapy.
2. Indolent lymphoma (including mycosis fungoides and follicular small cleaved cell) requiring initiation of more than one (single mode or multimodal) anticancer treatment regimen within a period of 12 consecutive months. Consider under a disability from at least the date of initiation of the treatment regimen that failed within 12 months.
OR
B. Hodgkin lymphoma with failure to achieve clinically complete remission, or recurrent lymphoma within 12 months of completing initial anticancer therapy.
OR
C. With bone marrow or stem cell transplantation. Consider under a disability until at least 12 months from the date of transplantation. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
OR
D. Mantle cell lymphoma.
13.06 Leukemia. (See 13.00K2.)
A. Acute leukemia (including T-cell lymphoblastic lymphoma). Consider under a disability until at least 24 months from the date of diagnosis or relapse, or at least 12 months from the date of bone marrow or stem cell transplantation, whichever is later. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
OR
B. Chronic myelogenous leukemia, as described in 1 or 2:
1. Accelerated or blast phase (see 13.00K2b). Consider under a disability until at least 24 months from the date of diagnosis or relapse, or at least 12 months from the date of bone marrow or stem cell transplantation, whichever is later. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
2. Chronic phase, as described in a or b:
a. Consider under a disability until at least 12 months from the date of bone marrow or stem cell transplantation. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
b. Progressive disease following initial anticancer therapy.
13.07 Multiple myeloma (confirmed by appropriate serum or urine protein electrophoresis and bone marrow findings).
A. Failure to respond or progressive disease following initial anticancer therapy.
OR
B. With bone marrow or stem cell transplantation. Consider under a disability until at least 12 months from the date of transplantation. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
13.08 Salivary glands - carcinoma or sarcoma with metastases beyond the regional lymph nodes.
13.09 Thyroid gland.
A. Anaplastic (undifferentiated) carcinoma.
OR
B. Carcinoma with metastases beyond the regional lymph nodes progressive despite radioactive iodine therapy.
OR
C. Medullary carcinoma with metastases beyond the regional lymph nodes.
13.10 Breast (except sarcoma - 13.04). (See 13.00K4.)
A. Locally advanced cancer (inflammatory carcinoma, cancer of any size with direct extension to the chest wall or skin, or cancer of any size with metastases to the ipsilateral internal mammary nodes).
OR
B. Carcinoma with metastases to the supraclavicular or infraclavicular nodes, to 10 or more axillary nodes, or with distant metastases.
OR
C. Recurrent carcinoma, except local recurrence that remits with anticancer therapy.
OR
D. Small-cell (oat cell) carcinoma.
OR
E. With secondary lymphedema that is caused by anticancer therapy and treated by surgery to salvage or restore the functioning of an upper extremity. (See 13.00K4b.) Consider under a disability until at least 12 months from the date of the surgery that treated the secondary lymphedema. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
13.11 Skeletal system - sarcoma.
A. Inoperable or unresectable.
OR
B. Recurrent cancer (except local recurrence) after initial anticancer therapy.
OR
C. With distant metastases.
OR
D. All other cancers originating in bone with multimodal anticancer therapy (see 13.00E3c). Consider under a disability for 12 months from the date of diagnosis. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
13.12 Maxilla, orbit, or temporal fossa.
A. Sarcoma or carcinoma of any type with regional or distant metastases.
OR
B. Carcinoma of the antrum with extension into the orbit or ethmoid or sphenoid sinus.
OR
C. Cancer with extension to the orbit, meninges, sinuses, or base of the skull.
13.13 Nervous system. (See 13.00K6.)
A. Primary central nervous system (CNS; that is, brain and spinal cord) cancers, as described in 1, 2, or 3:
1. Glioblastoma multiforme, ependymoblastoma, and diffuse intrinsic brain stem gliomas (see 13.00K6a).
2. Any Grade III or Grade IV CNS cancer (see 13.00K6b), including astrocytomas, sarcomas, and medulloblastoma and other primitive neuroectodermal tumors (PNETs).
3. Any primary CNS cancer, as described in a or b:
a. Metastatic.
b. Progressive or recurrent following initial anticancer therapy.
OR
B. Primary peripheral nerve or spinal root cancers, as described in 1 or 2:
1. Metastatic.
2. Progressive or recurrent following initial anticancer therapy.
13.14 Lungs.
A. Non-small-cell carcinoma - inoperable, unresectable, recurrent, or metastatic disease to or beyond the hilar nodes.
OR
B. Small-cell (oat cell) carcinoma.
OR
C. Carcinoma of the superior sulcus (including Pancoast tumors) with multimodal anticancer therapy (see 13.00E3c). Consider under a disability until at least 18 months from the date of diagnosis. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
13.15 Pleura or mediastinum.
A. Malignant mesothelioma of pleura.
OR
B. Tumors of the mediastinum, as described in 1 or 2:
1. With metastases to or beyond the regional lymph nodes.
2. Persistent or recurrent following initial anticancer therapy.
OR
C. Small-cell (oat cell) carcinoma.
13.16 Esophagus or stomach.
A. Carcinoma or sarcoma of the esophagus.
OR
B. Carcinoma or sarcoma of the stomach, as described in 1 or 2:
1. Inoperable, unresectable, extending to surrounding structures, or recurrent.
2. With metastases to or beyond the regional lymph nodes.
OR
C. Small-cell (oat cell) carcinoma.
13.17 Small intestine - carcinoma, sarcoma, or carcinoid.
A. Inoperable, unresectable, or recurrent.
OR
B. With metastases beyond the regional lymph nodes.
OR
C. Small-cell (oat cell) carcinoma.
13.18 Large intestine (from ileocecal valve to and including anal canal).
A. Adenocarcinoma that is inoperable, unresectable, or recurrent.
OR
B. Squamous cell carcinoma of the anus, recurrent after surgery.
OR
C. With metastases beyond the regional lymph nodes.
OR
D. Small-cell (oat cell) carcinoma.
13.19 Liver or gallbladder - cancer of the liver, gallbladder, or bile ducts.
13.20 Pancreas.
A. Carcinoma (except islet cell carcinoma).
OR
B. Islet cell carcinoma that is physiologically active and is either inoperable or unresectable.
13.21 Kidneys, adrenal glands, or ureters - carcinoma.
A. Inoperable, unresectable, or recurrent.
OR
B. With metastases to or beyond the regional lymph nodes.
13.22 Urinary bladder - carcinoma.
A. With infiltration beyond the bladder wall.
OR
B. Recurrent after total cystectomy.
OR
C. Inoperable or unresectable.
OR
D. With metastases to or beyond the regional lymph nodes.
OR
E. Small-cell (oat cell) carcinoma.
13.23 Cancers of the female genital tract - carcinoma or sarcoma (including primary peritoneal carcinoma).
A. Uterus (corpus), as described in 1, 2, or 3:
1. Invading adjoining organs.
2. With metastases to or beyond the regional lymph nodes.
3. Persistent or recurrent following initial anticancer therapy.
OR
B. Uterine cervix, as described in 1, 2, or 3:
1. Extending to the pelvic wall, lower portion of the vagina, or adjacent or distant organs.
2. Persistent or recurrent following initial anticancer therapy.
3. With metastases to distant (for example, para-aortic or supraclavicular) lymph nodes.
OR
C. Vulva or vagina, as described in 1, 2, or 3:
1. Invading adjoining organs.
2. With metastases to or beyond the regional lymph nodes.
3. Persistent or recurrent following initial anticancer therapy.
OR
D. Fallopian tubes, as described in 1 or 2:
1. Extending to the serosa or beyond.
2. Persistent or recurrent following initial anticancer therapy.
E. Ovaries, as described in 1 or 2:
1. All cancers except germ-cell cancers, with at least one of the following:
a. Extension beyond the pelvis; for example, implants on, or direct extension to, peritoneal, omental, or bowel surfaces.
b. Metastases to or beyond the regional lymph nodes.
c. Recurrent following initial anticancer therapy.
2. Germ-cell cancers - progressive or recurrent following initial anticancer therapy.
OR
F. Small-cell (oat cell) carcinoma.
13.24 Prostate gland - carcinoma.
A. Progressive or recurrent (not including biochemical recurrence) despite initial hormonal intervention. (See 13.00K8.)
OR
B. With visceral metastases (metastases to internal organs).
OR
C. Small cell (oat cell) carcinoma.
13.25 Testicles - cancer with metastatic disease progressive or recurrent following initial chemotherapy.
13.26 Penis - carcinoma with metastases to or beyond the regional lymph nodes.
13.27 Primary site unknown after appropriate search for primary - metastatic carcinoma or sarcoma, except for squamous cell carcinoma confined to the neck nodes.
13.28 Cancer treated by bone marrow or stem cell transplantation. (See 13.00L.)
A. Allogeneic transplantation. Consider under a disability until at least 12 months from the date of transplantation. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
OR
B. Autologous transplantation. Consider under a disability until at least 12 months from the date of the first treatment under the treatment plan that includes transplantation. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
13.29 Malignant melanoma (including skin, ocular, or mucosal melanomas), as described in either A, B, or C:
A. Recurrent (except an additional primary melanoma at a different site, which is not considered to be recurrent disease) following either 1 or 2:
1. Wide excision (skin melanoma).
2. Enucleation of the eye (ocular melanoma).
OR
B. With metastases as described in 1, 2, or 3:
1. Metastases to one or more clinically apparent nodes; that is, nodes that are detected by imaging studies (excluding lymphoscintigraphy) or by clinical evaluation (palpable).
2. If the nodes are not clinically apparent, with metastases to four or more nodes.
3. Metastases to adjacent skin (satellite lesions) or distant sites (for example, liver, lung, or brain).
OR
C. Mucosal melanoma.
14.00 Immune System Disorders
A. What disorders do we evaluate under the immune system disorders listings?
1. We evaluate immune system disorders that cause dysfunction in one or more components of your immune system.
a. The dysfunction may be due to problems in antibody production, impaired cell-mediated immunity, a combined type of antibody/cellular deficiency, impaired phagocytosis, or complement deficiency.
b. Immune system disorders may result in recurrent and unusual infections, or inflammation and dysfunction of the body's own tissues. Immune system disorders can cause a deficit in a single organ or body system that results in extreme (that is, very serious) loss of function. They can also cause lesser degrees of limitations in two or more organs or body systems, and when associated with symptoms or signs, such as severe fatigue, fever, malaise, diffuse musculoskeletal pain, or involuntary weight loss, can also result in extreme limitation.
c. We organize the discussions of immune system disorders in three categories: Autoimmune disorders; Immune deficiency disorders, excluding human immunodeficiency virus (HIV) infection; and HIV infection.
2. Autoimmune disorders (14.00D). Autoimmune disorders are caused by dysfunctional immune responses directed against the body's own tissues, resulting in chronic, multisystem impairments that differ in clinical manifestations, course, and outcome. They are sometimes referred to as rheumatic diseases, connective tissue disorders, or collagen vascular disorders. Some of the features of autoimmune disorders in adults differ from the features of the same disorders in children.
3. Immune deficiency disorders, excluding HIV infection (14.00E). Immune deficiency disorders are characterized by recurrent or unusual infections that respond poorly to treatment, and are often associated with complications affecting other parts of the body. Immune deficiency disorders are classified as either primary (congenital) or acquired. Individuals with immune deficiency disorders also have an increased risk of malignancies and of having autoimmune disorders.
4. Human immunodeficiency virus (HIV) infection (14.00F). HIV infection may be characterized by increased susceptibility to common infections as well as opportunistic infections, cancers, or other conditions listed in 14.11.
B. What information do we need to show that you have an immune system disorder? Generally, we need your medical history, a report(s) of a physical examination, a report(s) of laboratory findings, and in some instances, appropriate medically acceptable imaging or tissue biopsy reports to show that you have an immune system disorder. Therefore, we will make every reasonable effort to obtain your medical history, medical findings, and results of laboratory tests. We explain the information we need in more detail in the sections below.
C. Definitions
1. Appropriate medically acceptable imaging includes, but is not limited to, angiography, x-ray imaging, computerized axial tomography (CAT scan) or magnetic resonance imaging (MRI), with or without contrast material, myelography, and radionuclear bone scans. “Appropriate” means that the technique used is the proper one to support the evaluation and diagnosis of the impairment.
2. Constitutional symptoms or signs, as used in these listings, means severe fatigue, fever, malaise, or involuntary weight loss. Severe fatigue means a frequent sense of exhaustion that results in significantly reduced physical activity or mental function. Malaise means frequent feelings of illness, bodily discomfort, or lack of well-being that result in significantly reduced physical activity or mental function.
3. Disseminated means that a condition is spread over a considerable area. The type and extent of the spread will depend on your specific disease.
4. Dysfunction means that one or more of the body regulatory mechanisms are impaired, causing either an excess or deficiency of immunocompetent cells or their products.
5. Extra-articular means “other than the joints”; for example, an organ(s) such as the heart, lungs, kidneys, or skin.
6. Documented medical need has the same meaning as in 1.00C6a.
7. Fine and gross movements has the same meaning as in 1.00E4.
8. Major joint of an upper or a lower extremity has the same meaning as in 1.00I2 and 1.00I3.
9. Persistent means that a sign(s) or symptom(s) has continued over time. The precise meaning will depend on the specific immune system disorder, the usual course of the disorder, and the other circumstances of your clinical course.
10. Recurrent means that a condition that previously responded adequately to an appropriate course of treatment returns after a period of remission or regression. The precise meaning, such as the extent of response or remission and the time periods involved, will depend on the specific disease or condition you have, the body system affected, the usual course of the disorder and its treatment, and the other facts of your particular case.
11. Resistant to treatment means that a condition did not respond adequately to an appropriate course of treatment. Whether a response is adequate or a course of treatment is appropriate will depend on the specific disease or condition you have, the body system affected, the usual course of the disorder and its treatment, and the other facts of your particular case.
12. Severe means medical severity as used by the medical community. The term does not have the same meaning as it does when we use it in connection with a finding at the second step of the sequential evaluation process in §§ 404.1520 and 416.920 of this chapter.
D. How do we document and evaluate the listed autoimmune disorders?
1. Systemic lupus erythematosus (14.02).
a. General. Systemic lupus erythematosus (SLE) is a chronic inflammatory disease that can affect any organ or body system. It is frequently, but not always, accompanied by constitutional symptoms or signs (severe fatigue, fever, malaise, involuntary weight loss). Major organ or body system involvement can include: Respiratory (pleuritis, pneumonitis), cardiovascular (endocarditis, myocarditis, pericarditis, vasculitis), renal (glomerulonephritis), hematologic (anemia, leukopenia, thrombocytopenia), skin (photosensitivity), neurologic (seizures), mental (anxiety, fluctuating cognition (“lupus fog”), mood disorders, organic brain syndrome, psychosis), or immune system disorders (inflammatory arthritis). Immunologically, there is an array of circulating serum auto-antibodies and pro- and anti-coagulant proteins that may occur in a highly variable pattern.
b. Documentation of SLE. Generally, but not always, the medical evidence will show that your SLE satisfies the criteria in the current “Criteria for the Classification of Systemic Lupus Erythematosus” by the American College of Rheumatology found in the most recent edition of the Primer on the Rheumatic Diseases published by the Arthritis Foundation.
2. Systemic vasculitis (14.03).
a. General.
(i) Vasculitis is an inflammation of blood vessels. It may occur acutely in association with adverse drug reactions, certain chronic infections, and occasionally, malignancies. More often, it is chronic and the cause is unknown. Symptoms vary depending on which blood vessels are involved. Systemic vasculitis may also be associated with other autoimmune disorders; for example, SLE or dermatomyositis.
(ii) There are several clinical patterns, including but not limited to polyarteritis nodosa, Takayasu's arteritis (aortic arch arteritis), giant cell arteritis (temporal arteritis), and Wegener's granulomatosis.
b. Documentation of systemic vasculitis. Angiography or tissue biopsy confirms a diagnosis of systemic vasculitis when the disease is suspected clinically. When you have had angiography or tissue biopsy for systemic vasculitis, we will make every reasonable effort to obtain reports of the results of that procedure. However, we will not purchase angiography or tissue biopsy.
3. Systemic sclerosis (scleroderma) (14.04).
a. General. Systemic sclerosis (scleroderma) constitutes a spectrum of disease in which thickening of the skin is the clinical hallmark. Raynaud's phenomenon, often medically severe and progressive, is present frequently and may be the peripheral manifestation of a vasospastic abnormality in the heart, lungs, and kidneys. The CREST syndrome (calcinosis, Raynaud's phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia) is a variant that may slowly progress over years to the generalized process, systemic sclerosis.
b. Diffuse cutaneous systemic sclerosis. In diffuse cutaneous systemic sclerosis (also known as diffuse scleroderma), major organ or systemic involvement can include the gastrointestinal tract, lungs, heart, kidneys, and muscle in addition to skin or blood vessels. Although arthritis can occur, joint dysfunction results primarily from soft tissue/cutaneous thickening, fibrosis, and contractures.
c. Localized scleroderma (linear scleroderma and morphea).
(i) Localized scleroderma (linear scleroderma and morphea) is more common in children than in adults. However, this type of scleroderma can persist into adulthood. To assess the severity of the impairment, we need a description of the extent of involvement of linear scleroderma and the location of the lesions. For example, linear scleroderma involving the arm but not crossing any joints is not as functionally limiting as sclerodactyly (scleroderma localized to the fingers). Linear scleroderma of a lower extremity involving skin thickening and atrophy of underlying muscle or bone can result in contractures and leg length discrepancy. In such cases, we may evaluate your impairment under the musculoskeletal listings (1.00).
(ii) When there is isolated morphea of the face causing facial disfigurement from unilateral hypoplasia of the mandible, maxilla, zygoma, or orbit, adjudication may be more appropriate under the criteria in the affected body system, such as special senses and speech (2.00) or mental disorders (12.00).
(iii) Chronic variants of these syndromes include disseminated morphea, Shulman's disease (diffuse fasciitis with eosinophilia), and eosinophilia-myalgia syndrome (often associated with toxins such as toxic oil or contaminated tryptophan), all of which can impose medically severe musculoskeletal dysfunction and may also lead to restrictive pulmonary disease. We evaluate these variants of the disease under the criteria in the musculoskeletal listings (1.00) or respiratory system listings (3.00).
d. Documentation of systemic sclerosis (scleroderma). Documentation involves differentiating the clinical features of systemic sclerosis (scleroderma) from other autoimmune disorders. However, there may be an overlap.
4. Polymyositis and dermatomyositis (14.05).
a. General. Polymyositis and dermatomyositis are related disorders that are characterized by an inflammatory process in striated muscle, occurring alone or in association with other autoimmune disorders or malignancy. The most common manifestations are symmetric weakness, and less frequently, pain and tenderness of the proximal limb-girdle (shoulder or pelvic) musculature. There may also be involvement of the cervical, cricopharyngeal, esophageal, intercostal, and diaphragmatic muscles.
b. Documentation of polymyositis and dermatomyositis. Generally, but not always, polymyositis is associated with elevated serum muscle enzymes (creatine phosphokinase (CPK), aminotransferases, and aldolase), and characteristic abnormalities on electromyography and muscle biopsy. In dermatomyositis there are characteristic skin findings in addition to the findings of polymyositis. When you have had electromyography or muscle biopsy for polymyositis or dermatomyositis, we will make every reasonable effort to obtain reports of the results of that procedure. However, we will not purchase electromyography or muscle biopsy.
c. Additional information about how we evaluate polymyositis and dermatomyositis under the listings.
(i) Weakness of your pelvic girdle muscles that results in your inability to rise independently from a squatting or sitting position or to climb stairs may be an indication that you are unable to walk without assistance. Weakness of your shoulder girdle muscles may result in your inability to perform lifting, carrying, and reaching overhead, and also may seriously affect your ability to perform activities requiring fine movements. We evaluate these limitations under 14.05A.
(ii) We use the malignant neoplastic diseases listings (13.00) to evaluate malignancies associated with polymyositis or dermatomyositis. We evaluate the involvement of other organs/body systems under the criteria for the listings in the affected body system.
5. Undifferentiated and mixed connective tissue disease (14.06).
a. General. This listing includes syndromes with clinical and immunologic features of several autoimmune disorders, but which do not satisfy the criteria for any of the specific disorders described. For example, you may have clinical features of SLE and systemic vasculitis, and the serologic (blood test) findings of rheumatoid arthritis.
b. Documentation of undifferentiated and mixed connective tissue disease. Undifferentiated connective tissue disease is diagnosed when clinical features and serologic (blood test) findings, such as rheumatoid factor or antinuclear antibody (consistent with an autoimmune disorder) are present but do not satisfy the criteria for a specific disease. Mixed connective tissue disease (MCTD) is diagnosed when clinical features and serologic findings of two or more autoimmune diseases overlap.
6. Inflammatory arthritis (14.09).
a. General. The spectrum of inflammatory arthritis includes a vast array of disorders that differ in cause, course, and outcome. Clinically, inflammation of major joints in an upper or a lower extremity may be the dominant manifestation causing difficulties with walking or fine and gross movements; there may be joint pain, swelling, and tenderness. The arthritis may affect other joints, or cause less limitation in walking or fine and gross movements. However, in combination with extra-articular features, including constitutional symptoms or signs (severe fatigue, fever, malaise, and involuntary weight loss), inflammatory arthritis may result in an extreme limitation.
b. Inflammatory arthritis involving the axial spine (spondyloarthropathy). In adults, inflammatory arthritis involving the axial spine may be associated with disorders such as:
(i) Reiter's syndrome;
(ii) Ankylosing spondylitis;
(iii) Psoriatic arthritis;
(iv) Whipple's disease;
(v) Behçet's disease; and
(vi) Inflammatory bowel disease.
c. Inflammatory arthritis involving the peripheral joints. In adults, inflammatory arthritis involving peripheral joints may be associated with disorders such as:
(i) Rheumatoid arthritis;
(ii) Sjögren's syndrome;
(iii) Psoriatic arthritis;
(iv) Crystal deposition disorders (gout and pseudogout);
(v) Lyme disease; and
(vi) Inflammatory bowel disease.
d. Documentation of inflammatory arthritis. Generally, but not always, the diagnosis of inflammatory arthritis is based on the clinical features and serologic findings described in the most recent edition of the Primer on the Rheumatic Diseases published by the Arthritis Foundation.
e. How we evaluate inflammatory arthritis under the listings.
(i) Listing-level severity in 14.09A and 14.09C1 is shown by the presence of an impairment-related physical limitation of functioning. In 14.09C1, if you have the required ankylosis (fixation) of your cervical or dorsolumbar spine, we will find that you have a listing-level impairment-related physical limitation in your ability to see in front of you, above you, and to the side, even though you might not require bilateral upper limb assistance.
(ii) Listing-level severity in 14.09B, 14.09C2, and 14.09D is shown by inflammatory arthritis that involves various combinations of complications (such as inflammation or deformity, extra-articular features, repeated manifestations, and constitutional symptoms and signs) of one or more major joints in an upper or a lower extremity (see 14.00C8) or other joints. Extra-articular impairments may also meet listings in other body systems.
(iii) Extra-articular features of inflammatory arthritis may involve any body system; for example: Musculoskeletal (heel enthesopathy), ophthalmologic (iridocyclitis, keratoconjunctivitis sicca, uveitis), pulmonary (pleuritis, pulmonary fibrosis or nodules, restrictive lung disease), cardiovascular (aortic valve insufficiency, arrhythmias, coronary arteritis, myocarditis, pericarditis, Raynaud's phenomenon, systemic vasculitis), renal (amyloidosis of the kidney), hematologic (chronic anemia, thrombocytopenia), neurologic (peripheral neuropathy, radiculopathy, spinal cord or cauda equina compression with sensory and motor loss), mental (cognitive dysfunction, poor memory), and immune system (Felty's syndrome (hypersplenism with compromised immune competence)).
(iv) If both inflammation and chronic deformities are present, we evaluate your impairment under the criteria of any appropriate listing.
7. Sjögren's syndrome (14.10).
a. General.
(i) Sjögren's syndrome is an immune-mediated disorder of the exocrine glands. Involvement of the lacrimal and salivary glands is the hallmark feature, resulting in symptoms of dry eyes and dry mouth, and possible complications, such as corneal damage, blepharitis (eyelid inflammation), dysphagia (difficulty in swallowing), dental caries, and the inability to speak for extended periods of time. Involvement of the exocrine glands of the upper airways may result in persistent dry cough.
(ii) Many other organ systems may be involved, including musculoskeletal (arthritis, myositis), respiratory (interstitial fibrosis), gastrointestinal (dysmotility, dysphagia, involuntary weight loss), genitourinary (interstitial cystitis, renal tubular acidosis), skin (purpura, vasculitis), neurologic (central nervous system disorders, cranial and peripheral neuropathies), mental (cognitive dysfunction, poor memory), and neoplastic (lymphoma). Severe fatigue and malaise are frequently reported. Sjögren's syndrome may be associated with other autoimmune disorders (for example, rheumatoid arthritis or SLE); usually the clinical features of the associated disorder predominate.
b. Documentation of Sjögren's syndrome. If you have Sjögren's syndrome, the medical evidence will generally, but not always, show that your disease satisfies the criteria in the current “Criteria for the Classification of Sjögren's Syndrome” by the American College of Rheumatology found in the most recent edition of the Primer on the Rheumatic Diseases published by the Arthritis Foundation.
E. How do we document and evaluate immune deficiency disorders, excluding HIV infection?
1. General.
a. Immune deficiency disorders can be classified as:
(i) Primary (congenital); for example, X-linked agammaglobulinemia, thymic hypoplasia (DiGeorge syndrome), severe combined immunodeficiency (SCID), chronic granulomatous disease (CGD), C1 esterase inhibitor deficiency.
(ii) Acquired; for example, medication-related.
b. Primary immune deficiency disorders are seen mainly in children. However, recent advances in the treatment of these disorders have allowed many affected children to survive well into adulthood. Occasionally, these disorders are first diagnosed in adolescence or adulthood.
2. Documentation of immune deficiency disorders. The medical evidence must include documentation of the specific type of immune deficiency. Documentation may be by laboratory evidence or by other generally acceptable methods consistent with the prevailing state of medical knowledge and clinical practice.
3. Immune deficiency disorders treated by stem cell transplantation.
a. Evaluation in the first 12 months. If you undergo stem cell transplantation for your immune deficiency disorder, we will consider you disabled until at least 12 months from the date of the transplant.
b. Evaluation after the 12-month period has elapsed. After the 12-month period has elapsed, we will consider any residuals of your immune deficiency disorder as well as any residual impairment(s) resulting from the treatment, such as complications arising from:
(i) Graft-versus-host (GVH) disease.
(ii) Immunosuppressant therapy, such as frequent infections.
(iii) Significant deterioration of other organ systems.
4. Medication-induced immune suppression. Medication effects can result in varying degrees of immune suppression, but most resolve when the medication is ceased. However, if you are prescribed medication for long-term immune suppression, such as after an organ transplant, we will evaluate:
a. The frequency and severity of infections.
b. Residuals from the organ transplant itself, after the 12-month period has elapsed.
c. Significant deterioration of other organ systems.
F. How do we document and evaluate HIV infection? Any individual with HIV infection, including one with a diagnosis of acquired immune deficiency syndrome (AIDS), may be found disabled under 14.11 if his or her impairment meets the criteria in that listing or is medically equivalent to the criteria in that listing.
1. Documentation of HIV infection.
a. Definitive documentation of HIV infection. We may document a diagnosis of HIV infection by positive findings on one or more of the following definitive laboratory tests:
(i) HIV antibody screening test (for example, enzyme immunoassay, or EIA), confirmed by a supplemental HIV antibody test such as the Western blot (immunoblot), an immunofluorescence assay, or an HIV-1/HIV-2 antibody differentiation immunoassay.
(ii) HIV nucleic acid (DNA or RNA) detection test (for example, polymerase chain reaction, or PCR).
(iii) HIV p24 antigen (p24Ag) test.
(iv) Isolation of HIV in viral culture.
(v) Other tests that are highly specific for detection of HIV and that are consistent with the prevailing state of medical knowledge.
b. We will make every reasonable effort to obtain the results of your laboratory testing. Pursuant to §§ 404.1519f and 416.919f of this chapter, we will purchase examinations or tests necessary to make a determination in your claim if no other acceptable documentation exists.
c. Other acceptable documentation of HIV infection. We may also document HIV infection without definitive laboratory evidence.
(i) We will accept a persuasive report from a physician that a positive diagnosis of your HIV infection was confirmed by an appropriate laboratory test(s), such as those described in 14.00F1a. To be persuasive, this report must state that you had the appropriate definitive laboratory test(s) for diagnosing your HIV infection and provide the results. The report must also be consistent with the remaining evidence of record.
(ii) We may also document HIV infection by the medical history, clinical and laboratory findings, and diagnosis(es) indicated in the medical evidence, provided that such documentation is consistent with the prevailing state of medical knowledge and clinical practice and is consistent with the other evidence in your case record. For example, we will accept a diagnosis of HIV infection without definitive laboratory evidence of the HIV infection if you have an opportunistic disease that is predictive of a defect in cell-mediated immunity (for example, toxoplasmosis of the brain or Pneumocystis pneumonia (PCP)), and there is no other known cause of diminished resistance to that disease (for example, long-term steroid treatment or lymphoma). In such cases, we will make every reasonable effort to obtain full details of the history, medical findings, and results of testing.
2. Documentation of the manifestations of HIV infection.
a. Definitive documentation of manifestations of HIV infection. We may document manifestations of HIV infection by positive findings on definitive laboratory tests, such as culture, microscopic examination of biopsied tissue or other material (for example, bronchial washings), serologic tests, or on other generally acceptable definitive tests consistent with the prevailing state of medical knowledge and clinical practice.
b. We will make every reasonable effort to obtain the results of your laboratory testing. Pursuant to §§ 404.1519f and 416.919f of this chapter, we will purchase examinations or tests necessary to make a determination of your claim if no other acceptable documentation exists.
c. Other acceptable documentation of manifestations of HIV infection. We may also document manifestations of HIV infection without definitive laboratory evidence.
(i) We will accept a persuasive report from a physician that a positive diagnosis of your manifestation of HIV infection was confirmed by an appropriate laboratory test(s). To be persuasive, this report must state that you had the appropriate definitive laboratory test(s) for diagnosing your manifestation of HIV infection and provide the results. The report must also be consistent with the remaining evidence of record.
(ii) We may also document manifestations of HIV infection without the definitive laboratory evidence described in 14.00F2a, provided that such documentation is consistent with the prevailing state of medical knowledge and clinical practice and is consistent with the other evidence in your case record. For example, many conditions are now commonly diagnosed based on some or all of the following: Medical history, clinical manifestations, laboratory findings (including appropriate medically acceptable imaging), and treatment responses. In such cases, we will make every reasonable effort to obtain full details of the history, medical findings, and results of testing.
3. Disorders associated with HIV infection (14.11A-E).
a. Multicentric Castleman disease (MCD, 14.11A) affects multiple groups of lymph nodes and organs containing lymphoid tissue. This widespread involvement distinguishes MCD from localized (or unicentric) Castleman disease, which affects only a single set of lymph nodes. While not a cancer, MCD is known as a lymphoproliferative disorder. Its clinical presentation and progression is similar to that of lymphoma, and its treatment may include radiation or chemotherapy. We require characteristic findings on microscopic examination of the biopsied lymph nodes or other generally acceptable methods consistent with the prevailing state of medical knowledge and clinical practice to establish the diagnosis. Localized (or unicentric) Castleman disease does not meet or medically equal the criterion in 14.11A, but we may evaluate it under the criteria in 14.11H or 14.11I.
b. Primary central nervous system lymphoma (PCNSL, 14.11B) originates in the brain, spinal cord, meninges, or eye. Imaging tests (for example, MRI) of the brain, while not diagnostic, may show a single lesion or multiple lesions in the white matter of the brain. We require characteristic findings on microscopic examination of the cerebral spinal fluid or of the biopsied brain tissue, or other generally acceptable methods consistent with the prevailing state of medical knowledge and clinical practice to establish the diagnosis.
c. Primary effusion lymphoma (PEL, 14.11C) is also known as body cavity lymphoma. We require characteristic findings on microscopic examination of the effusion fluid or of the biopsied tissue from the affected internal organ, or other generally acceptable methods consistent with the prevailing state of medical knowledge and clinical practice to establish the diagnosis.
d. Progressive multifocal leukoencephalopathy (PML, 14.11D) is a progressive neurological degenerative syndrome caused by the John Cunningham (JC) virus in immunosuppressed individuals. Clinical findings of PML include clumsiness, progressive weakness, and visual and speech changes. Personality and cognitive changes may also occur. We require appropriate clinical findings, characteristic white matter lesions on MRI, and a positive PCR test for the JC virus in the cerebrospinal fluid to establish the diagnosis. We also accept a positive brain biopsy for JC virus or other generally acceptable methods consistent with the prevailing state of medical knowledge and clinical practice to establish the diagnosis.
e. Pulmonary Kaposi sarcoma (Kaposi sarcoma in the lung, 14.11E) is the most serious form of Kaposi sarcoma (KS). Other internal KS tumors (for example, tumors of the gastrointestinal tract) have a more variable prognosis. We require characteristic findings on microscopic examination of the induced sputum, bronchoalveolar lavage washings, or of the biopsied transbronchial tissue, or by other generally acceptable methods consistent with the prevailing state of medical knowledge and clinical practice to establish the diagnosis.
4. CD4 measurement (14.11F). To evaluate your HIV infection under 14.11F, we require one measurement of your absolute CD4 count (also known as CD4 count or CD4+ T-helper lymphocyte count). This measurement must occur within the period we are considering in connection with your application or continuing disability review. If you have more than one measurement of your absolute CD4 count within this period, we will use your lowest absolute CD4 count.
5. Measurement of CD4 and either body mass index or hemoglobin (14.11G). To evaluate your HIV infection under 14.11G, we require one measurement of your absolute CD4 count or your CD4 percentage, and either a measurement of your body mass index (BMI) or your hemoglobin. These measurements must occur within the period we are considering in connection with your application or continuing disability review. If you have more than one measurement of your CD4 (absolute count or percentage), BMI, or hemoglobin within this period, we will use the lowest of your CD4 (absolute count or percentage), BMI, or hemoglobin. The date of your lowest CD4 (absolute count or percentage) measurement may be different from the date of your lowest BMI or hemoglobin measurement. We calculate your BMI using the formulas in 5.00G2.
6. Complications of HIV infection requiring hospitalization (14.11H).
a. Complications of HIV infection may include infections (common or opportunistic), cancers, and other conditions. Examples of complications that may result in hospitalization include: Depression; diarrhea; immune reconstitution inflammatory syndrome; malnutrition; and PCP and other severe infections.
b. Under 14.11H, we require three hospitalizations within a 12-month period that are at least 30 days apart and that result from a complication(s) of HIV infection. The hospitalizations may be for the same complication or different complications of HIV infection and are not limited to the examples of complications that may result in hospitalization listed in 14.00F6a. All three hospitalizations must occur within the period we are considering in connection with your application or continuing disability review. Each hospitalization must last at least 48 hours, including hours in a hospital emergency department immediately before the hospitalization.
c. We will use the rules on medical equivalence in §§ 404.1526 and 416.926 of this chapter to evaluate your HIV infection if you have fewer, but longer, hospitalizations, or more frequent, but shorter, hospitalizations, or if you receive nursing, rehabilitation, or other care in alternative settings.
7. HIV infection manifestations specific to women.
a. General. Most women with severe immunosuppression secondary to HIV infection exhibit the typical opportunistic infections and other conditions, such as PCP, Candida esophagitis, wasting syndrome, cryptococcosis, and toxoplasmosis. However, HIV infection may have different manifestations in women than in men. Adjudicators must carefully scrutinize the medical evidence and be alert to the variety of medical conditions specific to, or common in, women with HIV infection that may affect their ability to function in the workplace.
b. Additional considerations for evaluating HIV infection in women. Many of these manifestations (for example, vulvovaginal candidiasis or pelvic inflammatory disease) occur in women with or without HIV infection, but can be more severe or resistant to treatment, or occur more frequently in a woman whose immune system is suppressed. Therefore, when evaluating the claim of a woman with HIV infection, it is important to consider gynecologic and other problems specific to women, including any associated symptoms (for example, pelvic pain), in assessing the severity of the impairment and resulting functional limitations. We may evaluate manifestations of HIV infection in women under 14.11H-I, or under the criteria for the appropriate body system (for example, cervical cancer under 13.23).
8. HIV-associated dementia (HAD). HAD is an advanced neurocognitive disorder, characterized by a significant decline in cognitive functioning. We evaluate HAD under 14.11I. Other names associated with neurocognitive disorders due to HIV infection include: AIDS dementia complex, HIV dementia, HIV encephalopathy, and major neurocognitive disorder due to HIV infection.
G. How do we consider the effects of treatment in evaluating your autoimmune disorder, immune deficiency disorder, or HIV infection?
1. General. If your impairment does not otherwise meet the requirements of a listing, we will consider your medical treatment in terms of its effectiveness in improving the signs, symptoms, and laboratory abnormalities of your specific immune system disorder or its manifestations, and in terms of any side effects that limit your functioning. We will make every reasonable effort to obtain a specific description of the treatment you receive (including surgery) for your immune system disorder. We consider:
a. The effects of medications you take.
b. Adverse side effects (acute and chronic).
c. The intrusiveness and complexity of your treatment (for example, the dosing schedule, need for injections).
d. The effect of treatment on your mental functioning (for example, cognitive changes, mood disturbance).
e. Variability of your response to treatment (see 14.00G2).
f. The interactive and cumulative effects of your treatments. For example, many individuals with immune system disorders receive treatment both for their immune system disorders and for the manifestations of the disorders or co-occurring impairments, such as treatment for HIV infection and hepatitis C. The interactive and cumulative effects of these treatments may be greater than the effects of each treatment considered separately.
g. The duration of your treatment.
h. Any other aspects of treatment that may interfere with your ability to function.
2. Variability of your response to treatment. Your response to treatment and the adverse or beneficial consequences of your treatment may vary widely. The effects of your treatment may be temporary or long term. For example, some individuals may show an initial positive response to a drug or combination of drugs followed by a decrease in effectiveness. When we evaluate your response to treatment and how your treatment may affect you, we consider such factors as disease activity before treatment, requirements for changes in therapeutic regimens, the time required for therapeutic effectiveness of a particular drug or drugs, the limited number of drug combinations that may be available for your impairment(s), and the time-limited efficacy of some drugs. For example, an individual with HIV infection or another immune deficiency disorder who develops pneumonia or tuberculosis may not respond to the same antibiotic regimen used in treating individuals without HIV infection or another immune deficiency disorder, or may not respond to an antibiotic that he or she responded to before. Therefore, we must consider the effects of your treatment on an individual basis, including the effects of your treatment on your ability to function.
3. How we evaluate the effects of treatment for autoimmune disorders on your ability to function. Some medications may have acute or long-term side effects. When we consider the effects of corticosteroids or other treatments for autoimmune disorders on your ability to function, we consider the factors in 14.00G1 and 14.00G2. Long-term corticosteroid treatment can cause ischemic necrosis of bone, posterior subcapsular cataract, weight gain, glucose intolerance, increased susceptibility to infection, and osteoporosis that may result in a loss of function. In addition, medications used in the treatment of autoimmune disorders may also have effects on mental functioning, including cognition (for example, memory), concentration, and mood.
4. How we evaluate the effects of treatment for immune deficiency disorders, excluding HIV infection, on your ability to function. When we consider the effects of your treatment for your immune deficiency disorder on your ability to function, we consider the factors in 14.00G1 and 14.00G2. A frequent need for treatment such as intravenous immunoglobulin and gamma interferon therapy can be intrusive and interfere with your ability to work. We will also consider whether you have chronic side effects from these or other medications, including severe fatigue, fever, headaches, high blood pressure, joint swelling, muscle aches, nausea, shortness of breath, or limitations in mental function including cognition (for example, memory), concentration, and mood.
5. How we evaluate the effects of treatment for HIV infection on your ability to function.
a. General. When we consider the effects of antiretroviral drugs (including the effects of highly active antiretroviral therapy (HAART)) and the effects of treatments for the manifestations of HIV infection on your ability to function, we consider the factors in 14.00G1 and 14.00G2. Side effects of antiretroviral drugs include, but are not limited to: Bone marrow suppression, pancreatitis, gastrointestinal intolerance (nausea, vomiting, diarrhea), neuropathy, rash, hepatotoxicity, lipodystrophy (fat redistribution, such as “buffalo hump”), glucose intolerance, and lactic acidosis. In addition, medications used in the treatment of HIV infection may also have effects on mental functioning, including cognition (for example, memory), concentration, and mood, and may result in malaise, severe fatigue, joint and muscle pain, and insomnia. The symptoms of HIV infection and the side effects of medication may be indistinguishable from each other. We will consider all of your functional limitations, whether they result from your symptoms or signs of HIV infection or the side effects of your treatment.
b. Structured treatment interruptions. A structured treatment interruption (STI, also called a “drug holiday”) is a treatment practice during which your treating source advises you to stop taking your medications temporarily. An STI in itself does not imply that your medical condition has improved; nor does it imply that you are noncompliant with your treatment because you are following your treating source's advice. Therefore, if you have stopped taking medication because your treating source prescribed or recommended an STI, we will not find that you are failing to follow treatment or draw inferences about the severity of your impairment on this fact alone. We will consider why your treating source has prescribed or recommended an STI and all the other information in your case record when we determine the severity of your impairment.
6. When there is no record of ongoing treatment. If you have not received ongoing treatment or have not had an ongoing relationship with the medical community despite the existence of a severe impairment(s), we will evaluate the medical severity and duration of your immune system disorder on the basis of the current objective medical evidence and other evidence in your case record, taking into consideration your medical history, symptoms, clinical and laboratory findings, and medical source opinions. If you have just begun treatment and we cannot determine whether you are disabled based on the evidence we have, we may need to wait to determine the effect of the treatment on your ability to function. The amount of time we need to wait will depend on the facts of your case. If you have not received treatment, you may not be able to show an impairment that meets the criteria of one of the immune system disorders listings, but your immune system disorder may medically equal a listing or be disabling based on a consideration of your residual functional capacity, age, education, and work experience.
H. How do we consider your symptoms, including your pain, severe fatigue, and malaise?
Your symptoms, including pain, severe fatigue, and malaise, may be important factors in our determination whether your immune system disorder(s) meets or medically equals a listing or in our determination whether you are otherwise able to work. In order for us to consider your symptoms, you must have medical signs or laboratory findings showing the existence of a medically determinable impairment(s) that could reasonably be expected to produce the symptoms. If you have such an impairment(s), we will evaluate the intensity, persistence, and functional effects of your symptoms using the rules throughout 14.00 and in our other regulations. See §§ 404.1521, 404.1529, 416.921, and 416.929. Additionally, when we assess the credibility of your complaints about your symptoms and their functional effects, we will not draw any inferences from the fact that you do not receive treatment or that you are not following treatment without considering all of the relevant evidence in your case record, including any explanations you provide that may explain why you are not receiving or following treatment.
I. How do we use the functional criteria in these listings?
1. The following listings in this body system include standards for evaluating the functional limitations resulting from immune system disorders: 14.02B, for systemic lupus erythematosus; 14.03B, for systemic vasculitis; 14.04D, for systemic sclerosis (scleroderma); 14.05E, for polymyositis and dermatomyositis; 14.06B, for undifferentiated and mixed connective tissue disease; 14.07C, for immune deficiency disorders, excluding HIV infection; 14.09D, for inflammatory arthritis; 14.10B, for Sjögren's syndrome; and 14.11I, for HIV infection.
2. When we use one of the listings cited in 14.00I1, we will consider all relevant information in your case record to determine the full impact of your immune system disorder on your ability to function on a sustained basis. Important factors we will consider when we evaluate your functioning under these listings include, but are not limited to: Your symptoms, the frequency and duration of manifestations of your immune system disorder, periods of exacerbation and remission, and the functional impact of your treatment, including the side effects of your medication.
3. As used in these listings, “repeated” means that the manifestations occur on an average of three times a year, or once every 4 months, each lasting 2 weeks or more; or the manifestations do not last for 2 weeks but occur substantially more frequently than three times in a year or once every 4 months; or they occur less frequently than an average of three times a year or once every 4 months but last substantially longer than 2 weeks. Your impairment will satisfy this criterion regardless of whether you have the same kind of manifestation repeatedly, all different manifestations, or any other combination of manifestations; for example, two of the same kind of manifestation and a different one. You must have the required number of manifestations with the frequency and duration required in this section. Also, the manifestations must occur within the period covered by your claim.
4. To satisfy the functional criterion in a listing, your immune system disorder must result in a “marked” level of limitation in one of three general areas of functioning: Activities of daily living, social functioning, or difficulties in completing tasks due to deficiencies in concentration, persistence, or pace. Functional limitation may result from the impact of the disease process itself on your mental functioning, physical functioning, or both your mental and physical functioning. This could result from persistent or intermittent symptoms, such as depression, severe fatigue, or pain, resulting in a limitation of your ability to do a task, to concentrate, to persevere at a task, or to perform the task at an acceptable rate of speed. You may also have limitations because of your treatment and its side effects (see 14.00G).
5. Marked limitation means that the signs and symptoms of your immune system disorder interfere seriously with your ability to function. Although we do not require the use of such a scale, “marked” would be the fourth point on a five-point scale consisting of no limitation, mild limitation, moderate limitation, marked limitation, and extreme limitation. You may have a marked limitation when several activities or functions are impaired, or even when only one is impaired. Also, you need not be totally precluded from performing an activity to have a marked limitation, as long as the degree of limitation seriously interferes with your ability to function independently, appropriately, and effectively. The term “marked” does not imply that you must be confined to bed, hospitalized, or in a nursing home.
6. Activities of daily living include, but are not limited to, such activities as doing household chores, grooming and hygiene, using a post office, taking public transportation, or paying bills. We will find that you have a “marked” limitation of activities of daily living if you have a serious limitation in your ability to maintain a household or take public transportation because of symptoms, such as pain, severe fatigue, anxiety, or difficulty concentrating, caused by your immune system disorder (including manifestations of the disorder) or its treatment, even if you are able to perform some self-care activities.
7. Social functioning includes the capacity to interact independently, appropriately, effectively, and on a sustained basis with others. It includes the ability to communicate effectively with others. We will find that you have a “marked” limitation in maintaining social functioning if you have a serious limitation in social interaction on a sustained basis because of symptoms, such as pain, severe fatigue, anxiety, or difficulty concentrating, or a pattern of exacerbation and remission, caused by your immune system disorder (including manifestations of the disorder) or its treatment, even if you are able to communicate with close friends or relatives.
8. Completing tasks in a timely manner involves the ability to sustain concentration, persistence, or pace to permit timely completion of tasks commonly found in work settings. We will find that you have a “marked” limitation in completing tasks if you have a serious limitation in your ability to sustain concentration or pace adequate to complete work-related tasks because of symptoms, such as pain, severe fatigue, anxiety, or difficulty concentrating, caused by your immune system disorder (including manifestations of the disorder) or its treatment, even if you are able to do some routine activities of daily living.
J. How do we evaluate your immune system disorder when it does not meet one of these listings?
1. These listings are only examples of immune system disorders that we consider severe enough to prevent you from doing any gainful activity. If your impairment(s) does not meet the criteria of any of these listings, we must also consider whether you have an impairment(s) that satisfies the criteria of a listing in another body system.
2. Individuals with immune system disorders, including HIV infection, may manifest signs or symptoms of a mental impairment or of another physical impairment. For example, HIV infection may accelerate the onset of conditions such as diabetes or affect the course of or treatment options for diseases such as cardiovascular disease or hepatitis. We may evaluate these impairments under the affected body system.
3. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. (See §§ 404.1526 and 416.926.) If it does not, you may or may not have the residual functional capacity to engage in substantial gainful activity. Therefore, we proceed to the fourth, and if necessary, the fifth steps of the sequential evaluation process in §§ 404.1520 and 416.920. We use the rules in §§ 404.1594, 416.994, and 416.994a as appropriate, when we decide whether you continue to be disabled.
14.01 Category of Impairments, Immune System Disorders.
14.02 Systemic lupus erythematosus. As described in 14.00D1. With:
A. Involvement of two or more organs/body systems, with:
1. One of the organs/body systems involved to at least a moderate level of severity; and
2. At least two of the constitutional symptoms or signs (severe fatigue, fever, malaise, or involuntary weight loss).
or
B. Repeated manifestations of SLE, with at least two of the constitutional symptoms or signs (severe fatigue, fever, malaise, or involuntary weight loss) and one of the following at the marked level:
1. Limitation of activities of daily living.
2. Limitation in maintaining social functioning.
3. Limitation in completing tasks in a timely manner due to deficiencies in concentration, persistence, or pace.
14.03 Systemic vasculitis. As described in 14.00D2. With:
A. Involvement of two or more organs/body systems, with:
1. One of the organs/body systems involved to at least a moderate level of severity; and
2. At least two of the constitutional symptoms or signs (severe fatigue, fever, malaise, or involuntary weight loss).
or
B. Repeated manifestations of systemic vasculitis, with at least two of the constitutional symptoms or signs (severe fatigue, fever, malaise, or involuntary weight loss) and one of the following at the marked level:
1. Limitation of activities of daily living.
2. Limitation in maintaining social functioning.
3. Limitation in completing tasks in a timely manner due to deficiencies in concentration, persistence, or pace.
14.04 Systemic sclerosis (scleroderma). As described in 14.00D3. With:
A. Involvement of two or more organs/body systems, with:
1. One of the organs/body systems involved to at least a moderate level of severity; and
2. At least two of the constitutional symptoms or signs (severe fatigue, fever, malaise, or involuntary weight loss).
or
B. One of the following:
1. Toe contractures or fixed deformity of one or both feet and medical documentation of at least one of the following:
a. A documented medical need (see 14.00C6) for a walker, bilateral canes, or bilateral crutches (see 1.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 1.00C6e(i)); or
b. An inability to use one upper extremity to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 14.00C7), and a documented medical need (see 14.00C6) for a one-handed, hand-held assistive device (see 1.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 1.00C6e(ii)); or
2. Finger contractures or fixed deformity in both hands and medical documentation of an inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 14.00C7); or
3. Atrophy with irreversible damage in one or both lower extremities and medical documentation of at least one of the following:
a. A documented medical need (see 14.00C6) for a walker, bilateral canes, or bilateral crutches (see 1.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 1.00C6e(i)); or
b. An inability to use one upper extremity to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 14.00C7), and a documented medical need (see 14.00C6) for a one-handed, hand-held assistive device (see 1.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 1.00C6e(ii)); or
4. Atrophy with irreversible damage in both upper extremities and medical documentation of an inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 14.00C7); or
C. Raynaud's phenomenon, characterized by:
1. Gangrene involving at least two extremities; or
2. Ischemia with ulcerations of toes or fingers and medical documentation of at least one of the following:
a. A documented medical need (see 14.00C6) for a walker, bilateral canes, or bilateral crutches (see 1.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 1.00C6e(i)); or
b. An inability to use one upper extremity to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 14.00C7), and a documented medical need (see 14.00C6) for a one-handed, hand-held assistive device (see 1.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 1.00C6e(ii)); or
c. An inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 14.00C7); or
D. Repeated manifestations of systemic sclerosis (scleroderma), with at least two of the constitutional symptoms or signs (severe fatigue, fever, malaise, or involuntary weight loss) and one of the following at the marked level:
1. Limitation of activities of daily living.
2. Limitation in maintaining social functioning.
3. Limitation in completing tasks in a timely manner due to deficiencies in concentration, persistence, or pace.
14.05 Polymyositis and dermatomyositis. As described in 14.00D4. With:
A. Proximal limb-girdle (pelvic or shoulder) muscle weakness and medical documentation of at least one of the following:
1. A documented medical need (see 14.00C6) for a walker, bilateral canes, or bilateral crutches (see 1.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 1.00C6e(i)); or
2. An inability to use one upper extremity to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 14.00C7), and a documented medical need (see 14.00C6) for a one-handed, hand-held assistive device (see 1.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 1.00C6e(ii)); or
3. An inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 14.00C7); or
B. Impaired swallowing (dysphagia) with aspiration due to muscle weakness.
or
C. Impaired respiration due to intercostal and diaphragmatic muscle weakness.
or
D. Diffuse calcinosis with limitation of joint mobility or intestinal motility.
or
E. Repeated manifestations of polymyositis or dermatomyositis, with at least two of the constitutional symptoms or signs (severe fatigue, fever, malaise, or involuntary weight loss) and one of the following at the marked level:
1. Limitation of activities of daily living.
2. Limitation in maintaining social functioning.
3. Limitation in completing tasks in a timely manner due to deficiencies in concentration, persistence, or pace.
14.06 Undifferentiated and mixed connective tissue disease. As described in 14.00D5. With:
A. Involvement of two or more organs/body systems, with:
1. One of the organs/body systems involved to at least a moderate level of severity; and
2. At least two of the constitutional symptoms or signs (severe fatigue, fever, malaise, or involuntary weight loss).
or
B. Repeated manifestations of undifferentiated or mixed connective tissue disease, with at least two of the constitutional symptoms or signs (severe fatigue, fever, malaise, or involuntary weight loss) and one of the following at the marked level:
1. Limitation of activities of daily living.
2. Limitation in maintaining social functioning.
3. Limitation in completing tasks in a timely manner due to deficiencies in concentration, persistence, or pace.
14.07 Immune deficiency disorders, excluding HIV infection. As described in 14.00E. With:
A. One or more of the following infections. The infection(s) must either be resistant to treatment or require hospitalization or intravenous treatment three or more times in a 12-month period.
1. Sepsis; or
2. Meningitis; or
3. Pneumonia; or
4. Septic arthritis; or
5. Endocarditis; or
6. Sinusitis documented by appropriate medically acceptable imaging.
or
B. Stem cell transplantation as described under 14.00E3. Consider under a disability until at least 12 months from the date of transplantation. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
or
C. Repeated manifestations of an immune deficiency disorder, with at least two of the constitutional symptoms or signs (severe fatigue, fever, malaise, or involuntary weight loss) and one of the following at the marked level:
1. Limitation of activities of daily living.
2. Limitation in maintaining social function.
3. Limitation in completing tasks in a timely manner due to deficiencies in concentration, persistence, or pace.
14.08 [Reserved]
14.09 Inflammatory arthritis. As described in 14.00D6. With:
A. Persistent inflammation or persistent deformity of:
1. One or more major joints in a lower extremity (see 14.00C8) and medical documentation of at least one of the following:
a. A documented medical need (see 14.00C6) for a walker, bilateral canes, or bilateral crutches (see 1.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 1.00C6e(i)); or
b. An inability to use one upper extremity to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 14.00C7), and a documented medical need (see 14.00C6) for a one-handed, hand-held assistive device (see 1.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 1.00C6e(ii)); or
2. One or more major joints in each upper extremity (see 14.00C8) and medical documentation of an inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete work-related activities involving fine and gross movements (see 14.00C7); or
B. Inflammation or deformity in one or more major joints of an upper or a lower extremity (see 14.00C8) with:
1. Involvement of two or more organs/body systems with one of the organs/body systems involved to at least a moderate level of severity; and
2. At least two of the constitutional symptoms or signs (severe fatigue, fever, malaise, or involuntary weight loss).
or
C. Ankylosing spondylitis or other spondyloarthropathies, with:
1. Ankylosis (fixation) of the dorsolumbar or cervical spine as shown by appropriate medically acceptable imaging and measured on physical examination at 45° or more of flexion from the vertical position (zero degrees); or
2. Ankylosis (fixation) of the dorsolumbar or cervical spine as shown by appropriate medically acceptable imaging and measured on physical examination at 30° or more of flexion (but less than 45°) measured from the vertical position (zero degrees), and involvement of two or more organs/body systems with one of the organs/body systems involved to at least a moderate level of severity.
or
D. Repeated manifestations of inflammatory arthritis, with at least two of the constitutional symptoms or signs (severe fatigue, fever, malaise, or involuntary weight loss) and one of the following at the marked level:
1. Limitation of activities of daily living.
2. Limitation in maintaining social functioning.
3. Limitation in completing tasks in a timely manner due to deficiencies in concentration, persistence, or pace.
14.10 Sjögren's syndrome. As described in 14.00D7. With:
A. Involvement of two or more organs/body systems, with:
1. One of the organs/body systems involved to at least a moderate level of severity; and
2. At least two of the constitutional symptoms or signs (severe fatigue, fever, malaise, or involuntary weight loss).
or
B. Repeated manifestations of Sjögren's syndrome, with at least two of the constitutional symptoms or signs (severe fatigue, fever, malaise, or involuntary weight loss) and one of the following at the marked level:
1. Limitation of activities of daily living.
2. Limitation in maintaining social functioning.
3. Limitation in completing tasks in a timely manner due to deficiencies in concentration, persistence, or pace.
14.11 Human immunodeficiency virus (HIV) infection. With documentation as described in 14.00F1 and one of the following:
A. Multicentric (not localized or unicentric) Castleman disease affecting multiple groups of lymph nodes or organs containing lymphoid tissue (see 14.00F3a).
OR
B. Primary central nervous system lymphoma (see 14.00F3b).
OR
C. Primary effusion lymphoma (see 14.00F3c).
OR
D. Progressive multifocal leukoencephalopathy (see 14.00F3d).
OR
E. Pulmonary Kaposi sarcoma (see 14.00F3e).
OR
F. Absolute CD4 count of 50 cells/mm3 or less (see 14.00F4).
OR
G. Absolute CD4 count of less than 200 cells/mm3 or CD4 percentage of less than 14 percent, and one of the following (values do not have to be measured on the same date) (see 14.00F5):
1. BMI measurement of less than 18.5; or
2. Hemoglobin measurement of less than 8.0 grams per deciliter (g/dL).
OR
H. Complication(s) of HIV infection requiring at least three hospitalizations within a 12-month period and at least 30 days apart (see 14.00F6). Each hospitalization must last at least 48 hours, including hours in a hospital emergency department immediately before the hospitalization.
OR
I. Repeated (as defined in 14.00I3) manifestations of HIV infection, including those listed in 14.11A-H, but without the requisite findings for those listings (for example, Kaposi sarcoma not meeting the criteria in 14.11E), or other manifestations (including, but not limited to, cardiovascular disease (including myocarditis, pericardial effusion, pericarditis, endocarditis, or pulmonary arteritis), diarrhea, distal sensory polyneuropathy, glucose intolerance, gynecologic conditions (including cervical cancer or pelvic inflammatory disease, see 14.00F7), hepatitis, HIV-associated dementia, immune reconstitution inflammatory syndrome (IRIS), infections (bacterial, fungal, parasitic, or viral), lipodystrophy (lipoatrophy or lipohypertrophy), malnutrition, muscle weakness, myositis, neurocognitive or other mental limitations not meeting the criteria in 12.00, oral hairy leukoplakia, osteoporosis, pancreatitis, peripheral neuropathy) resulting in significant, documented symptoms or signs (for example, but not limited to, fever, headaches, insomnia, involuntary weight loss, malaise, nausea, night sweats, pain, severe fatigue, or vomiting) and one of the following at the marked level:
1. Limitation of activities of daily living.
2. Limitation in maintaining social functioning.
3. Limitation in completing tasks in a timely manner due to deficiencies in concentration, persistence, or pace.
Part B
Medical criteria for the evaluation of impairments of children under age 18 (where criteria in part A do not give appropriate consideration to the particular disease process in childhood).
Sec.
100.00 Low Birth Weight and Failure to Thrive.
101.00 Musculoskeletal Disorders.
102.00 Special Senses and Speech.
103.00 Respiratory Disorders.
104.00 Cardiovascular System.
105.00 Digestive System.
106.00 Genitourinary Disorders.
107.00 Hematological Disorders.
108.00 Skin Disorders
109.00 Endocrine Disorders.
110.00 Congenital Disorders That Affect Multiple Body Systems.
111.00 Neurological Disorders.
112.00 Mental Disorders.
113.00 Cancer (Malignant Neoplastic Diseases)
114.00 Immune System Disorders.
100.00 Low Birth Weight and Failure to Thrive
A. What conditions do we evaluate under these listings? We evaluate low birth weight (LBW) in infants from birth to attainment of age 1 and failure to thrive (FTT) in infants and toddlers from birth to attainment of age 3.
B. How do we evaluate disability based on LBW under 100.04? In 100.04A and 100.04B, we use an infant's birth weight as documented by an original or certified copy of the infant's birth certificate or by a medical record signed by a physician. Birth weight means the first weight recorded after birth. In 100.04B, gestational age is the infant's age based on the date of conception as recorded in the medical record. If the infant's impairment meets the requirements for listing 100.04A or 100.04B, we will follow the rule in § 416.990(b)(11) of this chapter.
C. How do we evaluate disability based on FTT under 100.05?
1. General. We establish FTT with or without a known cause when we have documentation of an infant's or a toddler's growth failure and developmental delay from an acceptable medical source(s) as defined in § 416.913(a) of this chapter. We require documentation of growth measurements in 100.05A and developmental delay described in 100.05B or 100.05C within the same consecutive 12-month period. The dates of developmental testing and reports may be different from the dates of growth measurements. After the attainment of age 3, we evaluate growth failure under the affected body system(s).
2. Growth failure. Under 100.05A, we use the appropriate table(s) under 105.08B in the digestive system to determine whether a child's growth is less than the third percentile. The child does not need to have a digestive disorder for purposes of 100.05.
a. For children from birth to attainment of age 2, we use the weight-for-length table corresponding to the child's gender (Table I or Table II).
b. For children age 2 to attainment of age 3, we use the body mass index (BMI)-for-age table corresponding to the child's gender (Table III or Table IV).
c. BMI is the ratio of a child's weight to the square of his or her height. We calculate BMI using the formulas in 105.00G2c.
d. Growth measurements. The weight-for-length measurements for children from birth to the attainment of age 2 and BMI-for-age measurements for children age 2 to attainment of age 3 that are required for this listing must be obtained within a 12-month period and at least 60 days apart. If a child attains age 2 during the evaluation period, additional measurements are not needed. Any measurements taken before the child attains age 2 can be used to evaluate the impairment under the appropriate listing for the child's age. If the child attains age 3 during the evaluation period, the measurements can be used to evaluate the impairment in the affected body system.
3. Developmental delay.
a. Under 100.05B and C, we use reports from acceptable medical sources to establish delay in a child's development.
b. Under 100.05B, we document the severity of developmental delay with results from a standardized developmental assessment, which compares a child's level of development to the level typically expected for his or her chronological age. If the child was born prematurely, we may use the corrected chronological age (CCA) for comparison. (See § 416.924b(b) of this chapter.) CCA is the chronological age adjusted by a period of gestational prematurity. CCA = (chronological age) - (number of weeks premature). Acceptable medical sources or early intervention specialists, physical or occupational therapists, and other sources may conduct standardized developmental assessments and developmental screenings. The results of these tests and screenings must be accompanied by a statement or records from an acceptable medical source who established the child has a developmental delay.
c. Under 100.05C, when there are no results from a standardized developmental assessment in the case record, we need narrative developmental reports from the child's medical sources in sufficient detail to assess the severity of his or her developmental delay. A narrative developmental report is based on clinical observations, progress notes, and well-baby check-ups. To meet the requirements for 100.05C, the report must include: The child's developmental history; examination findings (with abnormal findings noted on repeated examinations); and an overall assessment of the child's development (that is, more than one or two isolated skills) by the medical source. Some narrative developmental reports may include results from developmental screening tests, which can identify a child who is not developing or achieving skills within expected timeframes. Although medical sources may refer to screening test results as supporting evidence in the narrative developmental report, screening test results alone cannot establish a diagnosis or the severity of developmental delay.
D. How do we evaluate disorders that do not meet one of these listings?
1. We may find infants disabled due to other disorders when their birth weights are greater than 1200 grams but less than 2000 grams and their weight and gestational age do not meet listing 100.04. The most common disorders of prematurity and LBW include retinopathy of prematurity (ROP), chronic lung disease of infancy (CLD, previously known as bronchopulmonary dysplasia, or BPD), intraventricular hemorrhage (IVH), necrotizing enterocolitis (NEC), and periventricular leukomalacia (PVL). Other disorders include poor nutrition and growth failure, hearing disorders, seizure disorders, cerebral palsy, and developmental disorders. We evaluate these disorders under the affected body systems.
2. We may evaluate infants and toddlers with growth failure that is associated with a known medical disorder under the body system of that medical disorder, for example, the respiratory or digestive body systems.
3. If an infant or toddler has a severe medically determinable impairment(s) that does not meet the criteria of any listing, we must also consider whether the child has an impairment(s) that medically equals a listing (see § 416.926 of this chapter). If the child's impairment(s) does not meet or medically equal a listing, we will determine whether the child's impairment(s) functionally equals the listings (see § 416.926a of this chapter) considering the factors in § 416.924a of this chapter. We use the rule in § 416.994a of this chapter when we decide whether a child continues to be disabled.
100.01 Category of Impairments, Low Birth Weight and Failure to Thrive
100.04 Low birth weight in infants from birth to attainment of age 1.
A. Birth weight (see 100.00B) of less than 1200 grams.
OR
B. The following gestational age and birth weight:
| Gestational age
(in weeks) | Birth weight |
|---|---|
| 37-40 | 2000 grams or less. |
| 36 | 1875 grams or less. |
| 35 | 1700 grams or less. |
| 34 | 1500 grams or less. |
| 33 | 1325 grams or less. |
| 32 | 1250 grams or less. |
100.05 Failure to thrive in children from birth to attainment of age 3 (see 100.00C), documented by A and B, or A and C.
A. Growth failure as required in 1 or 2:
1. For children from birth to attainment of age 2, three weight-for-length measurements that are:
a. Within a consecutive 12-month period; and
b. At least 60 days apart; and
c. Less than the third percentile on the appropriate weight-for-length table in listing 105.08B1; or
2. For children age 2 to attainment of age 3, three BMI-for-age measurements that are:
a. Within a consecutive 12-month period; and
b. At least 60 days apart; and
c. Less than the third percentile on the appropriate BMI-for-age table in listing 105.08B2.
AND
B. Developmental delay (see 100.00C1 and C3), established by an acceptable medical source and documented by findings from one current report of a standardized developmental assessment (see 100.00C3b) that:
1. Shows development not more than two-thirds of the level typically expected for the child's age; or
2. Results in a valid score that is at least two standard deviations below the mean.
OR
C. Developmental delay (see 100.00C3), established by an acceptable medical source and documented by findings from two narrative developmental reports (see 100.00C3c) that:
1. Are dated at least 120 days apart (see 100.00C1); and
2. Indicate current development not more than two-thirds of the level typically expected for the child's age.
101.00 Musculoskeletal Disorders
A. Which musculoskeletal disorders do we evaluate under these listings?
1. We evaluate disorders of the skeletal spine (vertebral column) or of the upper or lower extremities that affect musculoskeletal functioning under these listings. We use the term “skeletal” when we are referring to the structure of the bony skeleton. The skeletal spine refers to the bony structures, ligaments, and discs making up the spine. We refer to the skeletal spine in some musculoskeletal listings to differentiate it from the neurological spine (see 101.00B1). Musculoskeletal disorders may be congenital or acquired, and may include deformities, amputations, or other abnormalities. These disorders may involve the bones or major joints; or the tendons, ligaments, muscles, or other soft tissues.
2. We evaluate soft tissue injuries (including burns) or abnormalities that are under continuing surgical management (see 101.00P1). The injuries or abnormalities may affect any part of the body, including the face and skull.
3. We evaluate curvatures of the skeletal spine that affect musculoskeletal functioning under 101.15. If a curvature of the skeletal spine is under continuing surgical management (see 101.00P1), we will evaluate it under 101.21 using our rules for determining medical equivalence. See § 416.926 of this chapter.
B. Which related disorders do we evaluate under other listings?
1. We evaluate a disorder or injury of the skeletal spine that results in damage to, and neurological dysfunction of, the spinal cord and its associated nerves (for example, paraplegia or quadriplegia) under the listings in 111.00.
2. We evaluate inflammatory arthritis (for example, rheumatoid arthritis) under the listings in 114.00.
3. We evaluate curvatures of the skeletal spine that interfere with your ability to breathe under the listings in 103.00, impair myocardial function under the listings in 104.00, or result in social withdrawal or depression under the listings in 112.00.
4. We evaluate non-healing or pathological fractures due to cancer, whether it is a primary site or metastases, under the listings in 113.00.
5. We evaluate the leg pain associated with peripheral vascular claudication under the listings in 104.00.
6. We evaluate burns that do not require continuing surgical management under the listings in 108.00.
C. What evidence do we need to evaluate your musculoskeletal disorder?
1. General. We need objective medical evidence from an acceptable medical source to establish that you have a medically determinable musculoskeletal disorder. We also need evidence from both medical and nonmedical sources, who can describe how you function, to assess the severity and duration of your musculoskeletal disorder. We will determine the extent and kinds of evidence we need from medical and nonmedical sources based on the individual facts about your disorder. For our basic rules on evidence, see §§ 416.912, 416.913, and 416.920b of this chapter. For our rules on evidence about your symptoms, see § 416.929 of this chapter.
2. Physical examination report(s). In the report(s) of your physical examination, we require a medical source's detailed description of the orthopedic, neurologic, or other objective clinical findings appropriate to your specific musculoskeletal disorder from his or her direct observations during your physical examination. We will not accept a report of your statements about your symptoms and limitations in place of the medical source's report of objective clinical findings. We will not use findings on imaging or other diagnostic tests (see 101.00C3) as a substitute for findings on physical examination.
a. When the medical source reports that a clinical test sign(s) is positive, unless we have evidence to the contrary, we will assume that he or she performed the test properly and accept the medical source's interpretation of the test. For example, we will assume a straight-leg raising test was conducted properly (that is, in sitting and supine positions), even if the medical source does not specify the positions in which the test was performed.
b. If you use an assistive device (see 101.00C6), the report must support the medical need for the device.
c. If your musculoskeletal disorder causes a reduction in muscle strength, the report must document measurement of the strength of the muscle(s) in question. The measurement should be based on a muscle strength grading system that is considered medically acceptable based on your age and impairments. For example, a grading system of 0 to 5, with 0 indicating complete loss of strength and 5 indicating maximum strength or equivalent medically acceptable scale (see Table 1). Reduction in muscle strength is demonstrated by evidence that your muscle strength is less than active range of motion (ROM) against gravity with maximum resistance. If the reduction in muscle strength involves one or both of your hands, the report must also document measurements of grip and pinch strength.
Table 1 - Grading System of Muscle Function
| Grade | Function of the muscle |
|---|---|
| 0 - None | No visible or palpable contraction. |
| 1 - Trace | Visible or palpable contraction with no motion. |
| 2 - Poor | Active ROM with gravity eliminated. |
| 3 - Fair | Active ROM against gravity only, without resistance. |
| 4 - Good | Active ROM against gravity, moderate resistance. |
| 5 - Normal | Active ROM against gravity, maximum resistance. |
3. Imaging and other diagnostic tests.
a. Imaging refers to medical imaging techniques, such as x-ray, computed tomography (CT), magnetic resonance imaging (MRI), and radionuclide scanning. For the purpose of these listings, the imaging must be consistent with the prevailing state of medical knowledge and clinical practice as the proper technique to support the evaluation of the disorder.
b. Findings on imaging must have lasted, or be expected to last, for a continuous period of at least 12 months.
c. Imaging and other diagnostic tests can provide evidence of physical abnormalities; however, these abnormalities may correlate poorly with your symptoms, including pain, or with your musculoskeletal functioning. Accordingly, we will not use findings on imaging or other diagnostic tests as a substitute for findings on physical examination about your ability to function, nor can we infer severity or functional limitations based solely on such tests.
d. For our rules on purchasing imaging and other diagnostic tests, see §§ 416.919k and 416.919m of this chapter.
4. Operative reports. If you have had a surgical procedure, we need a copy of the operative report, including details of the findings at surgery and information about any medical complications that may have occurred. If we do not have the operative report, we need confirmatory evidence of the surgical procedure from a medical source (for example, detailed follow-up reports or notations in the medical records concerning the surgical procedure in your medical history).
5. Effects of treatment.
a. General. Treatments for musculoskeletal disorders may have beneficial or adverse effects, and responses to treatment vary from person to person. We will evaluate all of the effects of treatment (including surgical treatment, medications, and therapy) on the symptoms, signs, and laboratory findings of your musculoskeletal disorder, and on your musculoskeletal functioning.
b. Response to treatment. To evaluate your musculoskeletal functioning in response to treatment, we need the following: A description, including the frequency of the administration, of your medications; the type and frequency of therapy you receive; and a description of your response to treatment and any complications you experience related to your musculoskeletal disorder. The effects of treatment may be temporary or long-term. We need information over a sufficient period to determine the effects of treatment on your current musculoskeletal functioning and permit reasonable projections about your future functioning. We will determine the amount of time that constitutes a sufficient period in consultation with a medical consultant on a case by case basis. In some cases, we will need additional evidence to make an assessment about your response to treatment. Your musculoskeletal disorder may meet or medically equal one of these listings regardless of whether you were prescribed opioid medication, or whether you were prescribed opioid medication and did not follow this prescribed treatment.
6. Assistive devices.
a. General. An assistive device, for the purposes of these listings, is any device that you use to improve your stability, dexterity, or mobility. An assistive device can be worn (see 101.00C6b and 101.00C6c), hand-held (see 101.00C6d), or used in a seated position (see 101.00C6e). When we use the phrase “documented medical need,” we mean that there is evidence from a medical source that supports your medical need for an assistive device (see 101.00C2b) for a continuous period of at least 12 months (see 101.00c2a). This evidence must describe any limitation(s) in your upper or lower extremity functioning and the circumstances for which you need to use the assistive device. We do not require that you have a specific prescription for the assistive device.
b. Prosthesis(es). A prosthesis is a wearable device, such as an artificial limb, that takes the place of an absent body part. If you have a prosthesis(es), we need evidence from a medical source documenting your ability to walk, or perform fine and gross movements (see 101.00E4), with the prosthesis(es) in place. When amputation(s) involves one or both lower extremities, it is not necessary for the medical source to evaluate your ability to walk without the prosthesis(es) in place. If you cannot use your prosthesis(es) due to complications affecting your residual limb(s), we need evidence from a medical source documenting the condition of your residual limb(s) and the medical basis for your inability to use the device(s).
c. Orthosis(es). An orthosis is a wearable device, such as a brace, that prevents or corrects a dysfunction or deformity by aligning or supporting the affected body part. If you have an orthosis(es), we need evidence from a medical source documenting your ability to walk, or perform fine and gross movements (see 101.00E4), with the orthosis(es) in place. If you cannot use your orthosis(es), we need evidence from a medical source documenting the medical basis for your inability to use the device(s).
d. Hand-held assistive devices. Hand-held assistive devices include walkers, canes, or crutches, which you hold onto with your hand(s) to support or aid you in walking. When you use a one-handed, hand-held assistive device (such as a cane) with one upper extremity to walk and you cannot use your other upper extremity for fine or gross movements (see 101.00E4), the need for the assistive device limits the use of both upper extremities. If you use a hand-held assistive device, we need evidence from a medical source describing how you walk with the device.
e. Wheeled and seated mobility devices. Wheeled and seated mobility devices are assistive devices that you use in a seated position, such as manual wheelchairs, motorized wheelchairs, rollators, and power operated vehicles. If you use a wheeled and seated mobility device, we need evidence from a medical source describing the type of wheeled and seated mobility device that you use and how you use the assistive device, including any customizations or modifications to the assistive device itself or for your use of the assistive device. For example, if you use a wheelchair that typically requires the use of both hands but has been customized for your use with one hand, then we will evaluate your use of the assistive device using the criteria in 101.00E3b and not 101.00E3a.
(i) Wheeled and seated mobility devices involving the use of both hands. Some wheeled and seated mobility devices involve the use of both hands to use the assistive device (for example, most manual wheelchairs). If you use a wheeled and seated mobility device that involves the use of both hands, then the need for the assistive device limits the use of both upper extremities.
(ii) Wheeled and seated devices involving the use of one hand. Some wheeled and seated mobility devices involve the use of one hand to use the assistive device (for example, most motorized wheelchairs). If you use a wheeled and seated mobility device that involves the use of one upper extremity and you cannot use your other upper extremity for fine or gross movements (see 101.00E4), then the need for the assistive device limits the use of both upper extremities.
7. Longitudinal evidence.
a. The term pandemic period as used in 1.00C7c means the period beginning on April 2, 2021, and ending on the date that is 6 months after the effective date of a determination by the Secretary of Health and Human Services under section 319 of the Public Health Service Act, 42 U.S.C. 247d, that the national public health emergency resulting from the COVID-19 pandemic no longer exists.
b. We generally need a longitudinal medical record to assess the severity and duration of your musculoskeletal disorder because the severity of symptoms, signs, and laboratory findings related to most musculoskeletal disorders may improve over time or respond to treatment. Evidence over an extended period will show whether your musculoskeletal functioning is improving, worsening, or unchanging.
c. For 1.15, 1.16, 1.17, 1.18, 1.20C, 1.20D, 1.22, and 1.23, all of the required criteria must be present simultaneously, or within a close proximity of time, to satisfy the level of severity needed to meet the listing. The phrase “within a close proximity of time” means that all of the relevant criteria must appear in the medical record within a consecutive 4-month period, except for claims determined or decided during the pandemic period. For claims determined or decided during the pandemic period, all of the relevant criteria must appear in the medical record within a consecutive 12-month period. When the criterion is imaging, we mean that we could reasonably expect the findings on imaging to have been present at the date of impairment or date of onset. For listings that use the word “and” to link the elements of the required criteria, the medical record must establish the simultaneous presence, or presence within a close proximity of time, of all the required medical criteria. Once this level of severity is established, the medical record must also show that this level of severity has continued, or is expected to continue, for a continuous period of at least 12 months.
8. Surgical treatment or physical therapy. For some musculoskeletal disorders, a medical source may recommend surgery, or physical therapy (PT). If you have not yet had the recommended surgery or PT, we will not assume that these interventions will resolve your disorder or improve your functioning. We will assess each case on an individual basis. Depending on your response to treatment, or your medical sources' treatment plans, we may defer our findings regarding the effect of surgery or PT, until a sufficient period has passed to permit proper consideration or judgment about your future functioning. When necessary, we will follow the rules on following prescribed treatment in § 416.930 of this chapter, including consideration of your reasons for failure to follow prescribed treatment.
D. How do we consider symptoms, including pain, under these listings?
1. Musculoskeletal disorders may cause pain or other symptoms; however, your statements about your pain or other symptoms will not alone establish that you are disabled. We will not substitute an alleged or a reported increase in the intensity of a symptom, such as pain, no matter how severe, for a medical sign or diagnostic finding present in the listing criteria. Pain is included as just one consideration in 101.15A, 101.16A, and 101.18A, but it is not required to satisfy the criteria in 101.15, 101.16, and 101.18.
2. To consider your symptom(s), we require objective medical evidence from an acceptable medical source showing the existence of a medically determinable musculoskeletal impairment that we could reasonably expect to produce the symptom(s). See § 416.929 of this chapter for how we evaluate symptoms, including pain, related to your musculoskeletal disorder.
E. How do we use the functional criteria to evaluate your musculoskeletal disorder under these listings?
1. General. The functional criteria for children age 3 and older are based on impairment-related physical limitations in your ability to use both upper extremities, one or both lower extremities, or a combination of one upper and one lower extremity. We will use the relevant evidence that we have to compare your musculoskeletal functioning to the functioning of children your age who do not have impairments. The required impairment-related physical limitation of musculoskeletal functioning must have lasted, or be expected to last, for a continuous period of at least 12 months. We do not use the functional criteria in 101.20A, 101.20B, 101.21, or 101.24.
2. Medical and functional criteria, birth to attainment of age 3. The medical and functional criteria for children in this age group are in 101.24.
3. Functional criteria, age 3 to attainment of age 18. The functional criteria are based on impairment-related physical limitations in your ability to use both upper extremities, one or both lower extremities, or a combination of one upper and one lower extremity. A musculoskeletal disorder satisfies the functional criteria of a listing when the medical documentation shows the presence of at least one of the impairment-related limitations cited in the listing. The functional criteria require impairment-related physical limitation of musculoskeletal functioning that has lasted, or can be expected to last, for a continuous period of at least 12 months, medically documented by one of the following:
a. A documented medical need (see 101.00C6a) for a walker, bilateral canes, or bilateral crutches (see 101.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 101.00C6e(i));
b. An inability to use one upper extremity to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 101.00E4), and a documented medical need (see 101.00C6a) for a one-handed, hand-held assistive device (see 101.00C6d) that requires the use of your other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 101.00C6e(ii));
c. An inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 101.00E4).
4. Fine and gross movements. Fine movements, for the purposes of these listings, involve use of your wrists, hands, and fingers; such movements include picking, pinching, manipulating, and fingering. Gross movements involve use of your shoulders, upper arms, forearms, and hands; such movements include handling, gripping, grasping, holding, turning, and reaching. Gross movements also include exertional abilities such as lifting, carrying, pushing, and pulling.
F. What do we consider when we evaluate disorders of the skeletal spine resulting in compromise of a nerve root(s) (101.15)?
1. General. We consider musculoskeletal disorders such as skeletal dysplasias, caudal regression syndrome, tethered spinal cord syndrome, vertebral slippage (spondylolisthesis), scoliosis, and vertebral fracture or dislocation. Spinal disorders may cause cervical or lumbar spine dysfunction when abnormalities of the skeletal spine compromise nerve roots of the cervical spine, a nerve root of the lumbar spine, or a nerve root of both cervical and lumbar spines. We consider spinal nerve disorders that originate in the nervous system (for example, spinal arachnoiditis), under the neurological disorders body system, 111.00.
2. Compromise of a nerve root(s). Compromise of a nerve root, sometimes referred to as “nerve root impingement,” is a phrase used when a physical object, such as a tumor, herniated disc, foreign body, or arthritic spur, is pushing on the nerve root as seen on imaging or during surgery. It can occur when a musculoskeletal disorder produces irritation, inflammation, or compression of the nerve root(s) as it exits the skeletal spine between the vertebrae. Related symptoms must be associated with, or follow the path of, the affected nerve root(s).
a. Compromise of unilateral nerve root of the cervical spine. Compromise of a nerve root as it exits the cervical spine between the vertebrae may affect the functioning of the associated upper extremity. The physical examination reproduces the related symptoms based on radicular signs and clinical tests appropriate to the specific cervical nerve root (for example, a positive Spurling test).
b. Compromise of bilateral nerve roots of the cervical spine. Although uncommon, if compromise of a nerve root occurs on both sides of the cervical spinal column, functioning of both upper extremities may be limited.
c. Compromise of a nerve root(s) of the lumbar spine. Compromise of a nerve root as it exits the lumbar spine between the vertebrae may limit the functioning of the associated lower extremity. The physical examination reproduces the related symptoms based on radicular signs and clinical tests. When a nerve root of the lumbar spine is compromised, we require a positive straight-leg raising test (also known as a Lasègue test) in both supine and sitting positions appropriate to the specific lumbar nerve root that is compromised.
G. What do we consider when we evaluate lumbar spinal stenosis resulting in compromise of the cauda equina (101.16)?
1. General. We consider how pain, sensory changes, and muscle weakness caused by compromise of the cauda equina due to lumbar spinal stenosis affect your functioning. The cauda equina is a bundle of nerve roots that descends from the lower part of the spinal cord. Lumbar spinal stenosis can compress the nerves of the cauda equina, causing sensory changes and muscle weakness that may affect your ability to stand or walk. Pain related to compromise of the cauda equina is nonradicular because it is not typically associated with a specific nerve root (as is radicular pain in the cervical or lumbar spine).
2. Compromise of the cauda equina due to lumbar spinal stenosis can affect your ability to walk or stand because of neurogenic claudication (also known as pseudoclaudication), a condition usually causing nonradicular pain that starts in the low back and radiates bilaterally (or less commonly, unilaterally) into the buttocks and lower extremities (or extremity). Extension of the lumbar spine, which occurs when you walk or stand, may provoke the pain of neurogenic claudication. The pain may be relieved by forward flexion of the lumbar spine or by sitting. In contrast, the leg pain associated with peripheral vascular claudication results from inadequate arterial blood flow to a lower extremity. It occurs repeatedly and consistently when a person walks a certain distance and is relieved when the person rests.
H. What do we consider when we evaluate reconstructive surgery or surgical arthrodesis of a major weight-bearing joint (101.17)?
1. General. We consider reconstructive surgery or surgical arthrodesis when an acceptable medical source(s) documents the surgical procedure(s) and associated medical treatments to restore function of, or eliminate motion in, the affected major weight-bearing joint(s). Reconstructive surgery may be done in a single procedure or a series of procedures directed toward the salvage or restoration of functional use of the affected joint.
2. Major weight-bearing joints are the hip, knee, and ankle-foot. The ankle and foot are considered together as one major joint.
3. Surgical arthrodesis is the artificial fusion of the bones that form a joint, essentially eliminating the joint.
I. What do we consider when we evaluate abnormality of a major joint(s) in any extremity (101.18)?
1. General. We consider musculoskeletal disorders that produce anatomical abnormalities of major joints of the extremities, which result in functional abnormalities in the upper or lower extremities (for example, chronic infections of bones and joints, and surgical arthrodesis of a joint). Abnormalities of the joints include ligamentous laxity or rupture, soft tissue contracture, or tendon rupture, and can cause muscle weakness of the affected joint(s).
a. An anatomical abnormality is one that is readily observable by a medical source during a physical examination (for example, subluxation or contracture), or is present on imaging (for example, joint space narrowing, bony destruction, ankylosis, or deformity).
b. A functional abnormality is abnormal motion or instability of the affected joint(s), including limitation of motion, excessive motion (hypermobility), movement outside the normal plane of motion for the joint (for example, lateral deviation), or fixation of the affected joint(s).
2. Major joint of an upper extremity refers to the shoulder, elbow, and wrist-hand. We consider the wrist and hand together as one major joint.
3. Major joint of a lower extremity refers to the hip, knee, and ankle-foot. We consider the ankle and hindfoot together as one major joint.
J. What do we consider when we evaluate pathologic fractures due to any cause (101.19)? We consider pathologic fractures of the bones in the skeletal spine, extremities, or other parts of the skeletal system. Pathologic fractures result from disorders that weaken the bones, making them vulnerable to breakage. Pathologic fractures may occur with osteoporosis, osteogenesis imperfecta or any other skeletal dysplasias, side effects of medications, and disorders of the endocrine or other body systems. Under 101.19, the fractures must have occurred on separate, distinct occasions, rather than multiple fractures occurring at the same time, but the fractures may affect the same bone(s) multiple times. There is no required time that must elapse between the fractures, but all three must occur within a 12-month period; for example, separate incidents may occur within hours or days of each other. We evaluate non-healing or complex traumatic fractures without accompanying pathology under 101.22 or 101.23.
K. What do we consider when we evaluate amputation due to any cause (101.20)?
1. General. We consider amputation (the full or partial loss or absence of any extremity) due to any cause including trauma, congenital abnormality or absence, surgery for treatment of conditions such as cancer or infection, or complications of peripheral vascular disease or diabetes mellitus.
2. Amputation of both upper extremities (101.20A). Under 101.20A, we consider upper extremity amputations that occur at any level at or above the wrists (carpal joints), up to and including disarticulation of the shoulder (glenohumeral) joint. If you have had both upper extremities amputated at any level at or above the wrists up to and including the shoulder, your impairment satisfies the duration requirement in § 416.909 of this chapter. For amputations below the wrist, we will follow the rules described in 101.00R. We do not evaluate amputations below the wrists under 101.20A because the resulting limitation of function of the thumb(s), finger(s), or hand(s) will vary, depending on the extent of loss and corresponding effect on fine and gross movements.
3. Hemipelvectomy or hip disarticulation (101.20B). Under 101.20B, we consider hemipelvectomy, which involves amputation of an entire lower extremity through the sacroiliac joint, and hip disarticulation, which involves amputation of an entire lower extremity through the hip joint capsule and closure of the remaining musculature over the exposed acetabular bone. If you have had a hemipelvectomy or hip disarticulation, your impairment satisfies the duration requirement in § 416.909 of this chapter.
4. Amputation of one upper extremity and one lower extremity (101.20C). Under 101.20C, we consider the amputation of one upper extremity at any level at or above the wrist and one lower extremity at or above the ankle. If you have a documented medical need for a one-handed, hand-held assistive device (such as a cane) or a wheeled and seated mobility device involving the use of one hand (such as a motorized wheelchair), then you must use your remaining upper extremity to hold the device, making the extremity unavailable to perform other fine and gross movements (see 101.00E4).
5. Amputation of one lower extremity or both lower extremities with complications of the residual limb(s) (101.20D). Under 101.20D, we consider the amputation of one lower extremity or both lower extremities at or above the ankle. We also consider the condition of your residual limb(s), whether you can wear a prosthesis(es) (see 101.00C6b), and whether you have a documented medical need (see 101.00C6a) for a hand-held assistive device(s) (see 101.00C6d) or a wheeled and seated mobility device (see 101.00C6e). If you have a non-healing residual limb(s) and are receiving ongoing surgical treatment expected to re-establish or improve function, and that ongoing surgical treatment has not ended, or is not expected to end, within at least 12 months of the initiation of the surgical management (see 101.00L), we evaluate your musculoskeletal disorder under 101.21.
L. What do we consider when we evaluate soft tissue injury or abnormality under continuing surgical management (101.21)?
1. General.
a. We consider any soft tissue injury or abnormality involving the soft tissues of the body, whether congenital or acquired, when an acceptable medical source(s) documents the need for ongoing surgical procedures and associated medical treatments to restore function of the affected body part(s) (see 101.00P1). Surgical management includes the surgery(ies) itself, as well as various post-surgical procedures, surgical complications, infections or other medical complications, related illnesses, or related treatments that delay your attainment of maximum benefit from therapy (see 101.00P2).
b. Surgical procedures and associated treatments typically take place over extended periods, which may render you unable to perform age-appropriate activity on a sustained basis. To document such inability, we must have evidence from an acceptable medical source(s) confirming that the surgical management has continued, or is expected to continue, for at least 12 months from the date of the first surgical intervention. These procedures and treatments must be directed toward saving, reconstructing, or replacing the affected part of the body to re-establish or improve its function, and not for cosmetic appearances alone.
c. Examples include malformations, third- and fourth-degree burns, crush injuries, craniofacial injuries, avulsive injuries, and amputations with complications of the residual limb(s).
d. We evaluate skeletal spine abnormalities or injuries under 101.15 or 101.16, as appropriate. We evaluate abnormalities or injuries of bones in the lower extremities under 101.17, 101.18, or 101.22. We evaluate abnormalities or injuries of bones in the upper extremities under 101.18 or 101.23.
2. Documentation. In addition to the objective medical evidence we need to establish your soft tissue injury or abnormality, we also need all of the following medically documented evidence about your continuing surgical management:
a. Operative reports and related laboratory findings;
b. Records of post-surgical procedures;
c. Records of any surgical or medical complications (for example, related infections or systemic illnesses);
d. Records of any prolonged post-operative recovery periods and related treatments (for example, surgeries and treatments for burns);
e. An acceptable medical source's plans for additional surgeries; and
f. Records detailing any other factors that have delayed, or that an acceptable medical source expects to delay, the saving, restoring, or replacing of the involved part for a continuous period of at least 12 months following the initiation of the surgical management.
3. Burns. Third- and fourth-degree burns damage or destroy nerve tissue, reducing or preventing transmission of signals through those nerves. Such burns frequently require multiple surgical procedures and related therapies to re-establish or improve function, which we evaluate under 101.21. When burns are no longer under continuing surgical management (see 101.00P1), we evaluate the residual impairment(s). When the residual impairment(s) affects the musculoskeletal system, as often occurs in third- and fourth-degree burns, it can result in permanent musculoskeletal tissue loss, joint contractures, or loss of extremities. We will evaluate such impairments under the relevant musculoskeletal disorders listing, for example, 101.18 or 101.20. When the residual impairment(s) involves another body system, we will evaluate the impairment(s) under the listings in the relevant body system(s).
4. Craniofacial injuries or congenital abnormalities. Surgeons may treat craniofacial injuries or congenital abnormalities with multiple surgical procedures. These injuries or abnormalities may affect vision, hearing, speech, and the initiation of the digestive process, including mastication. When the craniofacial injury-related or congenital abnormality-related residual impairment(s) involves another body system(s), we will evaluate the impairment(s) under the listings in the relevant body system(s).
M. What do we consider when we evaluate non-healing or complex fractures of the femur, tibia, pelvis, or one or more of the talocrural bones (101.22)?
1. Non-healing fracture. A non-healing (nonunion) fracture is a fracture that has failed to unite completely. Nonunion is usually established when a minimum of 9 months has elapsed since the injury and the fracture site has shown no, or minimal, progressive signs of healing for a minimum of 3 months.
2. Complex fracture. A complex fracture is a fracture with one or more of the following:
a. Comminuted (broken into many pieces) bone fragments;
b. Multiple fractures in a single bone;
c. Bone loss due to severe trauma;
d. Damage to the surrounding soft tissue;
e. Severe cartilage damage to the associated joint; or
f. Dislocation of the associated joint.
3. When a complex fracture involves soft tissue damage, the treatment may involve continuing surgical management to restore or improve functioning. In such cases, we may evaluate the fracture(s) under 101.21.
N. What do we consider when we evaluate non-healing or complex fractures of an upper extremity (101.23)?
1. Non-healing fracture. A non-healing (nonunion) fracture is a fracture that has failed to unite completely. Nonunion is usually established when a minimum of 9 months has elapsed since the injury and the fracture site has shown no, or minimal, progressive signs of healing for a minimum of 3 months.
2. Complex fracture. A complex fracture is a fracture with one or more of the following:
a. Comminuted (broken into many pieces) bone fragments;
b. Multiple fractures in a single bone;
c. Bone loss due to severe trauma;
d. Damage to the surrounding soft tissue;
e. Severe cartilage damage to the associated joint; or
f. Dislocation of the associated joint.
3. When a complex fracture involves soft tissue damage, the treatment may involve continuing surgical management to restore or improve functioning. In such cases, we may evaluate the fracture(s) under 101.21.
O. What do we consider when we evaluate musculoskeletal disorders of infants and toddlers from birth to attainment of age 3 with developmental motor delay (101.24)?
1. General. Under 101.24, we require reports from an acceptable medical source(s) to establish a delay in your motor development as a medically determinable impairment. Examples of disorders we evaluate under this listing include arthrogryposis, clubfoot, osteogenesis imperfecta, caudal regression syndrome, fracture complications, disorders affecting the hip and pelvis, and complications associated with your musculoskeletal disorder or its treatment. Some medical records may simply document your condition as “developmental motor delay.”
2. Severity of developmental motor delay. To evaluate the severity of your developmental motor delay, we need developmental test reports from an acceptable medical source, or from early intervention specialists, physical and occupational therapists, and other sources.
a. If there is a standardized developmental assessment in your medical record, we will use the results to evaluate your developmental motor delay under 101.24A. Such an assessment compares your level of development to the level typically expected for children of your chronological age. If you were born prematurely, we use your corrected chronological age for comparison. See § 416.924b(b) of this chapter.
b. If there is no standardized developmental assessment in your medical record, we will use narrative developmental reports from a medical source(s) to evaluate your developmental motor delay under 101.24B. These reports must provide detailed information sufficient for us to assess the severity of your motor delay. If we cannot obtain sufficient detail from narrative reports, we may purchase standardized developmental assessments.
(i) A narrative developmental report is based on clinical observations, progress notes, and well-baby check-ups, and must include your developmental history, examination findings (with abnormal findings noted on repeated examinations), and an overall assessment of your development (that is, more than one or two isolated skills) by the medical source.
(ii) Some narrative developmental reports may include results from developmental screening tests, which can show that you are not developing or achieving skills within expected timeframes. Although medical sources may refer to screening test results as supporting evidence in the narrative developmental report, screening test results alone cannot establish a medically determinable impairment or the severity of developmental motor delay.
P. How will we determine whether your soft tissue injury or abnormality or your upper extremity fracture is no longer under continuing surgical management or you have received maximum benefit from therapy?
1. We will determine that your soft tissue injury or abnormality, or your upper extremity fracture, is no longer under continuing surgical management, as used in 101.21 and 101.23, when the last surgical procedure or medical treatment directed toward the re-establishment or improvement of function of the involved part has occurred.
2. We will determine that you have received maximum benefit from therapy, as used in 101.21, if there are no significant changes in physical findings or on appropriate imaging for any 6-month period after the last surgical procedure or medical treatment. We may also determine that you have received maximum benefit from therapy if your medical source(s) indicates that further improvement is not expected after the last surgical procedure or medical treatment.
3. When you have received maximum benefit from therapy, we will evaluate any impairment-related residual symptoms, signs, and laboratory findings (including those on imaging), any complications associated with your surgical procedures or medical treatments, and any residual limitations in your functioning (see 101.00R).
Q. How do we evaluate your musculoskeletal disorder if there is no record of ongoing treatment?
1. Despite having a musculoskeletal disorder, you may not have received ongoing treatment, may have just begun treatment, may not have access to prescribed medical treatment, or may not have an ongoing relationship with the medical community. In any of these situations, you will not have a longitudinal medical record for us to review when we evaluate your disorder and we may ask you to attend a consultative examination to determine the severity and potential duration of your disorder. See § 416.919a(b) of this chapter.
2. In some instances, we may be able to assess the severity and duration of your musculoskeletal disorder based on your medical record and current evidence alone. If the information in your case record is not sufficient to show that you have a musculoskeletal disorder that meets the criteria of one of the musculoskeletal disorders listings, we will follow the rules described in 101.00R.
R. How do we evaluate musculoskeletal disorders that do not meet one of these listings?
1. These listings are only examples of musculoskeletal disorders that we consider severe enough to result in marked and severe functional limitations. If your impairment(s) does not meet the criteria of any of these listings, we must also consider whether you have an impairment(s) that meets the criteria of a listing in another body system.
2. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. See § 416.926 of this chapter. If your impairment(s) does not meet or medically equal a listing, we will determine whether it functionally equals the listings. See § 416.926a of this chapter.
3. We use the rules in § 416.994a of this chapter when we decide whether you continue to be disabled.
101.01 Category of Impairments, Musculoskeletal Disorders
101.15 Disorders of the skeletal spine resulting in compromise of a nerve root(s) (see 101.00F), documented by A, B, C, and D:
A. Neuro-anatomic (radicular) distribution of one or more of the following symptoms consistent with compromise of the affected nerve root(s):
1. Pain; or
2. Paresthesia; or
3. Muscle fatigue.
AND
B. Radicular distribution of neurological signs present during physical examination (see 101.00C2) or on a diagnostic test (see 101.00C3) and evidenced by 1, 2, and either 3 or 4:
1. Muscle weakness; and
2. Sign(s) of nerve root irritation, tension, or compression, consistent with compromise of the affected nerve root (see 101.00F2)
3. Sensory changes evidenced by:
a. Decreased sensation; or
b. Sensory nerve deficit (abnormal sensory nerve latency) on electrodiagnostic testing; or
4. Decreased deep tendon reflexes.
AND
C. Findings on imaging (see 101.00C3) consistent with compromise of a nerve root(s) in the cervical or lumbosacral spine.
AND
D. Impairment-related physical limitation of musculoskeletal functioning that has lasted, or is expected to last, for a continuous period of at least 12 months, and medical documentation of at least one of the following:
1. A documented medical need (see 101.C6a) for a walker, bilateral canes, or bilateral crutches (see 101.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 101.00C6e(i)); or
2. An inability to use one upper extremity to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 101.00E4), and a documented medical need (see 101.00C6a) for a one-handed, hand-held assistive device (see 101.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 101.00C6e(ii)); or
3. An inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 101.00E4).
101.16 Lumbar spinal stenosis resulting in compromise of the cauda equina (see 101.00G), documented by A, B, C, and D:
A. Symptom(s) of neurological compromise manifested as:
1. Nonradicular distribution of pain in one or both lower extremities; or
2. Nonradicular distribution of sensory loss in one or both lower extremities; or
3. Neurogenic claudication.
AND
B. Nonradicular neurological signs present during physical examination (see 101.00C2) or on a diagnostic test (see 101.00C3) and evidenced by 1 and either 2 or 3:
1. Muscle weakness.
2. Sensory changes evidenced by:
a. Decreased sensation; or
b. Sensory nerve deficit (abnormal sensory nerve latency) on electrodiagnostic testing; or
c. Areflexia, trophic ulceration, or bladder or bowel incontinence.
3. Decreased deep tendon reflexes in one or both lower extremities.
AND
C. Findings on imaging (see 101.00C3) or in an operative report (see 101.00C4) consistent with compromise of the cauda equina with lumbar spinal stenosis.
AND
D. Impairment-related physical limitation of musculoskeletal functioning that has lasted, or is expected to last, for a continuous period of at least 12 months, and medical documentation of at least one of the following:
1. A documented medical need (see 101.00C6a) for a walker, bilateral canes, or bilateral crutches (see 101.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 101.00C6e(i)); or
2. An inability to use one upper extremity to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 101.00E4), and a documented medical need (see 101.00C6a) for a one-handed, hand-held assistive device (see 101.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 101.00C6e(ii)).
101.17 Reconstructive surgery or surgical arthrodesis of a major weight-bearing joint (see 101.00H), documented by A, B, and C:
A. History of reconstructive surgery or surgical arthrodesis of a major weight-bearing joint.
AND
B. Impairment-related physical limitation of musculoskeletal functioning that has lasted, or is expected to last, for a continuous period of at least 12 months.
AND
C. A documented medical need (see 101.00C6a) for a walker, bilateral canes, or bilateral crutches (see 101.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 101.00C6e(i)).
101.18 Abnormality of a major joint(s) in any extremity (see 101.00I), documented by A, B, C, and D:
A. Chronic joint pain or stiffness.
AND
B. Abnormal motion, instability, or immobility of the affected joint(s).
AND
C. Anatomical abnormality of the affected joint(s) noted on:
1. Physical examination (for example, subluxation, contracture, or bony or fibrous ankylosis); or
2. Imaging (for example, joint space narrowing, bony destruction, or ankylosis or arthrodesis of the affected joint).
AND
D. Impairment-related physical limitation of musculoskeletal functioning that has lasted, or is expected to last, for a continuous period of at least 12 months, and medical documentation of at least one of the following:
1. A documented medical need (see 101.00C6a) for a walker, bilateral canes, or bilateral crutches (see 101.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 101.00C6e(i)); or
2. An inability to use one upper extremity to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 101.00E4), and a documented medical need (see 101.00C6a) for a one-handed, hand-held assistive device (see 101.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 101.00C6e(ii)); or
3. An inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 101.00E4).
101.19 Pathologic fractures due to any cause (see 101.00J), documented by A and B:
A. Pathologic fractures occurring on three separate occasions within a 12-month period.
AND
B. Impairment-related physical limitation of musculoskeletal functioning that has lasted, or is expected to last, for a continuous period of at least 12 months, and medical documentation of at least one of the following:
1. A documented medical need (see 101.00C6a) for a walker, bilateral canes, or bilateral crutches (see 101.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 101.00C6e(i)); or
2. An inability to use one upper extremity to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 101.00E4), and a documented medical need (see 101.00C6a) for a one-handed, hand-held assistive device (see 101.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 101.00C6e(ii)); or
3. An inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 101.00E4).
101.20 Amputation due to any cause (see 101.00K), documented by A, B, C, or D:
A. Amputation of both upper extremities, occurring at any level at or above the wrists (carpal joints), up to and including the shoulder (glenohumeral) joint.
OR
B. Hemipelvectomy or hip disarticulation.
OR
C. Amputation of one upper extremity, occurring at any level at or above the wrist (carpal joints), and amputation of one lower extremity, occurring at or above the ankle (talocrural joint), and medical documentation of at least one of the following:
1. A documented medical need (see 101.00C6a) for a walker, bilateral canes, or bilateral crutches (see 101.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 101.00C6e(i)); or
2. A documented medical need (see 101.00C6a) for a one-handed, hand-held assistive device (see 101.00C6d) requiring the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 101.00C6e(ii)); or
3. The inability to use the remaining upper extremity to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (101.00E4).
OR
D. Amputation of one or both lower extremities, occurring at or above the ankle (talocrural joint), with complications of the residual limb(s) that have lasted, or are expected to last, for a continuous period of at least 12 months, and medical documentation of 1 and 2:
1. The inability to use a prosthesis(es); and
2. A documented medical need (see 101.00C6a) for a walker, bilateral canes, or bilateral crutches (see 101.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 101.00C6e(i)).
101.21 Soft tissue injury or abnormality under continuing surgical management (see 101.00L), documented by A, B, and C:
A. Evidence confirms continuing surgical management (see 101.00P1) directed toward saving, reconstructing, or replacing the affected part of the body.
AND
B. The surgical management has been, or is expected to be, ongoing for a continuous period of at least 12 months.
AND
C. Maximum benefit from therapy (see 101.00P2) has not yet been achieved.
101.22 Non-healing or complex fracture of the femur, tibia, pelvis, or one or more of the talocrural bones (see 101.00M), documented by A, B, and C:
A. Solid union not evident on imaging (see 101.00C3) and not clinically solid.
AND
B. Impairment-related physical limitation of musculoskeletal functioning that has lasted, or is expected to last, for a continuous period of at least 12 months.
AND
C. A documented medical need (see 101.00C6a) for a walker, bilateral canes, or bilateral crutches (see 101.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 101.00C6e(i)).
101.23 Non-healing or complex fracture of an upper extremity (see 101.00N), documented by A and B:
A. Nonunion or complex fracture, of the shaft of the humerus, radius, or ulna, under continuing surgical management (see 101.00P1) directed toward restoration of functional use of the extremity.
AND
B. Medical documentation of an inability to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 101.00E4) that has lasted, or is expected to last, for a continuous period of at least 12 months.
101.24 Musculoskeletal disorders of infants and toddlers, from birth to attainment of age 3, with developmental motor delay (see 101.00O), documented by A or B:
A. A standardized developmental motor assessment that:
1. Shows motor development not more than one-half of the level typically expected for the child's age; or
2. Results in a valid score that is at least three standard deviations below the mean.
OR
B. Two narrative developmental reports that:
1. Are dated at least 120 days apart; and
2. Indicate current motor development not more than one-half of the level typically expected for the child's age.
102.00 Special Senses and Speech
A. How do we evaluate visual disorders?
1. What are visual disorders? Visual disorders are abnormalities of the eye, the optic nerve, the optic tracts, or the brain that may cause a loss of visual acuity or visual fields. A loss of visual acuity limits your ability to distinguish detail, read, do fine work, or perform other age-appropriate activities. A loss of visual fields limits your ability to perceive visual stimuli in the peripheral extent of vision.
2. How do we define statutory blindness? Statutory blindness is blindness as defined in sections 216(i)(1) and 1614(a)(2) of the Social Security Act (Act).
a. The Act defines blindness as central visual acuity of 20/200 or less in the better eye with the use of a correcting lens. We use your best-corrected central visual acuity for distance in the better eye when we determine if this definition is met. (For visual acuity testing requirements, see 102.00A5.)
b. The Act also provides that an eye that has a visual field limitation such that the widest diameter of the visual field subtends an angle no greater than 20 degrees is considered as having a central visual acuity of 20/200 or less. (For visual field testing requirements, see 102.00A6.)
c. You have statutory blindness only if your visual disorder meets the criteria of 102.02A, 102.02B, or 102.03A. You do not have statutory blindness if your visual disorder medically equals the criteria of 102.02A, 102.02B, or 102.03A or meets or medically equals the criteria of 102.03B, 102.03C, 102.04A, or 102.04B because your disability is based on criteria other than those in the statutory definition of blindness.
3. What evidence do we need to establish statutory blindness under title XVI? To establish that you have statutory blindness under title XVI, we need evidence showing only that your central visual acuity in your better eye or your visual field in your better eye meets the criteria in 102.00A2, provided that those measurements are consistent with the other evidence in your case record. We do not need documentation of the cause of your blindness. Also, there is no duration requirement for statutory blindness under title XVI (see §§ 416.981 and 416.983 of this chapter).
4. What evidence do we need to evaluate visual disorders, including those that result in statutory blindness under title II? To evaluate your visual disorder, we usually need a report of an eye examination that includes measurements of your best-corrected central visual acuity (see 102.00A5) or the extent of your visual fields (see 102.00A6), as appropriate. If you have visual acuity or visual field loss, we need documentation of the cause of the loss. A standard eye examination will usually indicate the cause of any visual acuity loss. A standard eye examination can also indicate the cause of some types of visual field deficits. Some disorders, such as cortical visual disorders, may result in abnormalities that do not appear on a standard eye examination. If the standard eye examination does not indicate the cause of your vision loss, we will request the information used to establish the presence of your visual disorder. If your visual disorder does not satisfy the criteria in 102.02, 102.03, or 102.04, we will request a description of how your visual disorder affects your ability to function.
5. How do we measure your best-corrected central visual acuity?
a. Visual acuity testing. When we need to measure your best-corrected central visual acuity, which is your optimal visual acuity attainable with the use of a corrective lens, we use visual acuity testing for distance that was carried out using Snellen methodology or any other testing methodology that is comparable to Snellen methodology.
(i) Your best-corrected central visual acuity for distance is usually measured by determining what you can see from 20 feet. If your visual acuity is measured for a distance other than 20 feet, we will convert it to a 20-foot measurement. For example, if your visual acuity is measured at 10 feet and is reported as 10/40, we will convert this measurement to 20/80.
(ii) A visual acuity recorded as CF (counts fingers), HM (hand motion only), LP or LPO (light perception or light perception only), or NLP (no light perception) indicates that no optical correction will improve your visual acuity. If your central visual acuity in an eye is recorded as CF, HM, LP or LPO, or NLP, we will determine that your best-corrected central visual acuity is 20/200 or less in that eye.
(iii) We will not use the results of pinhole testing or automated refraction acuity to determine your best-corrected central visual acuity. These tests provide an estimate of potential visual acuity but not an actual measurement of your best-corrected central visual acuity.
(iv) Very young children, such as infants and toddlers, cannot participate in testing using Snellen methodology or other comparable testing. If you are unable to participate in testing using Snellen methodology or other comparable testing due to your young age, we will consider clinical findings of your fixation and visual-following behavior. If both these behaviors are absent, we will consider the anatomical findings or the results of neuroimaging, electroretinogram, or visual evoked response (VER) testing when this testing has been performed.
b. Other test charts.
(i) Children between the ages of 3 and 5 often cannot identify the letters on a Snellen or other letter test chart. Specialists with expertise in assessment of childhood vision use alternate methods for measuring visual acuity in young children. We consider alternate methods, for example, the Landolt C test or the tumbling-E test, which are used to evaluate young children who are unable to participate in testing using Snellen methodology, to be comparable to testing using Snellen methodology.
(ii) Most test charts that use Snellen methodology do not have lines that measure visual acuity between 20/100 and 20/200. Some test charts, such as the Bailey-Lovie or the Early Treatment Diabetic Retinopathy Study (ETDRS), used mostly in research settings, have such lines. If your visual acuity is measured with one of these charts, and you cannot read any of the letters on the 20/100 line, we will determine that you have statutory blindness based on a visual acuity of 20/200 or less. For example, if your best-corrected central visual acuity for distance in the better eye is 20/160 using an ETDRS chart, we will find that you have statutory blindness. Regardless of the type of test chart used, you do not have statutory blindness if you can read at least one letter on the 20/100 line. For example, if your best-corrected central visual acuity for distance in the better eye is 20/125 + 1 using an ETDRS chart, we will find that you do not have statutory blindness because you are able to read one letter on the 20/100 line.
c. Testing using a specialized lens. In some instances, you may have visual acuity testing performed using a specialized lens, such as a contact lens. We will use the visual acuity measurements obtained with a specialized lens only if you have demonstrated the ability to use the specialized lens on a sustained basis. We will not use visual acuity measurements obtained with telescopic lenses.
d. Cycloplegic refraction is an examination of the eye performed after administering cycloplegic eye drops capable of relaxing the ability of the pupil to become smaller and temporarily paralyzing the focusing muscles. If your case record contains the results of cycloplegic refraction, we may use the results to determine your best-corrected central visual acuity. We will not purchase cycloplegic refraction.
e. VER testing measures your response to visual events and can often detect dysfunction that is undetectable through other types of examinations. If you have an absent response to VER testing in your better eye, we will determine that your best-corrected central visual acuity is 20/200 or less in that eye and that your visual acuity loss satisfies the criterion in 102.02A or 102.02B4, as appropriate, when these test results are consistent with the other evidence in your case record. If you have a positive response to VER testing in an eye, we will not use that result to determine your best-corrected central visual acuity in that eye.
6. How do we measure your visual fields?
a. General. We generally need visual field testing when you have a visual disorder that could result in visual field loss, such as glaucoma, retinitis pigmentosa, or optic neuropathy, or when you display behaviors that suggest a visual field loss. When we need to measure the extent of your visual field loss, we use visual field testing (also referred to as perimetry) carried out using automated static threshold perimetry performed on an acceptable perimeter. (For perimeter requirements, see 102.00A9.)
b. Automated static threshold perimetry requirements.
(i) The test must use a white size III Goldmann stimulus and a 31.5 apostilb (asb) white background (or a 10 candela per square meter (cd/m2) white background). The stimuli test locations must be no more than 6 degrees apart horizontally or vertically. Measurements must be reported on standard charts and include a description of the size and intensity of the test stimulus.
(ii) We measure the extent of your visual field loss by determining the portion of the visual field in which you can see a white III4e stimulus. The “III” refers to the standard Goldmann test stimulus size III (4 mm2), and the “4e” refers to the standard Goldmann intensity filter (0 decibel (dB) attenuation, which allows presentation of the maximum luminance) used to determine the intensity of the stimulus.
(iii) In automated static threshold perimetry, the intensity of the stimulus varies. The intensity of the stimulus is expressed in decibels (dB). A perimeter's maximum stimulus luminance is usually assigned the value 0 dB. We need to determine the dB level that corresponds to a 4e intensity for the particular perimeter being used. We will then use the dB printout to determine which points you see at a 4e intensity level (a “seeing point”). For example:
A. When the maximum stimulus luminance (0 dB stimulus) on an acceptable perimeter is 10,000 asb, a 10 dB stimulus is equivalent to a 4e stimulus. Any point you see at 10 dB or greater is a seeing point.
B. When the maximum stimulus luminance (0 dB stimulus) on an acceptable perimeter is 4,000 asb, a 6 dB stimulus is equivalent to a 4e stimulus. Any point you see at 6 dB or greater is a seeing point.
C. When the maximum stimulus luminance (0 dB stimulus) on an acceptable perimeter is 1,000 asb, a 0 dB stimulus is equivalent to a 4e stimulus. Any point you see at 0 dB or greater is a seeing point.
c. Evaluation under 102.03A. To determine statutory blindness based on visual field loss in your better eye (102.03A), we need the results of a visual field test that measures the central 24 to 30 degrees of your visual field; that is, the area measuring 24 to 30 degrees from the point of fixation. Acceptable tests include the Humphrey Field Analyzer (HFA) 30-2, HFA 24-2, and Octopus 32.
d. Evaluation under 102.03B. To determine whether your visual field loss meets listing 102.03B, we use the mean deviation or defect (MD) from acceptable automated static threshold perimetry that measures the central 30 degrees of the visual field. MD is the average sensitivity deviation from normal values for all measured visual field locations. When using results from HFA tests, which report the MD as a negative number, we use the absolute value of the MD to determine whether your visual field loss meets listing 102.03B. We cannot use tests that do not measure the central 30 degrees of the visual field, such as the HFA 24-2, to determine if your impairment meets or medically equals 102.03B.
e. Other types of perimetry. If your case record contains visual field measurements obtained using manual or automated kinetic perimetry, such as Goldmann perimetry or the HFA “SSA Test Kinetic,” we can generally use these results if the kinetic test was performed using a white III4e stimulus projected on a white 31.5 asb (10 cd/m2) background. Automated kinetic perimetry, such as the HFA “SSA Test Kinetic,” does not detect limitations in the central visual field because testing along a meridian stops when you see the stimulus. If your visual disorder has progressed to the point at which it is likely to result in a significant limitation in the central visual field, such as a scotoma (see 102.00A6h), we will not use automated kinetic perimetry to determine the extent of your visual field loss. Instead, we will determine the extent of your visual field loss using automated static threshold perimetry or manual kinetic perimetry.
f. Screening tests. We will not use the results of visual field screening tests, such as confrontation tests, tangent screen tests, or automated static screening tests, to determine that your impairment meets or medically equals a listing, or functionally equals the listings. We can consider normal results from visual field screening tests to determine whether your visual disorder is severe when these test results are consistent with the other evidence in your case record. (See § 416.924(c) of this chapter.) We will not consider normal test results to be consistent with the other evidence if the clinical findings indicate that your visual disorder has progressed to the point that it is likely to cause visual field loss, or you have a history of an operative procedure for retinal detachment.
g. Use of corrective lenses. You must not wear eyeglasses during visual field testing because they limit your field of vision. You may wear contact lenses to correct your visual acuity during the visual field test to obtain the most accurate visual field measurements. For this single purpose, you do not need to demonstrate that you have the ability to use the contact lenses on a sustained basis.
h. Scotoma. A scotoma is a field defect or non-seeing area (also referred to as a “blind spot”) in the visual field surrounded by a normal field or seeing area. When we measure your visual field, we subtract the length of any scotoma, other than the normal blind spot, from the overall length of any diameter on which it falls.
7. How do we determine your visual acuity efficiency, visual field efficiency, and visual efficiency?
a. General. Visual efficiency, a calculated value of your remaining visual function, is the combination of your visual acuity efficiency and your visual field efficiency expressed as a percentage.
b. Visual acuity efficiency. Visual acuity efficiency is a percentage that corresponds to the best-corrected central visual acuity for distance in your better eye. See Table 1.
Table 1 - Visual Acuity Efficiency
| Snellen best-corrected central visual acuity for distance | Visual acuity efficiency (%)
(102.04A) | |
|---|---|---|
| English | Metric | |
| 20/16 | 6/5 | 100 |
| 20/20 | 6/6 | 100 |
| 20/25 | 6/7.5 | 95 |
| 20/30 | 6/9 | 90 |
| 20/40 | 6/12 | 85 |
| 20/50 | 6/15 | 75 |
| 20/60 | 6/18 | 70 |
| 20/70 | 6/21 | 65 |
| 20/80 | 6/24 | 60 |
| 20/100 | 6/30 | 50 |
c. Visual field efficiency. Visual field efficiency is a percentage that corresponds to the visual field in your better eye. Under 102.03C, we require kinetic perimetry to determine your visual field efficiency percentage. We calculate the visual field efficiency percentage by adding the number of degrees you see along the eight principal meridians found on a visual field chart (0, 45, 90, 135, 180, 225, 270, and 315) in your better eye and dividing by 5. For example, in Figure 1:
A. The diagram of the left eye illustrates a visual field, as measured with a III4e stimulus, contracted to 30 degrees in two meridians (180 and 225) and to 20 degrees in the remaining six meridians. The visual efficiency percentage of this field is: ((2 × 30) + (6 × 20)) ÷ 5 = 36 percent.
B. The diagram of the right eye illustrates the extent of a normal visual field as measured with a III4e stimulus. The sum of the eight principal meridians of this field is 500 degrees. The visual efficiency percentage of this field is 500 ÷ 5 = 100 percent.

d. Visual efficiency. Under 102.04A, we calculate the visual efficiency percentage by multiplying your visual acuity efficiency percentage (see 102.00A7b) by your visual field efficiency percentage (see 102.00A7c) and dividing by 100. For example, if your visual acuity efficiency percentage is 75 and your visual field efficiency percentage is 36, your visual efficiency percentage is: (75 × 36) ÷ 100 = 27 percent.
8. How do we determine your visual acuity impairment value, visual field impairment value, and visual impairment value?
a. General. Visual impairment value, a calculated value of your loss of visual function, is the combination of your visual acuity impairment value and your visual field impairment value.
b. Visual acuity impairment value. Your visual acuity impairment value corresponds to the best-corrected central visual acuity for distance in your better eye. See Table 2.
Table 2 - Visual Acuity Impairment Value
| Snellen best-corrected central visual acuity for distance | Visual acuity
impairment value (102.04B) | |
|---|---|---|
| English | Metric | |
| 20/16 | 6/5 | 0.00 |
| 20/20 | 6/6 | 0.00 |
| 20/25 | 6/7.5 | 0.10 |
| 20/30 | 6/9 | 0.18 |
| 20/40 | 6/12 | 0.30 |
| 20/50 | 6/15 | 0.40 |
| 20/60 | 6/18 | 0.48 |
| 20/70 | 6/21 | 0.54 |
| 20/80 | 6/24 | 0.60 |
| 20/100 | 6/30 | 0.70 |
c. Visual field impairment value. Your visual field impairment value corresponds to the visual field in your better eye. Using the MD from acceptable automated static threshold perimetry, we calculate the visual field impairment value by dividing the absolute value of the MD by 22. For example, if your MD on an HFA 30-2 is −16, your visual field impairment value is: |−16| ÷ 22 = 0.73.
d. Visual impairment value. Under 102.04B, we calculate the visual impairment value by adding your visual acuity impairment value (see 102.00A8b) and your visual field impairment value (see 102.00A8c). For example, if your visual acuity impairment value is 0.48 and your visual field impairment value is 0.73, your visual impairment value is: 0.48 + 0.73 = 1.21.
9. What are our requirements for an acceptable perimeter? We will use results from automated static threshold perimetry performed on a perimeter that:
a. Uses optical projection to generate the test stimuli.
b. Has an internal normative database for automatically comparing your performance with that of the general population.
c. Has a statistical analysis package that is able to calculate visual field indices, particularly mean deviation or mean defect.
d. Demonstrates the ability to correctly detect visual field loss and correctly identify normal visual fields.
e. Demonstrates good test-retest reliability.
f. Has undergone clinical validation studies by three or more independent laboratories with results published in peer-reviewed ophthalmic journals.
B. How do we evaluate hearing loss?
1. What evidence do we need?
a. We need evidence showing that you have a medically determinable impairment that causes your hearing loss and audiometric measurements of the severity of your hearing loss. We generally require both an otologic examination and audiometric testing to establish that you have a medically determinable impairment that causes your hearing loss. You should have this audiometric testing within 2 months of the otologic examination. Once we have evidence that you have a medically determinable impairment, we can use the results of later audiometric testing to assess the severity of your hearing loss without another otologic examination. We will consider your test scores together with any other relevant information we have about your hearing, including information from outside of the test setting.
b. The otologic examination must be performed by a licensed physician (medical or osteopathic doctor) or audiologist. It must include your medical history, your description of how your hearing loss affects you, and the physician's or audiologist's description of the appearance of the external ears (pinnae and external ear canals), evaluation of the tympanic membranes, and assessment of any middle ear abnormalities.
c. Audiometric testing must be performed by, or under the direct supervision of, a licensed audiologist or an otolaryngologist.
2. What audiometric testing do we need when you do not have a cochlear implant?
a. General. We need either physiologic or behavioral testing (other than screening testing, see 102.00B2g) that is appropriate for your age at the time of testing. See 102.00B2c-102.00B2f. We will make every reasonable effort to obtain the results of physiologic testing that has been done; however, we will not purchase such testing.
b. Testing requirements. The testing must be conducted in accordance with the most recently published standards of the American National Standards Institute (ANSI). You must not wear hearing aids during the testing. Additionally, a person described in 102.00B1c must perform an otoscopic examination immediately before the audiometric testing. (An otoscopic examination provides a description of the appearance of your external ear canals and an evaluation of the tympanic membranes. In these rules, we use the term to include otoscopic examinations performed by physicians and otoscopic inspections performed by audiologists and others.) The otoscopic examination must show that there are no conditions that would prevent valid audiometric testing, such as fluid in the ear, ear infection, or obstruction in an ear canal. The person performing the test should also report on any other factors, such as your ability to maintain attention, that can affect the interpretation of the test results.
c. Children from birth to the attainment of age 6 months.
(i) We need physiologic testing, such as auditory brainstem response (ABR) testing.
(ii) To determine whether your hearing loss meets 102.10A, we will average your hearing thresholds at 500, 1000, 2000, and 4000 Hertz (Hz). If you do not have a response at a particular frequency, we will use a threshold of 5 decibels (dB) over the limit of the audiometer.
d. Children from age 6 months to the attainment of age 2.
(i) We need air conduction thresholds determined by a behavioral assessment, usually visual reinforcement audiometry (VRA). We can use ABR testing if the behavioral assessment cannot be completed or if the results are inconclusive or unreliable.
(ii) To determine whether your hearing loss meets 102.10A, we will average your hearing thresholds at 500, 1000, 2000, and 4000 Hz. If you do not have a response at a particular frequency, we will use a threshold of 5 dB over the limit of the audiometer.
(iii) For this age group, behavioral assessments are often performed in a sound field, and each ear is not tested separately. If each ear is not tested separately, we will consider the test results to represent the hearing in the better ear.
e. Children from age 2 to the attainment of age 5.
(i) We need air conduction thresholds determined by a behavioral assessment, such as conditioned play audiometry (CPA), tangible or visually reinforced operant conditioning audiometry (TROCA, VROCA), or VRA. If you have had ABR testing, we can use the results of that testing if the behavioral assessment cannot be completed or the results are inconclusive or unreliable.
(ii) To determine whether your hearing loss meets 102.10A, we will average your hearing thresholds at 500, 1000, 2000, and 4000 Hz. If you do not have a response at a particular frequency, we will use a threshold of 5 dB over the limit of the audiometer.
(iii) For this age group, behavioral assessments are often performed in a sound field and each ear is not tested separately. If each ear is not tested separately, we will consider the test results to represent the hearing in the better ear.
f. Children from age 5 to the attainment of age 18.
(i) We generally need pure tone air conduction and bone conduction testing, speech reception threshold (SRT) testing (also referred to as “spondee threshold” or “ST” testing), and word recognition testing (also referred to as “word discrimination” or “speech discrimination” testing). This testing must be conducted in a sound-treated booth or room and must be in accordance with the most recently published ANSI standards. Each ear must be tested separately.
(ii) To determine whether your hearing loss meets the air and bone conduction criterion in 102.10B1 or 102.10B3, we will average your hearing thresholds at 500, 1000, 2000, and 4000 Hz. If you do not have a response at a particular frequency, we will use a threshold of 5 dB over the limit of the audiometer.
(iii) The SRT is the minimum dB level required for you to recognize 50 percent of the words on a standard list of spondee words. (Spondee words are two-syllable words that have equal stress on each syllable.) The SRT is usually within 10 dB of the average pure tone air conduction hearing thresholds at 500, 1000, and 2000 Hz. If the SRT is not within 10 dB of the average pure tone air conduction threshold, the reason for the discrepancy must be documented. If we cannot determine that there is a medical basis for the discrepancy, we will not use the results of the testing to determine whether your hearing loss meets a listing.
(iv) Word recognition testing determines your ability to recognize an age-appropriate, standardized list of phonetically balanced monosyllabic words in the absence of any visual cues. This testing must be performed in quiet. The list may be recorded or presented live, but in either case, the words should be presented at a level of amplification that will measure your maximum ability to discriminate words, usually 35 to 40 dB above your SRT. However, the amplification level used in the testing must be medically appropriate, and you must be able to tolerate it. If you cannot be tested at 35 to 40 dB above your SRT, the person who performs the test should report your word recognition testing score at your highest comfortable level of amplification.
g. Screening testing. Physiologic testing, such as ABR and otoacoustic emissions (OAE), and pure tone testing can be used as hearing screening tests. We will not use these tests to determine that your hearing loss meets or medically equals a listing, or to assess functional limitations due to your hearing loss, when they are used only as screening tests. We can consider normal results from hearing screening tests to determine that your hearing loss is not “severe” when these test results are consistent with the other evidence in your case record. See § 416.924(c).
3. What audiometric testing do we need when you have a cochlear implant?
a. If you have a cochlear implant, we will consider you to be disabled until age 5, or for 1 year after initial implantation, whichever is later.
b. After that period, we need word recognition testing performed with any age-appropriate version of the Hearing in Noise Test (HINT) or the Hearing in Noise Test for Children (HINT-C) to determine whether your impairment meets 102.11B. This testing must be conducted in quiet in a sound field. Your implant must be functioning properly and adjusted to your normal settings. The sentences should be presented at 60 dB HL (Hearing Level) and without any visual cues.
4. How do we evaluate your word recognition ability if you are not fluent in English?
If you are not fluent in English, you should have word recognition testing using an appropriate word list for the language in which you are most fluent. The person conducting the test should be fluent in the language used for the test. If there is no appropriate word list or no person who is fluent in the language and qualified to perform the test, it may not be possible to measure your word recognition ability. If your word recognition ability cannot be measured, your hearing loss cannot meet 102.10B2 or 102.11B. Instead, we will consider the facts of your case to determine whether you have difficulty understanding words in the language in which you are most fluent, and if so, whether that degree of difficulty medically equals 102.10B2 or 102.11B. For example, we will consider how you interact with family members, interpreters, and other persons who speak the language in which you are most fluent.
5. What do we mean by a marked limitation in speech or language as used in 102.10B3?
a. We will consider you to have a marked limitation in speech if:
(i) Entire phrases or sentences in your conversation are intelligible to unfamiliar listeners at least 50 percent (half) of the time but no more than 67 percent (two-thirds) of the time on your first attempt; and
(ii) Your sound production or phonological patterns (the ways in which you combine speech sounds) are atypical for your age.
b. We will consider you to have a marked limitation in language when your current and valid test score on an appropriate comprehensive, standardized test of overall language functioning is at least two standard deviations below the mean. In addition, the evidence of your daily communication functioning must be consistent with your test score. If you are not fluent in English, it may not be possible to test your language performance. If we cannot test your language performance, your hearing loss cannot meet 102.10B3. Instead, we will consider the facts of your case to determine whether your hearing loss medically equals 102.10B3.
102.01 Category of Impairments, Special Senses and Speech
102.02 Loss of central visual acuity.
A. Remaining vision in the better eye after best correction is 20/200 or less.
OR
B. An inability to participate in visual acuity testing using Snellen methodology or other comparable testing, clinical findings that fixation and visual-following behavior are absent in the better eye, and one of the following:
1. Abnormal anatomical findings indicating a visual acuity of 20/200 or less in the better eye (such as the presence of Stage III or worse retinopathy of prematurity despite surgery, hypoplasia of the optic nerve, albinism with macular aplasia, or bilateral optic atrophy); or
2. Abnormal neuroimaging documenting damage to the cerebral cortex which would be expected to prevent the development of a visual acuity better than 20/200 in the better eye (such as neuroimaging showing bilateral encephalomyelitis or bilateral encephalomalacia); or
3. Abnormal electroretinogram documenting the presence of Leber's congenital amaurosis or achromatopsia in the better eye; or
4. An absent response to VER testing in the better eye.
102.03 Contraction of the visual field in the better eye, with:
A. The widest diameter subtending an angle around the point of fixation no greater than 20 degrees.
OR
B. An MD of 22 decibels or greater, determined by automated static threshold perimetry that measures the central 30 degrees of the visual field (see 102.00A6d.).
OR
C. A visual field efficiency of 20 percent or less, determined by kinetic perimetry (see 102.00A7c).
102.04 Loss of visual efficiency, or visual impairment, in the better eye:
A. A visual efficiency percentage of 20 or less after best correction (see 102.00A7d.).
OR
B. A visual impairment value of 1.00 or greater after best correction (see 102.00A8d).
102.10 Hearing loss not treated with cochlear implantation.
A. For children from birth to the attainment of age 5, an average air conduction hearing threshold of 50 decibels or greater in the better ear (see 102.00B2).
OR
B. For children from age 5 to the attainment of age 18:
1. An average air conduction hearing threshold of 70 decibels or greater in the better ear and an average bone conduction hearing threshold of 40 decibels or greater in the better ear (see 102.00B2f); or
2. A word recognition score of 40 percent or less in the better ear determined using a standardized list of phonetically balanced monosyllabic words (see 102.00B2f); or
3. An average air conduction hearing threshold of 50 decibels or greater in the better ear and a marked limitation in speech or language (see 102.00B2f and 102.00B5).
102.11 Hearing loss treated with cochlear implantation.
A. Consider under a disability until the attainment of age 5 or for 1 year after initial implantation, whichever is later.
OR
B. Upon the attainment of age 5 or 1 year after initial implantation, whichever is later, a word recognition score of 60 percent or less determined using the HINT or the HINT-C (see 102.00B3b).
103.00 Respiratory Disorders
A. Which disorders do we evaluate in this body system?
1. We evaluate respiratory disorders that result in obstruction (difficulty moving air out of the lungs) or restriction (difficulty moving air into the lungs), or that interfere with diffusion (gas exchange) across cell membranes in the lungs. Examples of such disorders and the listings we use to evaluate them include chronic obstructive pulmonary disease (103.02), chronic lung disease of infancy (also known as bronchopulmonary dysplasia, 103.02C or 103.02E), pulmonary fibrosis (103.02), asthma (103.02 or 103.03), and cystic fibrosis (103.04). We also use listings in this body system to evaluate respiratory failure resulting from an underlying chronic respiratory disorder (103.04E or 103.14) and lung transplantation (103.11).
2. We evaluate cancers affecting the respiratory system under the listings in 113.00. We evaluate the pulmonary effects of neuromuscular and autoimmune disorders under these listings or under the listings in 111.00 or 114.00, respectively.
B. What are the symptoms and signs of respiratory disorders? Symptoms and signs of respiratory disorders include dyspnea (shortness of breath), chest pain, coughing, wheezing, sputum production, hemoptysis (coughing up blood from the respiratory tract), use of accessory muscles of respiration, and tachypnea (rapid rate of breathing).
C. What abbreviations do we use in this body system?
1. BiPAP means bi-level positive airway pressure ventilation.
2. BTPS means body temperature and ambient pressure, saturated with water vapor.
3. CF means cystic fibrosis.
4. CFRD means CF-related diabetes.
5. CFTR means CF transmembrane conductance regulator.
6. CLD means chronic lung disease of infancy.
7. FEV1 means forced expiratory volume in the first second of a forced expiratory maneuver.
8. FVC means forced vital capacity.
9. L means liter.
D. What documentation do we need to evaluate your respiratory disorder?
1. We need medical evidence to document and assess the severity of your respiratory disorder. Medical evidence should include your medical history, physical examination findings, the results of imaging (see 103.00D3), spirometry (see 103.00E), other relevant laboratory tests, and descriptions of any prescribed treatment and your response to it. We may not need all of this evidence depending on your particular respiratory disorder and its effects on you.
2. If you use supplemental oxygen, we still need medical evidence to establish the severity of your respiratory disorder.
3. Imaging refers to medical imaging techniques, such as x-ray and computerized tomography. The imaging must be consistent with the prevailing state of medical knowledge and clinical practice as the proper technique to support the evaluation of the disorder.
E. What is spirometry and what are our requirements for an acceptable test and report?
1. Spirometry, which measures how well you move air into and out of your lungs, involves at least three forced expiratory maneuvers during the same test session. A forced expiratory maneuver is a maximum inhalation followed by a forced maximum exhalation, and measures exhaled volumes of air over time. The volume of air you exhale in the first second of the forced expiratory maneuver is the FEV1. The total volume of air that you exhale during the entire forced expiratory maneuver is the FVC. We use your highest FEV1 value to evaluate your respiratory disorder under 103.02A and 103.04A, and your highest FVC value to evaluate your respiratory disorder under 103.02B, regardless of whether the values are from the same forced expiratory maneuver or different forced expiratory maneuvers. We will not purchase spirometry for children who have not attained age 6.
2. We have the following requirements for spirometry under these listings:
a. You must be medically stable at the time of the test. Examples of when we would not consider you to be medically stable include when you are:
(i) Within 2 weeks of a change in your prescribed respiratory medication.
(ii) Experiencing, or within 30 days of completion of treatment for, a lower respiratory tract infection.
(iii) Experiencing, or within 30 days of completion of treatment for, an acute exacerbation (temporary worsening) of a chronic respiratory disorder. Wheezing by itself does not indicate that you are not medically stable.
b. During testing, if your FEV1 is less than 70 percent of your predicted normal value, we require repeat spirometry after inhalation of a bronchodilator to evaluate your respiratory disorder under these listings, unless it is medically contraindicated. If you used a bronchodilator before the test and your FEV1 is less than 70 percent of your predicted normal value, we still require repeat spirometry after inhalation of a bronchodilator unless the supervising physician determines that it is not safe for you to take a bronchodilator again (in which case we may need to reschedule the test). If you do not have post-bronchodilator spirometry, the test report must explain why. We can use the results of spirometry administered without bronchodilators when the use of bronchodilators is medically contraindicated.
c. Your forced expiratory maneuvers must be satisfactory. We consider a forced expiratory maneuver to be satisfactory when you exhale with maximum effort following a full inspiration, and when the test tracing has a sharp takeoff and rapid rise to peak flow, has a smooth contour, and either lasts for at least 6 seconds (for children age 10 and older) or for at least 3 seconds (for children who have not attained age 10), or maintains a plateau for at least 1 second.
3. The spirometry report must include the following information:
a. The date of the test and your name, age or date of birth, gender, and height without shoes. (We will assume that your recorded height on the date of the test is without shoes, unless we have evidence to the contrary.) If your spine is abnormally curved (for example, you have kyphoscoliosis), we will substitute the longest distance between your outstretched fingertips with your arms abducted 90 degrees in place of your height when this measurement is greater than your standing height without shoes.
b. Any factors, if applicable, that can affect the interpretation of the test results (for example, your cooperation or effort in doing the test).
c. Legible tracings of your forced expiratory maneuvers in a volume-time format showing your name and the date of the test for each maneuver.
4. If you have attained age 6, we may need to purchase spirometry to determine whether your disorder meets a listing, unless we can make a fully favorable determination or decision on another basis.
5. Before we purchase spirometry for a child age 6 or older, a medical consultant (see § 416.1016 of this chapter), preferably one with experience in the care of children with respiratory disorders, must review your case record to determine if we need the test. If we purchase spirometry, the medical source we designate to administer the test is solely responsible for deciding whether it is safe for you to do the test and for how to administer it.
F. What is CLD and how do we evaluate it?
1. CLD, also known as bronchopulmonary dysplasia, or BPD, is scarring of the immature lung. CLD may develop as a complication of mechanical ventilation and oxygen therapy for infants with significant neonatal respiratory problems. Within the first 6 months of life, most infants with CLD are successfully weaned from mechanical ventilation, and then weaned from oxygen supplementation. We evaluate CLD under 103.02C, 103.02E, or if you are age 2 or older, under 103.03 or another appropriate listing.
2. If you have CLD, are not yet 6 months old, and need 24-hour-per-day oxygen supplementation, we will not evaluate your CLD under 103.02C until you are 6 months old. Depending on the evidence in your case record, we may make a fully favorable determination or decision under other rules before you are 6 months old.
3. We evaluate your CLD under 103.02C if you are at least 6 months old and you need 24-hour-per-day oxygen supplementation. (If you were born prematurely, we use your corrected chronological age. See § 416.924b(b) of this chapter.) We also evaluate your CLD under 103.02C if you were weaned off oxygen supplementation but needed it again by the time you were 6 months old or older.
4. We evaluate your CLD under 103.02E if you are any age from birth to the attainment of age 2 and have CLD exacerbations or complications (for example, wheezing, lower respiratory tract infections, or acute respiratory distress) that require hospitalization. For the purpose of 103.02E, we count your initial birth hospitalization as one hospitalization. The phrase “consider under a disability for 1 year from the discharge date of the last hospitalization or until the attainment of age 2, whichever is later” in 103.02E does not refer to the date on which your disability began, only to the date on which we must reevaluate whether your impairment(s) continues to meet a listing or is otherwise disabling.
G. What is asthma and how do we evaluate it?
1. Asthma is a chronic inflammatory disorder of the lung airways that we evaluate under 103.02 or 103.03. If you have respiratory failure resulting from chronic asthma (see 103.00J), we will evaluate it under 103.14.
2. For the purposes of 103.03:
a. The phrase “consider under a disability for 1 year” explains how long your asthma can meet the requirements of the listing. It does not refer to the date on which your disability began, only to the date on which we must reevaluate whether your asthma continues to meet a listing or is otherwise disabling.
b. We determine the onset of your disability based on the facts of your case, but it will be no later than the admission date of your first of three hospitalizations that satisfy the criteria of 103.03.
H. What is CF and how do we evaluate it?
1. General. We evaluate CF, a genetic disorder that results in abnormal salt and water transport across cell membranes in the lungs, pancreas, and other body organs, under 103.04. We need the evidence described in 103.00H2 to establish that you have CF.
2. Documentation of CF. We need a report signed by a physician (see § 416.913(a) of this chapter) showing both a and b:
a. One of the following:
(i) A positive newborn screen for CF; or
(ii) A history of CF in a sibling; or
(iii) Documentation of at least one specific CF phenotype or clinical criterion (for example, chronic sino-pulmonary disease with persistent colonization or infections with typical CF pathogens, pancreatic insufficiency, or salt-loss syndromes); and
b. One of the following definitive laboratory tests:
(i) An elevated sweat chloride concentration equal to or greater than 60 millimoles per L; or
(ii) The identification of two CF gene mutations affecting the CFTR; or
(iii) Characteristic abnormalities in ion transport across the nasal epithelium.
c. When we have the report showing a and b, but it is not signed by a physician, we also need a report from a physician stating that you have CF.
d. When we do not have the report showing a and b, we need a report from a physician that is persuasive that a positive diagnosis of CF was confirmed by an appropriate definitive laboratory test. To be persuasive, this report must include a statement by the physician that you had the appropriate definitive laboratory test for diagnosing CF. The report must provide the test results or explain how your diagnosis was established that is consistent with the prevailing state of medical knowledge and clinical practice.
3. CF pulmonary exacerbations. Examples of CF pulmonary exacerbations include increased cough and sputum production, hemoptysis, increased shortness of breath, increased fatigue, and reduction in pulmonary function. Treatment usually includes intravenous antibiotics and intensified airway clearance therapy (for example, increased frequencies of chest percussion or increased use of inhaled nebulized therapies, such as bronchodilators or mucolytics).
4. For 103.04G, we require any two exacerbations or complications from the list in 103.04G1 through 103.04G4 within a 12-month period. You may have two of the same exacerbation or complication or two different ones.
a. If you have two of the acute exacerbations or complications we describe in 103.04G1 and 103.04G2, there must be at least 30 days between the two.
b. If you have one of the acute exacerbations or complications we describe in 103.04G1 and 103.04G2 and one of the chronic complications we describe in 103.04G3 and 103.04G4, the two can occur during the same time. For example, your CF meets 103.04G if you have the pulmonary hemorrhage we describe in 103.04G2 and the weight loss we describe in 103.04G3 even if the pulmonary hemorrhage occurs during the 90-day period in 103.04G3.
c. Your CF also meets 103.04G if you have both of the chronic complications in 103.04G3 and 103.04G4.
5. CF may also affect other body systems such as digestive or endocrine. If your CF, including pulmonary exacerbations and nonpulmonary complications, does not meet or medically equal a respiratory disorders listing, we may evaluate your CF-related impairments under the listings in the affected body system.
I. How do we evaluate lung transplantation? If you receive a lung transplant (or a lung transplant simultaneously with other organs, such as the heart), we will consider you to be disabled under 103.11 for 3 years from the date of the transplant. After that, we evaluate your residual impairment(s) by considering the adequacy of your post-transplant function, the frequency and severity of any rejection episodes you have, complications in other body systems, and adverse treatment effects. Children who receive organ transplants generally have impairments that meet our definition of disability before they undergo transplantation. The phrase “consider under a disability for 3 years” in 103.11 does not refer to the date on which your disability began, only to the date on which we must reevaluate whether your impairment(s) continues to meet a listing or is otherwise disabling. We determine the onset of your disability based on the facts of your case.
J. What is respiratory failure and how do we evaluate it? Respiratory failure is the inability of the lungs to perform their basic function of gas exchange. We evaluate respiratory failure under 103.04E if you have CF-related respiratory failure, or under 103.14 if you have respiratory failure due to any other chronic respiratory disorder. Continuous positive airway pressure does not satisfy the criterion in 103.04E or 103.14, and cannot be substituted as an equivalent finding, for invasive mechanical ventilation or noninvasive ventilation with BiPAP.
K. How do we evaluate growth failure due to any chronic respiratory disorder?
1. To evaluate growth failure due to any chronic respiratory disorder, we require documentation of the oxygen supplementation described in 103.06A and the growth measurements in 103.06B within the same consecutive 12-month period. The dates of oxygen supplementation may be different from the dates of growth measurements.
2. Under 103.06B, we use the appropriate table(s) under 105.08B in the digestive system to determine whether a child's growth is less than the third percentile.
a. For children from birth to attainment of age 2, we use the weight-for-length table corresponding to the child's gender (Table I or Table II).
b. For children age 2 to attainment of age 18, we use the body mass index (BMI)-for-age table corresponding to the child's gender (Table III or Table IV).
c. BMI is the ratio of a child's weight to the square of his or her height. We calculate BMI using the formulas in 105.00G2c.
L. How do we evaluate respiratory disorders that do not meet one of these listings?
1. These listings are only examples of common respiratory disorders that we consider severe enough to result in marked and severe functional limitations. If your impairment(s) does not meet the criteria of any of these listings, we must also consider whether you have an impairment(s) that meets the criteria of a listing in another body system. For example, if your CF has resulted in chronic pancreatic or hepatobiliary disease, we evaluate your impairment under the listings in 105.00.
2. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. See § 416.926 of this chapter. Respiratory disorders may be associated with disorders in other body systems, and we consider the combined effects of multiple impairments when we determine whether they medically equal a listing. If your impairment(s) does not meet or medically equal a listing, we will also consider whether it functionally equals the listings. See § 416.926a of this chapter. We use the rules in § 416.994a of this chapter when we decide whether you continue to be disabled.
103.01 Category of Impairments, Respiratory Disorders
103.02 Chronic respiratory disorders due to any cause except CF (for CF, see 103.04), with A, B, C, D, or E:
A. FEV1 (see 103.00E) less than or equal to the value in Table I-A or I-B for your age, gender, and height without shoes (see 103.00E3a).
Table I - FEV1 Criteria for 103.02A
| Table I-A | Table I-B | |||||
|---|---|---|---|---|---|---|
| Age 6 to attainment of age 13
(for both females and males) | Age 13 to attainment of age 18 | |||||
| Height without shoes
(centimeters) < means less than | Height without shoes
(inches) < means less than | FEV1
less than or equal to (L, BTPS) | Height without shoes
(centimeters) < means less than | Height without shoes
(inches) < means less than | Females FEV1 less than
or equal to (L, BTPS) | Males FEV1 less than
or equal to (L, BTPS) |
| <123.0 | <48.50 | 0.80 | <153.0 | <60.25 | 1.35 | 1.40 |
| 123.0 to <129.0 | 48.50 to <50.75 | 0.90 | 153.0 to <159.0 | 60.25 to <62.50 | 1.45 | 1.50 |
| 129.0 to <134.0 | 50.75 to <52.75 | 1.00 | 159.0 to <164.0 | 62.50 to <64.50 | 1.55 | 1.60 |
| 134.0 to <139.0 | 52.75 to <54.75 | 1.10 | 164.0 to <169.0 | 64.50 to <66.50 | 1.65 | 1.70 |
| 139.0 to <144.0 | 54.75 to <56.75 | 1.20 | 169.0 to <174.0 | 66.50 to <68.50 | 1.75 | 1.85 |
| 144.0 to <149.0 | 56.75 to <58.75 | 1.30 | 174.0 to <180.0 | 68.50 to <70.75 | 1.85 | 2.00 |
| 149.0 or more | 58.75 or more | 1.40 | 180.0 or more | 70.75 or more | 1.95 | 2.10 |
OR
B. FVC (see 103.00E) less than or equal to the value in Table II-A or II-B for your age, gender, and height without shoes (see 103.00E3a).
Table II - FVC Criteria for 103.02B
| Table II-A | Table II-B | |||||
|---|---|---|---|---|---|---|
| Age 6 to attainment of age 13
(for both females and males) | Age 13 to attainment of age 18 | |||||
| Height without shoes (centimeters)
< means less than | Height without shoes
(inches) < means less than | FVC
less than or equal to (L, BTPS) | Height without shoes
(centimeters) < means less than | Height without shoes
(inches) < means less than | Females
FVC less than or equal to (L, BTPS) | Males
FVC less than or equal to (L, BTPS) |
| <123.0 | <48.50 | 0.85 | <153.0 | <60.25 | 1.65 | 1.65 |
| 123.0 to <129.0 | 48.50 to <50.75 | 1.00 | 153.0 to <159.0 | 60.25 to <62.50 | 1.70 | 1.80 |
| 129.0 to <134.0 | 50.75 to <52.75 | 1.10 | 159.0 to <164.0 | 62.50 to <64.50 | 1.80 | 1.95 |
| 134.0 to <139.0 | 52.75 to <54.75 | 1.30 | 164.0 to <169.0 | 64.50 to <66.50 | 1.95 | 2.10 |
| 139.0 to <144.0 | 54.75 to <56.75 | 1.40 | 169.0 to <174.0 | 66.50 to <68.50 | 2.05 | 2.25 |
| 144.0 to <149.0 | 56.75 to <58.75 | 1.55 | 174.0 to <180.0 | 68.50 to <70.75 | 2.20 | 2.45 |
| 149.0 or more | 58.75 or more | 1.70 | 180.0 or more | 70.75 or more | 2.30 | 2.55 |
OR
C. Hypoxemia with the need for at least 1.0 L per minute of continuous (24 hours per day) oxygen supplementation for at least 90 consecutive days.
OR
D. The presence of a tracheostomy.
1. Consider under a disability until the attainment of age 3; or
2. Upon the attainment of age 3, documented need for mechanical ventilation via a tracheostomy for at least 4 hours per day and for at least 90 consecutive days.
OR
E. For children who have not attained age 2, CLD (see 103.00F) with exacerbations or complications requiring three hospitalizations within a 12-month period and at least 30 days apart (the 12-month period must occur within the period we are considering in connection with your application or continuing disability review). Each hospitalization must last at least 48 hours, including hours in a hospital emergency department immediately before the hospitalization. (A child's initial birth hospitalization when CLD is first diagnosed counts as one hospitalization.) Consider under a disability for 1 year from the discharge date of the last hospitalization or until the attainment of age 2, whichever is later. After that, evaluate the impairment(s) under 103.03 or another appropriate listing.
103.03 Asthma (see 103.00G) with exacerbations or complications requiring three hospitalizations within a 12-month period and at least 30 days apart (the 12-month period must occur within the period we are considering in connection with your application or continuing disability review). Each hospitalization must last at least 48 hours, including hours in a hospital emergency department immediately before the hospitalization. Consider under a disability for 1 year from the discharge date of the last hospitalization; after that, evaluate the residual impairment(s) under 103.03 or another appropriate listing.
103.04 Cystic fibrosis (documented as described in 103.00H), with A, B, C, D, E, F, or G:
A. FEV1 (see 103.00E) less than or equal to the value in Table III-A or Table III-B for your age, gender, and height without shoes (see 103.00E3a).
Table III - FEV1 Criteria for 103.04A
| Table III-A | Table III-B | |||||
|---|---|---|---|---|---|---|
| Age 6 to attainment of age 13
(for both females and males) | Age 13 to attainment of age 18 | |||||
| Height without shoes (centimeters)
< means less than | Height without shoes
(inches) < means less than | FEV1
less than or equal to (L, BTPS) | Height without shoes (centimeters)
< means less than | Height without shoes
(inches) < means less than | Females
FEV1 less than or equal to (L, BTPS) | Males
FEV1 less than or equal to (L, BTPS) |
| <123.0 | <48.50 | 1.00 | <153.0 | <60.25 | 1.75 | 1.85 |
| 123.0 to <129.0 | 48.50 to <50.75 | 1.15 | 153.0 to <159.0 | 60.25 to <62.50 | 1.85 | 2.05 |
| 129.0 to <134.0 | 50.75 to <52.75 | 1.25 | 159.0 to <164.0 | 62.50 to <64.50 | 1.95 | 2.15 |
| 134.0 to <139.0 | 52.75 to <54.75 | 1.40 | 164.0 to <169.0 | 64.50 to <66.50 | 2.10 | 2.30 |
| 139.0 to <144.0 | 54.75 to <56.75 | 1.50 | 169.0 to <174.0 | 66.50 to <68.50 | 2.25 | 2.45 |
| 144.0 to <149.0 | 56.75 to <58.75 | 1.70 | 174.0 to <180.0 | 68.50 to <70.75 | 2.35 | 2.60 |
| 149.0 or more | 58.75 or more | 1.80 | 180.0 or more | 70.75 or more | 2.50 | 2.70 |
OR
B. For children who have not attained age 6, findings on imaging (see 103.00D3) of thickening of the proximal bronchial airways, nodular-cystic lesions, segmental or lobular atelectasis, or consolidation, and documentation of one of the following:
1. Shortness of breath with activity; or
2. Accumulation of secretions as manifested by repetitive coughing; or
3. Bilateral rales or rhonchi, or reduction of breath sounds.
OR
C. Exacerbations or complications (see 103.00H3) requiring three hospitalizations of any length within a 12-month period and at least 30 days apart (the 12-month period must occur within the period we are considering in connection with your application or continuing disability review).
OR
D. Spontaneous pneumothorax, secondary to CF, requiring chest tube placement.
OR
E. Respiratory failure (see 103.00J) requiring invasive mechanical ventilation, noninvasive ventilation with BiPAP, or a combination of both treatments, for a continuous period of at least 48 hours, or for a continuous period of at least 72 hours if postoperatively.
OR
F. Pulmonary hemorrhage requiring vascular embolization to control bleeding.
OR
G. Two of the following exacerbations or complications (either two of the same or two different, see 103.00H3 and 103.00H4) within a 12-month period (the 12-month period must occur within the period we are considering in connection with your application or continuing disability review):
1. Pulmonary exacerbation requiring 10 consecutive days of intravenous antibiotic treatment.
2. Pulmonary hemorrhage (hemoptysis with more than blood-streaked sputum but not requiring vascular embolization) requiring hospitalization of any length.
3. Weight loss requiring daily supplemental enteral nutrition via a gastrostomy for at least 90 consecutive days or parenteral nutrition via a central venous catheter for at least 90 consecutive days.
4. CFRD requiring daily insulin therapy for at least 90 consecutive days.
103.05 [Reserved]
103.06 Growth failure due to any chronic respiratory disorder (see 103.00K), documented by:
A. Hypoxemia with the need for at least 1.0 L per min of oxygen supplementation for at least 4 hours per day and for at least 90 consecutive days.
AND
B. Growth failure as required in 1 or 2:
1. For children from birth to attainment of age 2, three weight-for-length measurements that are:
a. Within a consecutive 12-month period; and
b. At least 60 days apart; and
c. Less than the third percentile on the appropriate weight-for-length table under 105.08B1; or
2. For children age 2 to attainment of age 18, three BMI-for-age measurements that are:
a. Within a consecutive 12-month period; and
b. At least 60 days apart; and
c. Less than the third percentile on the appropriate BMI-for-age table under 105.08B2.
103.07 [Reserved]
103.08 [Reserved]
103.09 [Reserved]
103.10 [Reserved]
103.11 Lung transplantation (see 103.00I). Consider under a disability for 3 years from the date of the transplant; after that, evaluate the residual impairment(s).
103.12 [Reserved]
103.13 [Reserved]
103.14 Respiratory failure (see 103.00J) resulting from any underlying chronic respiratory disorder except CF (for CF, see 103.04E), requiring invasive mechanical ventilation, noninvasive ventilation with BiPAP, or a combination of both treatments, for a continuous period of at least 48 hours, or for a continuous period of at least 72 hours if postoperatively, twice within a 12-month period and at least 30 days apart (the 12-month period must occur within the period we are considering in connection with your application or continuing disability review).
104.00 Cardiovascular System
A. General
1. What do we mean by a cardiovascular impairment?
a. We mean any disorder that affects the proper functioning of the heart or the circulatory system (that is, arteries, veins, capillaries, and the lymphatic drainage). The disorder can be congenital or acquired.
b. Cardiovascular impairment results from one or more of four consequences of heart disease:
(i) Chronic heart failure or ventricular dysfunction.
(ii) Discomfort or pain due to myocardial ischemia, with or without necrosis of heart muscle.
(iii) Syncope, or near syncope, due to inadequate cerebral perfusion from any cardiac cause, such as obstruction of flow or disturbance in rhythm or conduction resulting in inadequate cardiac output.
(iv) Central cyanosis due to right-to-left shunt, reduced oxygen concentration in the arterial blood, or pulmonary vascular disease.
c. Disorders of the veins or arteries (for example, obstruction, rupture, or aneurysm) may cause impairments of the lower extremities (peripheral vascular disease), the central nervous system, the eyes, the kidneys, and other organs. We will evaluate peripheral vascular disease under 4.11 or 4.12 in part A, and impairments of another body system(s) under the listings for that body system(s).
2. What do we consider in evaluating cardiovascular impairments? The listings in this section describe cardiovascular impairments based on symptoms, signs, laboratory findings, response to a regimen of prescribed treatment, and functional limitations.
3. What do the following terms or phrases mean in these listings?
a. Medical consultant is an individual defined in §§ 404.1616(a) and 416.1016(a). This term does not include medical sources who provide consultative examinations for us. We use the abbreviation “MC” throughout this section to designate a medical consultant.
b. Persistent means that the longitudinal clinical record shows that, with few exceptions, the required finding(s) has been present, or is expected to be present, for a continuous period of at least 12 months, such that a pattern of continuing severity is established.
c. Recurrent means that the longitudinal clinical record shows that, within a consecutive 12-month period, the finding(s) occurs at least three times, with intervening periods of improvement of sufficient duration that it is clear that separate events are involved.
d. Appropriate medically acceptable imaging means that the technique used is the proper one to evaluate and diagnose the impairment and is commonly recognized as accurate for assessing the cited finding.
e. A consecutive 12-month period means a period of 12 consecutive months, all or part of which must occur within the period we are considering in connection with an application or continuing disability review.
f. Currently present means that the finding is present at the time of adjudication.
g. Uncontrolled means the impairment does not respond adequately to standard prescribed medical treatment.
B. Documenting Cardiovascular Impairment
1. What basic documentation do we need? We need sufficiently detailed reports of history, physical examinations, laboratory studies, and any prescribed treatment and response to allow us to assess the severity and duration of your cardiovascular impairment. A longitudinal clinical record covering a period of not less than 3 months of observations and treatment is usually necessary, unless we can make a determination or decision based on the current evidence.
2. Why is a longitudinal clinical record important? We will usually need a longitudinal clinical record to assess the severity and expected duration of your impairment(s). If you have a listing-level impairment, you probably will have received medically prescribed treatment. Whenever there is evidence of such treatment, your longitudinal clinical record should include a description of the ongoing management and evaluation provided by your treating or other medical source. It should also include your response to this medical management, as well as information about the nature and severity of your impairment. The record will provide us with information on your functional status over an extended period of time and show whether your ability to function is improving, worsening, or unchanging.
3. What if you have not received ongoing medical treatment?
a. You may not have received ongoing treatment or have an ongoing relationship with the medical community despite the existence of a severe impairment(s). In this situation, we will base our evaluation on the current objective medical evidence and the other evidence we have. If you do not receive treatment, you cannot show an impairment that meets the criteria of these listings. However, we may find you disabled because you have another impairment(s) that in combination with your cardiovascular impairment medically equals the severity of a listed impairment or that functionally equals the listings.
b. Unless we can decide your claim favorably on the basis of the current evidence, a longitudinal record is still important. In rare instances where there is no or insufficient longitudinal evidence, we may purchase a consultative examination(s) to help us establish the severity and duration of your impairment.
4. When will we wait before we ask for more evidence?
a. We will wait when we have information showing that your impairment is not yet stable and the expected change in your impairment might affect our determination or decision. In these situations, we need to wait to properly evaluate the severity and duration of your impairment during a stable period. Examples of when we might wait are:
(i) If you have had a recent acute event; for example, acute rheumatic fever.
(ii) If you have recently had a corrective cardiac procedure; for example, open-heart surgery.
(iii) If you have started new drug therapy and your response to this treatment has not yet been established; for example, beta-blocker therapy for dilated congestive cardiomyopathy.
b. In these situations, we will obtain more evidence 3 months following the event before we evaluate your impairment. However, we will not wait if we have enough information to make a determination or decision based on all of the relevant evidence in your case.
5. Will we purchase any studies? In appropriate situations, we will purchase studies necessary to substantiate the diagnosis or to document the severity of your impairment, generally after we have evaluated the medical and other evidence we already have. We will not purchase studies involving exercise testing if there is significant risk involved or if there is another medical reason not to perform the test. We will follow sections 4.00C6, 4.00C7, 4.00C8, and 104.00B7 when we decide whether to purchase exercise testing. We will make a reasonable effort to obtain any additional studies from a qualified medical source in an office or center experienced in pediatric cardiac assessment. (See § 416.919g.)
6. What studies will we not purchase? We will not purchase any studies involving cardiac catheterization, such as coronary angiography, arteriograms, or electrophysiological studies. However, if the results of catheterization are part of the existing evidence we have, we will consider them together with the other relevant evidence. See 4.00C15a in part A.
7. Will we use exercise tolerance tests (ETTs) for evaluating children with cardiovascular impairment?
a. ETTs, though increasingly used, are still less frequently indicated in children than in adults, and can rarely be performed successfully by children under 6 years of age. An ETT may be of value in the assessment of some arrhythmias, in the assessment of the severity of chronic heart failure, and in the assessment of recovery of function following cardiac surgery or other treatment.
b. We will purchase an ETT in a childhood claim only if we cannot make a determination or decision based on the evidence we have and an MC, preferably one with experience in the care of children with cardiovascular impairments, has determined that an ETT is needed to evaluate your impairment. We will not purchase an ETT if you are less than 6 years of age. If we do purchase an ETT for a child age 12 or younger, it must be performed by a qualified medical source in a specialty center for pediatric cardiology or other facility qualified to perform exercise tests of children.
c. For full details on ETT requirements and usage, see 4.00C in part A.
C. Evaluating Chronic Heart Failure
1. What is chronic heart failure (CHF)?
a. CHF is the inability of the heart to pump enough oxygenated blood to body tissues. This syndrome is characterized by symptoms and signs of pulmonary or systemic congestion (fluid retention) or limited cardiac output. Certain laboratory findings of cardiac functional and structural abnormality support the diagnosis of CHF.
b. CHF is considered in these listings as a single category whether due to atherosclerosis (narrowing of the arteries), cardiomyopathy, hypertension, or rheumatic, congenital, or other heart disease. However, if the CHF is the result of primary pulmonary hypertension secondary to disease of the lung (cor pulmonale), we will evaluate your impairment using 3.09 in the respiratory system listings in part A.
2. What evidence of CHF do we need?
a. Cardiomegaly or ventricular dysfunction must be present and demonstrated by appropriate medically acceptable imaging, such as chest x-ray, echocardiography (M-Mode, 2-dimensional, and Doppler), radionuclide studies, or cardiac catheterization.
(i) Cardiomegaly is present when:
(A) Left ventricular diastolic dimension or systolic dimension is greater than 2 standard deviations above the mean for the child's body surface area;
(B) Left ventricular mass is greater than 2 standard deviations above the mean for the child's body surface area; or
(C) Chest x-ray (6 foot PA film) is indicative of cardiomegaly if the cardiothoracic ratio is over 60 percent at 1 year of age or less, or 55 percent or greater at more than 1 year of age.
(ii) Ventricular dysfunction is present when indices of left ventricular function, such as fractional shortening or ejection fraction (the percentage of the blood in the ventricle actually pumped out with each contraction), are greater than 2 standard deviations below the mean for the child's age. (Fractional shortening, also called shortening fraction, reflects the left ventricular systolic function in the absence of segmental wall motion abnormalities and has a linear correlation with ejection fraction. In children, fractional shortening is more commonly used than ejection fraction.)
(iii) However, these measurements alone do not reflect your functional capacity, which we evaluate by considering all of the relevant evidence.
(iv) Other findings on appropriate medically acceptable imaging may include increased pulmonary vascular markings, pleural effusion, and pulmonary edema. These findings need not be present on each report, since CHF may be controlled by prescribed treatment.
b. To establish that you have chronic heart failure, we require that your medical history and physical examination describe characteristic symptoms and signs of pulmonary or systemic congestion or of limited cardiac output associated with abnormal findings on appropriate medically acceptable imaging. When a remediable factor, such as arrhythmia, triggers an acute episode of heart failure, you may experience restored cardiac function, and a chronic impairment may not be present.
(i) Symptoms of congestion or of limited cardiac output include easy fatigue, weakness, shortness of breath (dyspnea), cough, or chest discomfort at rest or with activity. Children with CHF may also experience shortness of breath on lying flat (orthopnea) or episodes of shortness of breath that wake them from sleep (paroxysmal nocturnal dyspnea). They may also experience cardiac arrhythmias resulting in palpitations, lightheadedness, or fainting. Fatigue or exercise intolerance in an infant may be manifested by prolonged feeding time, often associated with excessive respiratory effort and sweating.
(ii) During infancy, other manifestations of chronic heart failure may include repeated lower respiratory tract infections.
(iii) Signs of congestion may include hepatomegaly, ascites, increased jugular venous distention or pressure, rales, peripheral edema, rapid shallow breathing (tachypnea), or rapid weight gain. However, these signs need not be found on all examinations because fluid retention may be controlled by prescribed treatment.
3. How do we evaluate growth failure due to CHF?
a. To evaluate growth failure due to CHF, we require documentation of the clinical findings of CHF described in 104.00C2 and the growth measurements in 104.02C within the same consecutive 12-month period. The dates of clinical findings may be different from the dates of growth measurements.
b. Under 104.02C, we use the appropriate table(s) under 105.08B in the digestive system to determine whether a child's growth is less than the third percentile.
(i) For children from birth to attainment of age 2, we use the weight-for-length table corresponding to the child's gender (Table I or Table II).
(ii) For children age 2 to attainment of age 18, we use the body mass index (BMI)-for-age table corresponding to the child's gender (Table III or Table IV).
(iii) BMI is the ratio of a child's weight to the square of his or her height. We calculate BMI using the formulas in 105.00G2c.
D. Evaluating Congenital Heart Disease
1. What is congenital heart disease? Congenital heart disease is any abnormality of the heart or the major blood vessels that is present at birth. Examples include:
a. Abnormalities of cardiac septation, including ventricular septal defect or atrioventricular canal;
b. Abnormalities resulting in cyanotic heart disease, including tetralogy of Fallot or transposition of the great arteries;
c. Valvular defects or obstructions to ventricular outflow, including pulmonary or aortic stenosis or coarctation of the aorta; and
d. Major abnormalities of ventricular development, including hypoplastic left heart syndrome or pulmonary tricuspid atresia with hypoplastic right ventricle.
2. How will we evaluate symptomatic congenital heart disease?
a. Because of improved treatment methods, more children with congenital heart disease are living longer. Although some types of congenital heart disease may be corrected by surgery, many children with treated congenital heart disease continue to have problems throughout their lives (symptomatic congenital heart disease). If you have congenital heart disease that results in chronic heart failure with evidence of ventricular dysfunction or in recurrent arrhythmias, we will evaluate your impairment under 104.02 or 104.05. Otherwise, we will evaluate your impairment under 104.06.
b. For 104.06A2, we will accept pulse oximetry measurements instead of arterial O2, but the arterial O2 values are preferred, if available.
c. For 104.06D, examples of impairments that in most instances will require life-saving surgery or a combination of surgery and other major interventional procedures (for example, multiple “balloon” catheter procedures) before age 1 include, but are not limited to, the following:
(i) Hypoplastic left heart syndrome,
(ii) Critical aortic stenosis with neonatal heart failure,
(iii) Critical coarctation of the aorta, with or without associated anomalies,
(iv) Complete atrioventricular canal defects,
(v) Transposition of the great arteries,
(vi) Tetralogy of Fallot,
(vii) Pulmonary atresia with intact ventricular septum,
(viii) Single ventricle,
(ix) Tricuspid atresia, and
(x) Multiple ventricular septal defects.
E. Evaluating Arrhythmias
1. What is an arrhythmia? An arrhythmia is a change in the regular beat of the heart. Your heart may seem to skip a beat or beat irregularly, very quickly (tachycardia), or very slowly (bradycardia).
2. What are the different types of arrhythmias?
a. There are many types of arrhythmias. Arrhythmias are identified by where they occur in the heart (atria or ventricles) and by what happens to the heart's rhythm when they occur.
b. Arrhythmias arising in the cardiac atria (upper chambers of the heart) are called atrial or supraventricular arrhythmias. Ventricular arrhythmias begin in the ventricles (lower chambers). In general, ventricular arrhythmias caused by heart disease are the most serious.
3. How do we evaluate arrhythmias using 104.05?
a. We will use 104.05 when you have arrhythmias that are not fully controlled by medication, an implanted pacemaker, or an implanted cardiac defibrillator and you have uncontrolled recurrent episodes of syncope or near syncope. If your arrhythmias are controlled, we will evaluate your underlying heart disease using the appropriate listing. For other considerations when we evaluate arrhythmias in the presence of an implanted cardiac defibrillator, see 104.00E4.
b. We consider near syncope to be a period of altered consciousness, since syncope is a loss of consciousness or a faint. It is not merely a feeling of light-headedness, momentary weakness, or dizziness.
c. For purposes of 104.05, there must be a documented association between the syncope or near syncope and the recurrent arrhythmia. The recurrent arrhythmia, not some other cardiac or non-cardiac disorder, must be established as the cause of the associated symptom. This documentation of the association between the symptoms and the arrhythmia may come from the usual diagnostic methods, including Holter monitoring (also called ambulatory electrocardiography) and tilt-table testing with a concurrent ECG. Although an arrhythmia may be a coincidental finding on an ETT, we will not purchase an ETT to document the presence of a cardiac arrhythmia.
4. What will we consider when you have an implanted cardiac defibrillator and you do not have arrhythmias that meet the requirements of 104.05?
a. Implanted cardiac defibrillators are used to prevent sudden cardiac death in children who have had, or are at high risk for, cardiac arrest from life-threatening ventricular arrhythmias. The largest group of children at risk for sudden cardiac death consists of children with cardiomyopathy (ischemic or non-ischemic) and reduced ventricular function. However, life-threatening ventricular arrhythmias can also occur in children with little or no ventricular dysfunction. The shock from the implanted cardiac defibrillator is a unique form of treatment; it rescues a child from what may have been cardiac arrest. However, as a consequence of the shock(s), children may experience psychological distress, which we may evaluate under the mental disorders listings in 112.00ff.
b. Most implantable cardiac defibrillators have rhythm-correcting and pacemaker capabilities. In some children, these functions may result in the termination of ventricular arrhythmias without an otherwise painful shock. (The shock is like being kicked in the chest.) Implanted cardiac defibrillators may deliver inappropriate shocks, often repeatedly, in response to benign arrhythmias or electrical malfunction. Also, exposure to strong electrical or magnetic fields, such as from MRI (magnetic resonance imaging), can trigger or reprogram an implanted cardiac defibrillator, resulting in inappropriate shocks. We must consider the frequency of, and the reason(s) for, the shocks when evaluating the severity and duration of your impairment.
c. In general, the exercise limitations imposed on children with an implanted cardiac defibrillator are those dictated by the underlying heart impairment. However, the exercise limitations may be greater when the implanted cardiac defibrillator delivers an inappropriate shock in response to the increase in heart rate with exercise, or when there is exercise-induced ventricular arrhythmia.
F. Evaluating Other Cardiovascular Impairments
1. What is ischemic heart disease (IHD) and how will we evaluate it in children? IHD results when one or more of your coronary arteries is narrowed or obstructed or, in rare situations, constricted due to vasospasm, interfering with the normal flow of blood to your heart muscle (ischemia). The obstruction may be the result of an embolus, a thrombus, or plaque. When heart muscle tissue dies as a result of the reduced blood supply, it is called a myocardial infarction (heart attack). Ischemia is rare in children, but when it occurs, its effects on children are the same as on adults. If you have IHD, we will evaluate it under 4.00E and 4.04 in part A.
2. How will we evaluate hypertension? Because hypertension (high blood pressure) generally causes disability through its effects on other body systems, we will evaluate it by reference to the specific body system(s) affected (heart, brain, kidneys, or eyes) when we consider its effects under the listings. We will also consider any limitations imposed by your hypertension when we consider whether you have an impairment that functionally equals the listings.
3. What is cardiomyopathy and how will we evaluate it? Cardiomyopathy is a disease of the heart muscle. The heart loses its ability to pump blood (heart failure), and in some instances, heart rhythm is disturbed, leading to irregular heartbeats (arrhythmias). Usually, the exact cause of the muscle damage is never found (idiopathic cardiomyopathy). There are various types of cardiomyopathy, which fall into two major categories: Ischemic and nonischemic cardiomyopathy. Ischemic cardiomyopathy typically refers to heart muscle damage that results from coronary artery disease, including heart attacks. Nonischemic cardiomyopathy includes several types: Dilated, hypertrophic, and restrictive. We will evaluate cardiomyopathy under 4.04 in part A, 104.02, 104.05, or 111.06, depending on its effects on you.
4. How will we evaluate valvular heart disease? We will evaluate valvular heart disease under the listing appropriate for its effect on you. Thus, we may use 4.04 in part A, 104.02, 104.05, 104.06, or an appropriate neurological listing in 111.00ff.
5. What do we consider when we evaluate heart transplant recipients?
a. After your heart transplant, we will consider you disabled for 1 year following the surgery because there is a greater likelihood of rejection of the organ and infection during the first year.
b. However, heart transplant patients generally meet our definition of disability before they undergo transplantation. We will determine the onset of your disability based on the facts in your case.
c. We will not assume that you became disabled when your name was placed on a transplant waiting list. This is because you may be placed on a waiting list soon after diagnosis of the cardiac disorder that may eventually require a transplant. Physicians recognize that candidates for transplantation often have to wait months or even years before a suitable donor heart is found, so they place their patients on the list as soon as permitted.
d. When we do a continuing disability review to determine whether you are still disabled, we will evaluate your residual impairment(s), as shown by symptoms, signs, and laboratory findings, including any side effects of medication. We will consider any remaining symptoms, signs, and laboratory findings indicative of cardiac dysfunction in deciding whether medical improvement (as defined in § 416.994a) has occurred.
6. How will we evaluate chronic rheumatic fever or rheumatic heart disease? The diagnosis should be made in accordance with the current revised Jones criteria for guidance in the diagnosis of rheumatic fever. We will evaluate persistence of rheumatic fever activity under 104.13. If you have evidence of chronic heart failure or recurrent arrhythmias associated with rheumatic heart disease, we will use 104.02 or 104.05.
7. What is hyperlipidemia and how will we evaluate it? Hyperlipidemia is the general term for an elevation of any or all of the lipids (fats or cholesterol) in the blood; for example, hypertriglyceridemia, hypercholesterolemia, and hyperlipoproteinemia. These disorders of lipoprotein metabolism and transport can cause defects throughout the body. The effects most likely to interfere with function are those produced by atherosclerosis (narrowing of the arteries) and coronary artery disease. We will evaluate your lipoprotein disorder by considering its effects on you.
8. How will we evaluate Kawasaki disease? We will evaluate Kawasaki disease under the listing appropriate to its effects on you, which may include major coronary artery aneurysm or heart failure. A major coronary artery aneurysm may cause ischemia or arrhythmia, which we will evaluate under 4.04 in part A or 104.05. We will evaluate chronic heart failure under 104.02.
9. What is lymphedema and how will we evaluate it?
a. Lymphedema is edema of the extremities due to a disorder of the lymphatic circulation; at its worst, it is called elephantiasis. Primary lymphedema is caused by abnormal development of lymph vessels and may be present at birth (congenital lymphedema), but more often develops during the teens (lymphedema praecox). Secondary lymphedema is due to obstruction or destruction of normal lymphatic channels due to tumor, surgery, repeated infections, or parasitic infection such as filariasis. Lymphedema most commonly affects one extremity.
b. Lymphedema does not meet the requirements of 4.11 in part A, although it may medically equal the severity of that listing. We will evaluate lymphedema by considering whether the underlying cause meets or medically equals any listing or whether the lymphedema medically equals a cardiovascular listing, such as 4.11, or a musculoskeletal disorders listing, such as 101.18. If no listing is met or medically equaled, we will evaluate any functional limitations imposed by your lymphedema when we consider whether you have an impairment that functionally equals the listings.
10. What is Marfan syndrome and how will we evaluate it?
a. Marfan syndrome is a genetic connective tissue disorder that affects multiple body systems, including the skeleton, eyes, heart, blood vessels, nervous system, skin, and lungs. There is no specific laboratory test to diagnose Marfan syndrome. The diagnosis is generally made by medical history, including family history, physical examination, including an evaluation of the ratio of arm/leg size to trunk size, a slit lamp eye examination, and a heart test(s), such as an echocardiogram. In some cases, a genetic analysis may be useful, but such analyses may not provide any additional helpful information.
b. The effects of Marfan syndrome can range from mild to severe. In most cases, the disorder progresses as you age. Most individuals with Marfan syndrome have abnormalities associated with the heart and blood vessels. Your heart's mitral valve may leak, causing a heart murmur. Small leaks may not cause symptoms, but larger ones may cause shortness of breath, fatigue, and palpitations. Another effect is that the wall of the aorta may be weakened and stretch (aortic dilation). This aortic dilation may tear, dissect, or rupture, causing serious heart problems or sometimes sudden death. We will evaluate the manifestations of your Marfan syndrome under the appropriate body system criteria, such as 4.10 in part A, or if necessary consider the functional limitations imposed by your impairment.
G. Other Evaluation Issues
1. What effect does obesity have on the cardiovascular system and how will we evaluate it? Obesity is a medically determinable impairment that is often associated with disorders of the cardiovascular system. Disturbance of this system can be a major cause of disability in children with obesity. Obesity may affect the cardiovascular system because of the increased workload the additional body mass places on the heart. Obesity may make it harder for the chest and lungs to expand. This can mean that the respiratory system must work harder to provide needed oxygen. This in turn would make the heart work harder to pump blood to carry oxygen to the body. Because the body would be working harder at rest, its ability to perform additional work would be less than would otherwise be expected. Thus, the combined effects of obesity with cardiovascular impairments can be greater than the effects of each of the impairments considered separately. We must consider any additional and cumulative effects of obesity when we determine whether you have a severe cardiovascular impairment or a listing-level cardiovascular impairment (or a combination of impairments that medically equals a listing), and when we determine whether your impairment(s) functionally equals the listings.
2. How do we relate treatment to functional status? In general, conclusions about the severity of a cardiovascular impairment cannot be made on the basis of type of treatment rendered or anticipated. The amount of function restored and the time required for improvement after treatment (medical, surgical, or a prescribed program of progressive physical activity) vary with the nature and extent of the disorder, the type of treatment, and other factors. Depending upon the timing of this treatment in relation to the alleged onset date of disability, we may need to defer evaluation of the impairment for a period of up to 3 months from the date treatment began to permit consideration of treatment effects, unless we can make a determination or decision using the evidence we have. See 104.00B4.
3. How do we evaluate impairments that do not meet one of the cardiovascular listings?
a. These listings are only examples of common cardiovascular disorders that we consider severe enough to result in marked and severe functional limitations. If your severe impairment(s) does not meet the criteria of any of these listings, we must also consider whether you have an impairment(s) that satisfies the criteria of a listing in another body system.
b. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. (See § 416.926.) If you have a severe impairment(s) that does not meet or medically equal the criteria of a listing, we will consider whether it functionally equals the listings. (See § 416.926a.) When we decide whether you continue to be disabled, we use the rules in § 416.994a.
104.01 Category of Impairments, Cardiovascular System
104.02. Chronic heart failure while on a regimen of prescribed treatment, with symptoms and signs described in 104.00C2, and with one of the following:
A. Persistent tachycardia at rest (see Table I);
OR
B. Persistent tachypnea at rest (see Table II) or markedly decreased exercise tolerance (see 104.00C2b);
OR
C. Growth failure as required in 1 or 2:
1. For children from birth to attainment of age 2, three weight-for-length measurements that are:
a. Within a consecutive 12-month period; and
b. At least 60 days apart; and
c. Less than the third percentile on the appropriate weight-for-length table under 105.08B1; or
2. For children age 2 to attainment of age 18, three BMI-for-age measurements that are:
a. Within a consecutive 12-month period; and
b. At least 60 days apart; and
c. Less than the third percentile on the appropriate BMI-for-age table under 105.08B2.
104.05 Recurrent arrhythmias, not related to reversible causes such as electrolyte abnormalities or digitalis glycoside or antiarrhythmic drug toxicity, resulting in uncontrolled (see 104.00A3g), recurrent (see 104.00A3c) episodes of cardiac syncope or near syncope (see 104.00E3b), despite prescribed treatment (see 104.00B3 if there is no prescribed treatment), and documented by resting or ambulatory (Holter) electrocardiography, or by other appropriate medically acceptable testing, coincident with the occurrence of syncope or near syncope (see 104.00E3c).
104.06 Congenital heart disease, documented by appropriate medically acceptable imaging (see 104.00A3d) or cardiac catheterization, with one of the following:
A. Cyanotic heart disease, with persistent, chronic hypoxemia as manifested by:
1. Hematocrit of 55 percent or greater on two evaluations 3 months or more apart within a consecutive 12-month period (see 104.00A3e); or
2. Arterial O2 saturation of less than 90 percent in room air, or resting arterial PO2 of 60 Torr or less; or
3. Hypercyanotic spells, syncope, characteristic squatting, or other incapacitating symptoms directly related to documented cyanotic heart disease; or
4. Exercise intolerance with increased hypoxemia on exertion.
OR
B. Secondary pulmonary vascular obstructive disease with pulmonary arterial systolic pressure elevated to at least 70 percent of the systemic arterial systolic pressure.
OR
C. Symptomatic acyanotic heart disease, with ventricular dysfunction interfering very seriously with the ability to independently initiate, sustain, or complete activities.
OR
D. For infants under 12 months of age at the time of filing, with life-threatening congenital heart impairment that will require or already has required surgical treatment in the first year of life, and the impairment is expected to be disabling (because of residual impairment following surgery, or the recovery time required, or both) until the attainment of at least 1 year of age, consider the infant to be under disability until the attainment of at least age 1; thereafter, evaluate impairment severity with reference to the appropriate listing.
104.09 Heart transplant. Consider under a disability for 1 year following surgery; thereafter, evaluate residual impairment under the appropriate listing.
104.13 Rheumatic heart disease, with persistence of rheumatic fever activity manifested by significant murmurs(s), cardiac enlargement or ventricular dysfunction (see 104.00C2a), and other associated abnormal laboratory findings; for example, an elevated sedimentation rate or ECG findings, for 6 months or more in a consecutive 12-month period (see 104.00A3e). Consider under a disability for 18 months from the established onset of impairment, then evaluate any residual impairment(s).
105.00 Digestive System
A. What kinds of disorders do we consider in the digestive system? Disorders of the digestive system include gastrointestinal hemorrhage, hepatic (liver) dysfunction, inflammatory bowel disease, short bowel syndrome, and malnutrition. They may also lead to complications, such as obstruction, or be accompanied by manifestations in other body systems. Congenital abnormalities involving the organs of the gastrointestinal system may interfere with the ability to maintain adequate nutrition, growth, and development.
B. What documentation do we need? We need a record of your medical evidence, including clinical and laboratory findings. The documentation should include appropriate medically acceptable imaging studies and reports of endoscopy, operations, and pathology, as appropriate to each listing, to document the severity and duration of your digestive disorder. We may also need assessments of your growth and development. Medically acceptable imaging includes, but is not limited to, x-ray imaging, sonography, computerized axial tomography (CAT scan), magnetic resonance imaging (MRI), and radionuclide scans. Appropriate means that the technique used is the proper one to support the evaluation and diagnosis of the disorder. The findings required by these listings must occur within the period we are considering in connection with your application or continuing disability review.
C. How do we consider the effects of treatment?
1. Digestive disorders frequently respond to medical or surgical treatment; therefore, we generally consider the severity and duration of these disorders within the context of the prescribed treatment.
2. We assess the effects of treatment, including medication, therapy, surgery, or any other form of treatment you receive, by determining if there are improvements in the symptoms, signs, and laboratory findings of your digestive disorder. We also assess any side effects of your treatment that may further limit your functioning.
3. To assess the effects of your treatment, we may need information about:
a. The treatment you have been prescribed (for example, the type of medication or therapy, or your use of parenteral (intravenous) nutrition or supplemental enteral nutrition via a gastrostomy);
b. The dosage, method, and frequency of administration;
c. Your response to the treatment;
d. Any adverse effects of such treatment; and
e. The expected duration of the treatment.
4. Because the effects of treatment may be temporary or long-term, in most cases we need information about the impact of your treatment, including its expected duration and side effects, over a sufficient period of time to help us assess its outcome. When adverse effects of treatment contribute to the severity of your impairment(s), we will consider the duration or expected duration of the treatment when we assess the duration of your impairment(s).
5. If you need parenteral (intravenous) nutrition or supplemental enteral nutrition via a gastrostomy to avoid debilitating complications of a digestive disorder, this treatment will not, in itself, indicate that you have marked and severe functional limitations. The exceptions are 105.07, short bowel syndrome, and 105.10, for children who have not attained age 3 and who require supplemental daily enteral feedings via a gastrostomy (see 105.00F and 105.00H).
6. If you have not received ongoing treatment or have not had an ongoing relationship with the medical community despite the existence of a severe impairment(s), we will evaluate the severity and duration of your digestive impairment on the basis of current medical and other evidence in your case record. If you have not received treatment, you may not be able to show an impairment that meets the criteria of one of the digestive system listings, but your digestive impairment may medically equal a listing or functionally equal the listings.
D. How do we evaluate chronic liver disease?
1. General. Chronic liver disease is characterized by liver cell necrosis, inflammation, or scarring (fibrosis or cirrhosis), due to any cause, that persists for more than 6 months. Chronic liver disease may result in portal hypertension, cholestasis (suppression of bile flow), extrahepatic manifestations, or liver cancer. (We evaluate liver cancer under 113.03.) Significant loss of liver function may be manifested by hemorrhage from varices or portal hypertensive gastropathy, ascites (accumulation of fluid in the abdominal cavity), hydrothorax (ascitic fluid in the chest cavity), or encephalopathy. There can also be progressive deterioration of laboratory findings that are indicative of liver dysfunction. Liver transplantation is the only definitive cure for end stage liver disease (ESLD).
2. Examples of chronic liver disease include, but are not limited to, biliary atresia, chronic hepatitis, non-alcoholic steatohepatitis (NASH), primary biliary cirrhosis (PBC), primary sclerosing cholangitis (PSC), autoimmune hepatitis, hemochromatosis, drug-induced liver disease, Wilson's disease, and serum alpha-1 antitrypsin deficiency. Children can also have congenital abnormalities of abdominal organs or inborn metabolic disorders that result in chronic liver disease. Acute hepatic injury is frequently reversible as in viral, drug-induced, toxin-induced, and ischemic hepatitis. In the absence of evidence of a chronic impairment, episodes of acute liver disease do not meet 105.05.
3. Manifestations of chronic liver disease.
a. Symptoms may include, but are not limited to, pruritis (itching), fatigue, nausea, loss of appetite, or sleep disturbances. Children can also have associated developmental delays or poor school performance. Symptoms of chronic liver disease may have a poor correlation with the severity of liver disease and functional ability.
b. Signs may include, but are not limited to, jaundice, enlargement of the liver and spleen, ascites, peripheral edema, and altered mental status.
c. Laboratory findings may include, but are not limited to, increased liver enzymes, increased serum total bilirubin, increased ammonia levels, decreased serum albumin, and abnormal coagulation studies, such as increased International Normalized Ratio (INR) or decreased platelet counts. Abnormally low serum albumin or elevated INR levels indicate loss of synthetic liver function, with increased likelihood of cirrhosis and associated complications. However, other abnormal lab tests, such as liver enzymes, serum total bilirubin, or ammonia levels, may have a poor correlation with the severity of liver disease and functional ability. A liver biopsy may demonstrate the degree of liver cell necrosis, inflammation, fibrosis, and cirrhosis. If you have had a liver biopsy, we will make every reasonable effort to obtain the results; however, we will not purchase a liver biopsy. Imaging studies (CAT scan, ultrasound, MRI) may show the size and consistency (fatty liver, scarring) of the liver and document ascites (see 105.00D6).
4. Chronic viral hepatitis infections.
a. General.
(i) Chronic viral hepatitis infections are commonly caused by hepatitis C virus (HCV), and to a lesser extent, hepatitis B virus (HBV). Usually, these are slowly progressive disorders that persist over many years during which the symptoms and signs are typically nonspecific, intermittent, and mild (for example, fatigue, difficulty with concentration, or right upper quadrant pain). Laboratory findings (liver enzymes, imaging studies, liver biopsy pathology) and complications are generally similar in HCV and HBV. The spectrum of these chronic viral hepatitis infections ranges widely and includes an asymptomatic state; insidious disease with mild to moderate symptoms associated with fluctuating liver tests; extrahepatic manifestations; cirrhosis, both compensated and decompensated; ESLD with the need for liver transplantation; and liver cancer. Treatment for chronic viral hepatitis infections varies considerably based on age, medication tolerance, treatment response, adverse effects of treatment, and duration of the treatment. Comorbid disorders, such as HIV infection, may accelerate the clinical course of viral hepatitis infection(s) or may result in a poorer response to medical treatment.
(ii) We evaluate all types of chronic viral hepatitis infections under 105.05 or any listing in an affected body system(s). If your impairment(s) does not meet or medically equal a listing, we will consider the effects of your hepatitis when we assess whether your impairment(s) functionally equals the listings.
b. Chronic hepatitis B virus (HBV) infection.
(i) Chronic HBV infection can be diagnosed by the detection of hepatitis B surface antigen (HBsAg) or hepatitis B virus DNA (HBV DNA) in the blood for at least 6 months. In addition, detection of the hepatitis B e antigen (HBeAg) suggests an increased likelihood of progression to cirrhosis, ESLD, and hepatocellular carcinoma. (HBeAg may also be referred to as “hepatitis B early antigen” or “hepatitis B envelope antigen.”)
(ii) The therapeutic goal of treatment is to suppress HBV replication and thereby prevent progression to cirrhosis, ESLD, and hepatocellular carcinoma. Treatment usually includes interferon injections, oral antiviral agents, or a combination of both. Common adverse effects of treatment are the same as noted in 105.00D4c(ii) for HCV, and generally end within a few days after treatment is discontinued.
c. Chronic hepatitis C virus (HCV) infection.
(i) Chronic HCV infection is diagnosed by the detection of hepatitis C viral RNA in the blood for at least 6 months. Documentation of the therapeutic response to treatment is also monitored by the quantitative assay of serum HCV RNA (“HCV viral load”). Treatment usually includes a combination of interferon injections and oral ribavirin; whether a therapeutic response has occurred is usually assessed after 12 weeks of treatment by checking the HCV viral load. If there has been a substantial reduction in HCV viral load (also known as early viral response, or EVR), this reduction is predictive of a sustained viral response with completion of treatment. Combined therapy is commonly discontinued after 12 weeks when there is no early viral response, since in that circumstance there is little chance of obtaining a sustained viral response (SVR). Otherwise, treatment is usually continued for a total of 48 weeks.
(ii) Combined interferon and ribavirin treatment may have significant adverse effects that may require dosing reduction, planned interruption of treatment, or discontinuation of treatment. Adverse effects may include: Anemia (ribavirin-induced hemolysis), neutropenia, thrombocytopenia, fever, cough, fatigue, myalgia, arthralgia, nausea, loss of appetite, pruritis, and insomnia. Behavioral side effects may also occur. Influenza-like symptoms are generally worse in the first 4 to 6 hours after each interferon injection and during the first weeks of treatment. Adverse effects generally end within a few days after treatment is discontinued.
d. Extrahepatic manifestations of HBV and HCV. In addition to their hepatic manifestations, both HBV and HCV may have significant extrahepatic manifestations in a variety of body systems. These include, but are not limited to: Keratoconjunctivitis (sicca syndrome), glomerulonephritis, skin disorders (for example, lichen planus, porphyria cutanea tarda), neuropathy, and immune dysfunction (for example, cryoglobulinemia, Sjögren's syndrome, and vasculitis). The extrahepatic manifestations of HBV and HCV may not correlate with the severity of your hepatic impairment. If your impairment(s) does not meet or medically equal a listing in an affected body system(s), we will consider the effects of your extrahepatic manifestations when we determine whether your impairment(s) functionally equals the listings.
5. Gastrointestinal hemorrhage (105.02 and 105.05A). Gastrointestinal hemorrhaging can result in hematemesis (vomiting of blood), melena (tarry stools), or hematochezia (bloody stools). Under 105.02, the required transfusions of at least 10 cc of blood/kg of body weight must be at least 30 days apart and occur at least three times during a consecutive 6-month period. Under 105.05A, hemodynamic instability is diagnosed with signs such as pallor (pale skin), diaphoresis (profuse perspiration), rapid pulse, low blood pressure, postural hypotension (pronounced fall in blood pressure when arising to an upright position from lying down) or syncope (fainting). Hemorrhaging that results in hemodynamic instability is potentially life-threatening and therefore requires hospitalization for transfusion and supportive care. Under 105.05A, we require only one hospitalization for transfusion of at least 10 cc of blood/kg of body weight.
6. Ascites or hydrothorax (105.05B) indicates significant loss of liver function due to chronic liver disease. We evaluate ascites or hydrothorax that is not attributable to other causes under 105.05B. The required findings must be present on at least two evaluations at least 60 days apart within a consecutive 6-month period and despite continuing treatment as prescribed.
7. Spontaneous bacterial peritonitis (105.05C) is an infectious complication of chronic liver disease. It is diagnosed by ascitic peritoneal fluid that is documented to contain an absolute neutrophil count of at least 250 cells/mm3. The required finding in 105.05C is satisfied with one evaluation documenting peritoneal fluid infection. We do not evaluate other causes of peritonitis that are unrelated to chronic liver disease, such as tuberculosis, malignancy, and perforated bowel, under this listing. We evaluate these other causes of peritonitis under the appropriate body system listings.
8. Hepatorenal syndrome (105.05D) is defined as functional renal failure associated with chronic liver disease in the absence of underlying kidney pathology. Hepatorenal syndrome is documented by elevation of serum creatinine, marked sodium retention, and oliguria (reduced urine output). The requirements of 105.05D are satisfied with documentation of any one of the three laboratory findings on one evaluation. We do not evaluate known causes of renal dysfunction, such as glomerulonephritis, tubular necrosis, drug-induced renal disease, and renal infections, under this listing. We evaluate these other renal impairments under 106.00ff.
9. Hepatopulmonary syndrome (105.05E) is defined as arterial deoxygenation (hypoxemia) that is associated with chronic liver disease due to intrapulmonary arteriovenous shunting and vasodilatation, in the absence of other causes of arterial deoxygenation. Clinical manifestations usually include dyspnea, orthodeoxia (increasing hypoxemia with erect position), platypnea (improvement of dyspnea with flat position), cyanosis, and clubbing. The requirements of 105.05E are satisfied with documentation of any one of the findings on one evaluation. In 105.05E1, we require documentation of the altitude of the testing facility because altitude affects the measurement of arterial oxygenation. We will not purchase the specialized studies described in 105.05E2; however, if you have had these studies at a time relevant to your claim, we will make every reasonable effort to obtain the reports for the purpose of establishing whether your impairment meets 105.05E2.
10. Hepatic encephalopathy (105.05F).
a. General. Hepatic encephalopathy usually indicates severe loss of hepatocellular function. We define hepatic encephalopathy under 105.05F as a recurrent or chronic neuropsychiatric disorder, characterized by abnormal behavior, cognitive dysfunction, altered state of consciousness, and ultimately coma and death. The diagnosis is established by changes in mental status associated with fleeting neurological signs, including “flapping tremor” (asterixis), characteristic electroencephalographic (EEG) abnormalities, or abnormal laboratory values that indicate loss of synthetic liver function. We will not purchase the EEG testing described in 105.05F3b. However, if you have had this test at a time relevant to your claim, we will make every reasonable effort to obtain the report for the purpose of establishing whether your impairment meets 105.05F.
b. Acute encephalopathy. We will not evaluate your acute encephalopathy under 105.05F if it results from conditions other than chronic liver disease, such as vascular events and neoplastic diseases. We will evaluate these other causes of acute encephalopathy under the appropriate body system listings.
11. End stage liver disease (ESLD) documented by scores from the SSA Chronic Liver Disease (SSA CLD) calculation (105.05G1) and SSA Chronic Liver Disease-Pediatric (SSA CLD-P) calculation (105.05G2).
a. SSA CLD score.
(i) If you are age 12 or older, we will use the SSA CLD score to evaluate your ESLD under 105.05G1. We explain how we calculate the SSA CLD score in a(ii) through a(vii) of this section.
(ii) To calculate the SSA CLD score, we use a formula that includes three laboratory values: Serum total bilirubin (mg/dL), serum creatinine (mg/dL), and International Normalized Ratio (INR). The formula for the SSA CLD score calculation is:
9.57 × [Loge (serum creatinine mg/dL)]
+ 3.78 × [Loge (serum total bilirubin mg/dL)]
+ 11.2 × [Loge (INR)]
+ 6.43
(iii) When we indicate “Loge” in the formula for the SSA CLD score calculation, we mean the “base e logarithm” or “natural logarithm” (ln) of a numerical laboratory value, not the “base 10 logarithm” or “common logarithm” (log) of the laboratory value, and not the actual laboratory value. For an example of SSA CLD calculation, see 5.00D11c.
(iv) For any SSA CLD score calculation, all of the required laboratory values must have been obtained within 30 days of each other. If there are multiple laboratory values within the 30-day interval for any given laboratory test (serum total bilirubin, serum creatinine, or INR), we will use the highest value for the SSA CLD score calculation. We will round all laboratory values less than 1.0 up to 1.0.
(v) Listing 105.05G requires two SSA CLD scores. The laboratory values for the second SSA CLD score calculation must have been obtained at least 60 days after the latest laboratory value for the first SSA CLD score and within the required 6-month period. We will consider the date of each SSA CLD score to be the date of the first laboratory value used for its calculation.
(vi) If you are in renal failure or on dialysis within a week of any serum creatinine test in the period used for the SSA CLD calculation, we will use a serum creatinine of 4, which is the maximum serum creatinine level allowed in the calculation, to calculate your SSA CLD score.
(vii) If you have the two SSA CLD scores required by 105.05G1, we will find that your impairment meets the criteria of the listing from at least the date of the first SSA CLD score.
b. SSA CLD-P score.
(i) If you have not attained age 12, we will use the SSA CLD-P score to evaluate your ESLD under 105.05G2. We explain how we calculate the SSA CLD-P score in b(ii) through b(vii) of this section.
(ii) To calculate the SSA CLD-P score, we use a formula that includes four parameters: Serum total bilirubin (mg/dL), International Normalized Ratio (INR), serum albumin (g/dL), and whether growth failure is occurring. The formula for the SSA CLD-P score calculation is:
4.80 × [Loge (serum total bilirubin mg/dL)]
+ 18.57 × [Loge (INR)]
−6.87 × [Loge (serum albumin g/dL)]
+ 6.67 if the child has growth failure (<−2 standard deviations for weight or height)
(iii) When we indicate “Loge” in the formula for the SSA CLD-P score calculation, we mean the “base e logarithm” or “natural logarithm” (ln) of a numerical laboratory value, not the “base 10 logarithm” or “common logarithm” (log) of the laboratory value, and not the actual laboratory value. For example, if a female child is 4.0 years old, has a current weight of 13.5 kg (10th percentile for age) and height of 92 cm (less than the third percentile for age), and has laboratory values of serum total bilirubin 2.2 mg/dL, INR 1.0, and serum albumin 3.5 g/dL, we will compute the SSA CLD-P score as follows:
4.80 × [Loge + (serum total bilirubin 2.2 mg/dL) = 0.788]
+ 18.57 × [Loge (INR 1.0) = 0]
−6.87 × [Loge + (serum albumin 3.5 g/dL) = 1.253]
+ 6.67
___
= 3.78 + 0 − 8.61 + 6.67
= 1.84, which is then rounded to an SSA CLD-P score of 2
(iv) For any SSA CLD-P score calculation, all of the required laboratory values (serum total bilirubin, INR, or serum albumin) must have been obtained within 30 days of each other. We will not purchase INR values for children who have not attained age 12. If there is no INR value for a child under 12 within the applicable time period, we will use an INR value of 1.1 to calculate the SSA CLD-P score. If there are multiple laboratory values within the 30-day interval for any given laboratory test, we will use the highest serum total bilirubin and INR values and the lowest serum albumin value for the SSA CLD-P score calculation. We will round all laboratory values less than 1.0 up to 1.0.
(v) The weight and length/height measurements used for the calculation must be obtained from one evaluation within the same 30-day period as in D11b(iv).
(vi) Listing 105.05G2 requires two SSA CLD-P scores. The laboratory values for the second SSA CLD-P score calculation must have been obtained at least 60 days after the latest laboratory value for the first SSA CLD-P score and within the required 6-month period. We will consider the date of each SSA CLD-P score to be the date of the first laboratory value used for its calculation.
(vii) If you have the two SSA CLD-P scores required by listing 105.05G2, we will find that your impairment meets the criteria of the listing from at least the date of the first SSA CLD-P score.
12. Extrahepatic biliary atresia (EBA) (105.05H) usually presents in the first 2 months of life with persistent jaundice. The impairment meets 105.05H if the diagnosis of EBA is confirmed by liver biopsy or intraoperative cholangiogram that shows obliteration of the extrahepatic biliary tree. EBA is usually surgically treated by portoenterostomy (for example, Kasai procedure). If this surgery is not performed in the first months of life or is not completely successful, liver transplantation is indicated. If you have had a liver transplant, we will evaluate your impairment under 105.09.
13. Liver transplantation (105.09) may be performed for metabolic liver disease, progressive liver failure, life-threatening complications of liver disease, hepatic malignancy, and acute fulminant hepatitis (viral, drug-induced, or toxin-induced). We will consider you to be disabled for 1 year from the date of the transplantation. Thereafter, we will evaluate your residual impairment(s) by considering the adequacy of post-transplant liver function, the requirement for post-transplant antiviral therapy, the frequency and severity of rejection episodes, comorbid complications, and all adverse treatment effects.
E. How do we evaluate inflammatory bowel disease (IBD)?
1. Inflammatory bowel disease (105.06) includes, but is not limited to, Crohn's disease and ulcerative colitis. These disorders, while distinct entities, share many clinical, laboratory, and imaging findings, as well as similar treatment regimens. Remissions and exacerbations of variable duration are the hallmark of IBD. Crohn's disease may involve the entire alimentary tract from the mouth to the anus in a segmental, asymmetric fashion. Obstruction, stenosis, fistulization, perineal involvement, and extraintestinal manifestations are common. Crohn's disease is rarely curable and recurrence may be a lifelong problem, even after surgical resection. In contrast, ulcerative colitis only affects the colon. The inflammatory process may be limited to the rectum, extend proximally to include any contiguous segment, or involve the entire colon. Ulcerative colitis may be cured by total colectomy.
2. Symptoms and signs of IBD include diarrhea, fecal incontinence, rectal bleeding, abdominal pain, fatigue, fever, nausea, vomiting, arthralgia, abdominal tenderness, palpable abdominal mass (usually inflamed loops of bowel) and perineal disease. You may also have signs or laboratory findings indicating malnutrition, such as weight loss, edema, anemia, hypoalbuminemia, hypokalemia, hypocalcemia, or hypomagnesemia.
3. IBD may be associated with significant extraintestinal manifestations in a variety of body systems. These include, but are not limited to, involvement of the eye (for example, uveitis, episcleritis, iritis); hepatobiliary disease (for example, gallstones, primary sclerosing cholangitis); urologic disease (for example, kidney stones, obstructive hydronephrosis); skin involvement (for example, erythema nodosum, pyoderma gangrenosum); or non-destructive inflammatory arthritis. You may also have associated thromboembolic disorders or vascular disease. These manifestations may not correlate with the severity of your IBD. If your impairment does not meet any of the criteria of 105.06, we will consider the effects of your extraintestinal manifestations in determining whether you have an impairment(s) that meets or medically equals another listing, and we will also consider the effects of your extraintestinal manifestations when we determine whether your impairment(s) functionally equals the listings.
4. Surgical diversion of the intestinal tract, including ileostomy and colostomy, does not very seriously interfere with age-appropriate functioning if you are able to maintain adequate nutrition and function of the stoma. However, if you are not able to maintain adequate nutrition, we will evaluate your impairment under 105.08.
F. How do we evaluate short bowel syndrome (SBS)?
1. Short bowel syndrome (105.07) is a disorder that occurs when congenital intestinal abnormalities, ischemic vascular insults (for example, necrotizing enterocolitis, volvulus), trauma, or IBD complications require surgical resection of more than one-half of the small intestine, resulting in the loss of intestinal absorptive surface and a state of chronic malnutrition. The management of SBS requires long-term parenteral nutrition via an indwelling central venous catheter (central line); the process is often referred to as hyperalimentation or total parenteral nutrition (TPN). Children with SBS can also feed orally, with variable amounts of nutrients being absorbed through their remaining intestine. Over time, some of these children can develop additional intestinal absorptive surface, and may ultimately be able to be weaned off their parenteral nutrition.
2. Your impairment will continue to meet 105.07 as long as you remain dependent on daily parenteral nutrition via a central venous catheter for most of your nutritional requirements. Long-term complications of SBS and parenteral nutrition include abnormal growth rates, central line infections (with or without septicemia), thrombosis, hepatotoxicity, gallstones, and loss of venous access sites. Intestinal transplantation is the only definitive treatment for children with SBS who remain chronically dependent on parenteral nutrition.
3. To document SBS, we need a copy of the operative report of intestinal resection, the summary of the hospitalization(s) including: Details of the surgical findings, medically appropriate postoperative imaging studies that reflect the amount of your residual small intestine, or if we cannot get one of these reports, other medical reports that include details of the surgical findings. We also need medical documentation that you are dependent on daily parenteral nutrition to provide most of your nutritional requirements.
G. How do we evaluate growth failure due to any digestive disorder?
1. To evaluate growth failure due to any digestive disorder, we require documentation of the laboratory findings of chronic nutritional deficiency described in 105.08A and the growth measurements in 105.08B within the same consecutive 12-month period. The dates of laboratory findings may be different from the dates of growth measurements.
2. Under 105.08B, we evaluate a child's growth failure by using the appropriate table for age and gender.
a. For children from birth to attainment of age 2, we use the weight-for-length table (see Table I or Table II).
b. For children age 2 to attainment of age 18, we use the body mass index (BMI)-for-age table (see Tables III or IV).
c. BMI is the ratio of a child's weight to the square of the child's height. We calculate BMI using one of the following formulas:
English Formula
BMI = [Weight in Pounds/(Height in Inches × Height in Inches)] × 703
Metric Formulas
BMI = Weight in Kilograms/(Height in Meters × Height in Meters)
BMI = [Weight in Kilograms/(Height in Centimeters × Height in Centimeters)] × 10,000
H. How do we evaluate the need for supplemental daily enteral feeding via a gastrostomy?
1. General. Infants and young children may have anatomical, neurological, or developmental disorders that interfere with their ability to feed by mouth, resulting in inadequate caloric intake to meet their growth needs. These disorders frequently result in the medical necessity to supplement caloric intake and to bypass the anatomical feeding route of mouth-throat-esophagus into the stomach.
2. Children who have not attained age 3 and who require supplemental daily enteral nutrition via a feeding gastrostomy meet 105.10 regardless of the medical reason for the gastrostomy. Thereafter, we evaluate growth impairment under 100.02, malnutrition under 105.08, or other medical or developmental disorder(s) (including the disorder(s) that necessitated gastrostomy placement) under the appropriate listing(s).
I. How do we evaluate esophageal stricture or stenosis? Esophageal stricture or stenosis (narrowing) from congenital atresia (absence or abnormal closure of a tubular body organ) or destructive esophagitis may result in malnutrition or the need for gastrostomy placement, which we evaluate under 105.08 or 105.10. Esophageal stricture or stenosis may also result in complications such as pneumonias due to frequent aspiration, or difficulty in maintaining nutritional status short of listing-level severity. While none of these complications may be of such severity that they would meet the criteria of another listing, the combination of impairments may medically equal the severity of a listing or functionally equal the listings.
J. What do we mean by the phrase “consider under a disability for 1 year”? We use the phrase “consider under a disability for 1 year” following a specific event in 105.02, 105.05A, and 105.09 to explain how long your impairment can meet the requirements of those particular listings. This phrase does not refer to the date on which your disability began, only to the date on which we must reevaluate whether your impairment continues to meet a listing or is otherwise disabling. For example, if you have received a liver transplant, you may have become disabled before the transplant because of chronic liver disease. Therefore, we do not restrict our determination of the onset of disability to the date of the specified event. We will establish an onset date earlier than the date of the specified event if the evidence in your case record supports such a finding.
K. How do we evaluate impairments that do not meet one of the digestive disorder listings?
1. These listings are only examples of common digestive disorders that we consider severe enough to result in marked and severe functional limitations. If your impairment(s) does not meet the criteria of any of these listings, we must also consider whether you have an impairment(s) that satisfies the criteria of a listing in another body system. For example:
a. If you have hepatitis B or C and you are depressed, we will evaluate your impairment under 112.04.
b. If you have multiple congenital abnormalities, we will evaluate your impairment(s) under the criteria in the listings for impairments that affect multiple body systems (110.00) or the criteria of listings in other affected body systems.
c. If you have digestive disorders that interfere with intake, digestion, or absorption of nutrition, and result in a reduction in your rate of growth, and your impairment does not satisfy the criteria in the malnutrition listing (105.08), we will evaluate your impairment under the growth impairment listings (100.00).
2. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. (See § 416.926.) If your impairment(s) does not meet or medically equal a listing, you may or may not have an impairment(s) that functionally equals the listings. (See § 416.926a.) When we decide whether you continue to be disabled, we use the rules in § 416.994a.
105.01 Category of Impairments, Digestive System
105.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 10 cc of blood/kg of body weight, and occurring at least three times during a consecutive 6-month period. The transfusions must be at least 30 days apart within the 6-month period. Consider under a disability for 1 year following the last documented transfusion; thereafter, evaluate the residual impairment(s).
105.03-105.04 [Reserved]
105.05 Chronic liver disease, with:
A. Hemorrhaging from esophageal, gastric, or ectopic varices or from portal hypertensive gastropathy, demonstrated by endoscopy, x-ray, or other appropriate medically acceptable imaging, resulting in hemodynamic instability as defined in 105.00D5, and requiring hospitalization for transfusion of at least 10 cc of blood/kg of body weight. Consider under a disability for 1 year following the last documented transfusion; thereafter, evaluate the residual impairment(s).
OR
B. Ascites or hydrothorax not attributable to other causes, despite continuing treatment as prescribed, present on at least two evaluations at least 60 days apart within a consecutive 6-month period. Each evaluation must be documented by:
1. Paracentesis or thoracentesis; or
2. Appropriate medically acceptable imaging or physical examination and one of the following:
a. Serum albumin of 3.0 g/dL or less; or
b. International Normalized Ratio (INR) of at least 1.5.
OR
C. Spontaneous bacterial peritonitis with peritoneal fluid containing an absolute neutrophil count of at least 250 cells/mm3.
OR
D. Hepatorenal syndrome as described in 105.00D8, with one of the following:
1. Serum creatinine elevation of at least 2 mg/dL; or
2. Oliguria with 24-hour urine output less than 1 mL/kg/hr; or
3. Sodium retention with urine sodium less than 10 mEq per liter.
OR
E. Hepatopulmonary syndrome as described in 105.00D9, with:
1. Arterial oxygenation (PaO2,) on room air of:
a. 60 mm Hg or less, at test sites less than 3000 feet above sea level, or
b. 55 mm Hg or less, at test sites from 3000 to 6000 feet, or
c. 50 mm Hg or less, at test sites above 6000 feet; or
2. Documentation of intrapulmonary arteriovenous shunting by contrast-enhanced echocardiography or macroaggregated albumin lung perfusion scan.
OR
F. Hepatic encephalopathy as described in 105.00D10, with 1 and either 2 or 3:
1. Documentation of abnormal behavior, cognitive dysfunction, changes in mental status, or altered state of consciousness (for example, confusion, delirium, stupor, or coma), present on at least two evaluations at least 60 days apart within a consecutive 6-month period; and
2. History of transjugular intrahepatic portosystemic shunt (TIPS) or any surgical portosystemic shunt; or
3. One of the following occurring on at least two evaluations at least 60 days apart within the same consecutive 6-month period as in F1:
a. Asterixis or other fluctuating physical neurological abnormalities; or
b. Electroencephalogram (EEG) demonstrating triphasic slow wave activity; or
c. Serum albumin of 3.0 g/dL or less; or
d. International Normalized Ratio (INR) of 1.5 or greater.
OR
G. End Stage Liver Disease, with:
1. For children 12 years of age or older, SSA CLD scores of 22 or greater calculated as described in 105.00D11a. Consider under a disability from at least the date of the first score.
2. For children who have not attained age 12, SSA CLD-P scores of 11 or greater calculated as described in 105.00D11b. Consider under a disability from at least the date of the first score.
OR
H. Extrahepatic biliary atresia as diagnosed on liver biopsy or intraoperative cholangiogram. Consider under a disability for 1 year following the diagnosis; thereafter, evaluate the residual liver function.
105.06 Inflammatory bowel disease (IBD) documented by endoscopy, biopsy, appropriate medically acceptable imaging, or operative findings with:
A. Obstruction of stenotic areas (not adhesions) in the small intestine or colon with proximal dilatation, confirmed by appropriate medically acceptable imaging or in surgery, requiring hospitalization for intestinal decompression or for surgery, and occurring on at least two occasions at least 60 days apart within a consecutive 6-month period;
OR
B. Two of the following despite continuing treatment as prescribed and occurring within the same consecutive 6-month period:
1. Anemia with hemoglobin less than 10.0 g/dL, present on at least two evaluations at least 60 days apart; or
2. Serum albumin of 3.0 g/dL or less, present on at least two evaluations at least 60 days apart; or
3. Clinically documented tender abdominal mass palpable on physical examination with abdominal pain or cramping that is not completely controlled by prescribed narcotic medication, present on at least two evaluations at least 60 days apart; or
4. Perineal disease with a draining abscess or fistula, with pain that is not completely controlled by prescribed narcotic medication, present on at least two evaluations at least 60 days apart; or
5. Need for supplemental daily enteral nutrition via a gastrostomy or daily parenteral nutrition via a central venous catheter. (See 105.10 for children who have not attained age 3.)
105.07 Short bowel syndrome (SBS), due to surgical resection of more than one-half of the small intestine, with dependence on daily parenteral nutrition via a central venous catheter (see 105.00F).
105.08 Growth failure due to any digestive disorder (see 105.00G), documented by A and B:
A. Chronic nutritional deficiency present on at least two evaluations at least 60 days apart within a consecutive 12-month period documented by one of the following:
1. Anemia with hemoglobin less than 10.0 g/dL; or
2. Serum albumin of 3.0 g/dL or less;
AND
B. Growth failure as required in 1 or 2:
1. For children from birth to attainment of age 2, three weight-for-length measurements that are:
a. Within a 12-month period; and
b. At least 60 days apart; and
c. Less than the third percentile on Table I or Table II; or
Table I - Males Birth to Attainment of Age 2
[Third Percentile Values for Weight-for-Length]
| Length
(centimeters) | Weight
(kilograms) | Length
(centimeters) | Weight
(kilograms) | Length
(centimeters) | Weight
(kilograms) |
|---|---|---|---|---|---|
| 45.0 | 1.597 | 64.5 | 6.132 | 84.5 | 10.301 |
| 45.5 | 1.703 | 65.5 | 6.359 | 85.5 | 10.499 |
| 46.5 | 1.919 | 66.5 | 6.584 | 86.5 | 10.696 |
| 47.5 | 2.139 | 67.5 | 6.807 | 87.5 | 10.895 |
| 48.5 | 2.364 | 68.5 | 7.027 | 88.5 | 11.095 |
| 49.5 | 2.592 | 69.5 | 7.245 | 89.5 | 11.296 |
| 50.5 | 2.824 | 70.5 | 7.461 | 90.5 | 11.498 |
| 51.5 | 3.058 | 71.5 | 7.674 | 91.5 | 11.703 |
| 52.5 | 3.294 | 72.5 | 7.885 | 92.5 | 11.910 |
| 53.5 | 3.532 | 73.5 | 8.094 | 93.5 | 12.119 |
| 54.5 | 3.771 | 74.5 | 8.301 | 94.5 | 12.331 |
| 55.5 | 4.010 | 75.5 | 8.507 | 95.5 | 12.546 |
| 56.5 | 4.250 | 76.5 | 8.710 | 96.5 | 12.764 |
| 57.5 | 4.489 | 77.5 | 8.913 | 97.5 | 12.987 |
| 58.5 | 4.728 | 78.5 | 9.113 | 98.5 | 13.213 |
| 59.5 | 4.966 | 79.5 | 9.313 | 99.5 | 13.443 |
| 60.5 | 5.203 | 80.5 | 9.512 | 100.5 | 13.678 |
| 61.5 | 5.438 | 81.5 | 9.710 | 101.5 | 13.918 |
| 62.5 | 5.671 | 82.5 | 9.907 | 102.5 | 14.163 |
| 63.5 | 5.903 | 83.5 | 10.104 | 103.5 | 14.413 |
Table II - Females Birth to Attainment of Age 2
[Third percentile values for weight-for-length]
| Length
(centimeters) | Weight
(kilograms) | Length
(centimeters) | Weight
(kilograms) | Length
(centimeters) | Weight
(kilograms) |
|---|---|---|---|---|---|
| 45.0 | 1.613 | 64.5 | 5.985 | 84.5 | 10.071 |
| 45.5 | 1.724 | 65.5 | 6.200 | 85.5 | 10.270 |
| 46.5 | 1.946 | 66.5 | 6.413 | 86.5 | 10.469 |
| 47.5 | 2.171 | 67.5 | 6.625 | 87.5 | 10.670 |
| 48.5 | 2.397 | 68.5 | 6.836 | 88.5 | 10.871 |
| 49.5 | 2.624 | 69.5 | 7.046 | 89.5 | 11.074 |
| 50.5 | 2.852 | 70.5 | 7.254 | 90.5 | 11.278 |
| 51.5 | 3.081 | 71.5 | 7.461 | 91.5 | 11.484 |
| 52.5 | 3.310 | 72.5 | 7.667 | 92.5 | 11.691 |
| 53.5 | 3.538 | 73.5 | 7.871 | 93.5 | 11.901 |
| 54.5 | 3.767 | 74.5 | 8.075 | 94.5 | 12.112 |
| 55.5 | 3.994 | 75.5 | 8.277 | 95.5 | 12.326 |
| 56.5 | 4.220 | 76.5 | 8.479 | 96.5 | 12.541 |
| 57.5 | 4.445 | 77.5 | 8.679 | 97.5 | 12.760 |
| 58.5 | 4.669 | 78.5 | 8.879 | 98.5 | 12.981 |
| 59.5 | 4.892 | 79.5 | 9.078 | 99.5 | 13.205 |
| 60.5 | 5.113 | 80.5 | 9.277 | 100.5 | 13.431 |
| 61.5 | 5.333 | 81.5 | 9.476 | 101.5 | 13.661 |
| 62.5 | 5.552 | 82.5 | 9.674 | 102.5 | 13.895 |
| 63.5 | 5.769 | 83.5 | 9.872 | 103.5 | 14.132 |
2. For children age 2 to attainment of age 18, three BMI-for-age measurements that are:
a. Within a consecutive 12-month period; and
b. At least 60 days apart; and
c. Less than the third percentile on Table III or Table IV.
Table III - Males Age 2 to Attainment of Age 18
[Third Percentile Values for BMI-for-Age]
| Age
(yrs. and mos.) | BMI | Age
(yrs. and mos.) | BMI | Age
(yrs. and mos.) | BMI |
|---|---|---|---|---|---|
| 2.0 to 2.1 | 14.5 | 10.11 to 11.2 | 14.3 | 14.9 to 14.10 | 16.1 |
| 2.2 to 2.4 | 14.4 | 11.3 to 11.5 | 14.4 | 14.11 to 15.0 | 16.2 |
| 2.5 to 2.7 | 14.3 | 11.6 to 11.8 | 14.5 | 15.1 to 15.3 | 16.3 |
| 2.8 to 2.11 | 14.2 | 11.9 to 11.11 | 14.6 | 15.4 to 15.5 | 16.4 |
| 3.0 to 3.2 | 14.1 | 12.0 to 12.1 | 14.7 | 15.6 to 15.7 | 16.5 |
| 3.3 to 3.6 | 14.0 | 12.2 to 12.4 | 14.8 | 15.8 to 15.9 | 16.6 |
| 3.7 to 3.11 | 13.9 | 12.5 to 12.7 | 14.9 | 15.10 to 15.11 | 16.7 |
| 4.0 to 4.5 | 13.8 | 12.8 to 12.9 | 15.0 | 16.0 to 16.1 | 16.8 |
| 4.6 to 5.0 | 13.7 | 12.10 to 13.0 | 15.1 | 16.2 to 16.3 | 16.9 |
| 5.1 to 6.0 | 13.6 | 13.1 to 13.2 | 15.2 | 16.4 to 16.5 | 17.0 |
| 6.1 to 7.6 | 13.5 | 13.3 to 13.4 | 15.3 | 16.6 to 16.8 | 17.1 |
| 7.7 to 8.6 | 13.6 | 13.5 to 13.7 | 15.4 | 16.9 to 16.10 | 17.2 |
| 8.7 to 9.1 | 13.7 | 13.8 to 13.9 | 15.5 | 16.11 to 17.0 | 17.3 |
| 9.2 to 9.6 | 13.8 | 13.10 to 13.11 | 15.6 | 17.1 to 17.2 | 17.4 |
| 9.7 to 9.11 | 13.9 | 14.0 to 14.1 | 15.7 | 17.3 to 17.5 | 17.5 |
| 10.0 to 10.3 | 14.0 | 14.2 to 14.4 | 15.8 | 17.6 to 17.7 | 17.6 |
| 10.4 to 10.7 | 14.1 | 14.5 to 14.6 | 15.9 | 17.8 to 17.9 | 17.7 |
| 10.8 to 10.10 | 14.2 | 14.7 to 14.8 | 16.0 | 17.10 to 17.11 | 17.8 |
Table IV - Females Age 2 to Attainment of Age 18
[Third Percentile Values for BMI-for-Age]
| Age
(yrs. and mos.) | BMI | Age
(yrs. and mos.) | BMI | Age
(yrs. and mos.) | BMI |
|---|---|---|---|---|---|
| 2.0 to 2.2 | 14.1 | 10.8 to 10.10 | 14.0 | 14.3 to 14.5 | 15.6 |
| 2.3 to 2.6 | 14.0 | 10.11 to 11.2 | 14.1 | 14.6 to 14.7 | 15.7 |
| 2.7 to 2.10 | 13.9 | 11.3 to 11.5 | 14.2 | 14.8 to 14.9 | 15.8 |
| 2.11 to 3.2 | 13.8 | 11.6 to 11.7 | 14.3 | 14.10 to 15.0 | 15.9 |
| 3.3 to 3.6 | 13.7 | 11.8 to 11.10 | 14.4 | 15.1 to 15.2 | 16.0 |
| 3.7 to 3.11 | 13.6 | 11.11 to 12.1 | 14.5 | 15.3 to 15.5 | 16.1 |
| 4.0 to 4.4 | 13.5 | 12.2 to 12.4 | 14.6 | 15.6 to 15.7 | 16.2 |
| 4.5 to 4.11 | 13.4 | 12.5 to 12.6 | 14.7 | 15.8 to 15.10 | 16.3 |
| 5.0 to 5.9 | 13.3 | 12.7 to 12.9 | 14.8 | 15.11 to 16.0 | 16.4 |
| 5.10 to 7.6 | 13.2 | 12.10 to 12.11 | 14.9 | 16.1 to 16.3 | 16.5 |
| 7.7 to 8.4 | 13.3 | 13.0 to 13.2 | 15.0 | 16.4 to 16.6 | 16.6 |
| 8.5 to 8.10 | 13.4 | 13.3 to 13.4 | 15.1 | 16.7 to 16.9 | 16.7 |
| 8.11 to 9.3 | 13.5 | 13.5 to 13.7 | 15.2 | 16.10 to 17.0 | 16.8 |
| 9.4 to 9.8 | 13.6 | 13.8 to 13.9 | 15.3 | 17.1 to 17.3 | 16.9 |
| 9.9 to 10.0 | 13.7 | 13.10 to 14.0 | 15.4 | 17.4 to 17.7 | 17.0 |
| 10.1 to 10.4 | 13.8 | 14.1 to 14.2 | 15.5 | 17.8 to 17.11 | 17.1 |
| 10.5 to 10.7 | 13.9 |
105.09 Liver transplantation. Consider under a disability for 1 year following the date of transplantation; thereafter, evaluate the residual impairment(s) (see 105.00D13 and 105.00J).
105.10 Need for supplemental daily enteral feeding via a gastrostomy due to any cause, for children who have not attained age 3; thereafter, evaluate the residual impairment(s) (see 105.00H).
106.00 Genitourinary Disorders
A. Which disorders do we evaluate under these listings?
We evaluate genitourinary disorders resulting in chronic kidney disease (CKD). Examples of such disorders include chronic glomerulonephritis, hypertensive nephropathy, diabetic nephropathy, chronic obstructive uropathy, and hereditary nephropathies. We also evaluate nephrotic syndrome due to glomerular dysfunction, and congenital genitourinary disorders, such as ectopic ureter, exstrophic urinary bladder, urethral valves, and Eagle-Barrett syndrome (prune belly syndrome), under these listings.
B. What evidence do we need?
1. We need evidence that documents the signs, symptoms, and laboratory findings of your CKD. This evidence should include reports of clinical examinations, treatment records, and documentation of your response to treatment. Laboratory findings, such as serum creatinine or serum albumin levels, may document your kidney function. We generally need evidence covering a period of at least 90 days unless we can make a fully favorable determination or decision without it.
2. Estimated glomerular filtration rate (eGFR). The eGFR is an estimate of the filtering capacity of the kidneys that takes into account serum creatinine concentration and other variables, such as your age, gender, and body size. If your medical evidence includes eGFR findings, we will consider them when we evaluate your CKD under 106.05.
3. Kidney or bone biopsy. If you have had a kidney or bone biopsy, we need a copy of the pathology report. When we cannot get a copy of the pathology report, we will accept a statement from an acceptable medical source verifying that a biopsy was performed and describing the results.
C. What other factors do we consider when we evaluate your genitourinary disorder?
1. Chronic hemodialysis or peritoneal dialysis.
a. Dialysis is a treatment for CKD that uses artificial means to remove toxic metabolic byproducts from the blood. Hemodialysis uses an artificial kidney machine to clean waste products from the blood; peritoneal dialysis uses a dialyzing solution that is introduced into and removed from the abdomen (peritoneal cavity) either continuously or intermittently. Under 106.03, your ongoing dialysis must have lasted or be expected to last for a continuous period of at least 12 months. To satisfy the requirement in 106.03, we will accept a report from an acceptable medical source that describes your CKD and your current dialysis, and indicates that your dialysis will be ongoing.
b. If you are undergoing chronic hemodialysis or peritoneal dialysis, your CKD may meet our definition of disability before you started dialysis. We will determine the onset of your disability based on the facts in your case record.
2. Kidney transplant.
a. If you receive a kidney transplant, we will consider you to be disabled under 106.04 for 1 year from the date of transplant. After that, we will evaluate your residual impairment(s) by considering your post-transplant function, any rejection episodes you have had, complications in other body systems, and any adverse effects related to ongoing treatment.
b. If you received a kidney transplant, your CKD may meet our definition of disability before you received the transplant. We will determine the onset of your disability based on the facts in your case record.
3. Anasarca (generalized massive edema or swelling). Under 106.06B, we need a description of the extent of edema, including pretibial (in front of the tibia), periorbital (around the eyes), or presacral (in front of the sacrum) edema. We also need a description of any ascites, pleural effusion, or pericardial effusion.
4. Congenital genitourinary disorder. Procedures such as diagnostic cystoscopy or circumcision do not satisfy the requirement for urologic surgical procedures in 106.07.
5. Growth failure due to any chronic renal disease.
a. To evaluate growth failure due to any chronic renal disease, we require documentation of the laboratory findings described in 106.08A and the growth measurements in 106.08B within the same consecutive 12-month period. The dates of laboratory findings may be different from the dates of growth measurements.
b. Under 106.08B, we use the appropriate table(s) under 105.08B in the digestive system to determine whether a child's growth is less than the third percentile.
(i) For children from birth to attainment of age 2, we use the weight-for-length table corresponding to the child's gender (Table I or Table II).
(ii) For children age 2 to attainment of age 18, we use the body mass index (BMI)-for-age table corresponding to the child's gender (Table III or Table IV).
(iii) BMI is the ratio of a child's weight to the square of his or her height. We calculate BMI using the formulas in 105.00G2c.
6. Complications of CKD. The hospitalizations in 106.09 may be for different complications of CKD. Examples of complications from CKD that may result in hospitalization include stroke, congestive heart failure, hypertensive crisis, or acute kidney failure requiring a short course of hemodialysis. If the CKD complication occurs during a hospitalization that was initially for a co-occurring condition, we will evaluate it under our rules for determining medical equivalence. (See § 416.926 of this chapter.) We will evaluate co-occurring conditions, including those that result in hospitalizations, under the listings for the affected body system or under our rules for medical equivalence.
D. How do we evaluate disorders that do not meet one of the genitourinary listings?
1. The listed disorders are only examples of common genitourinary disorders that we consider severe enough to result in marked and severe functional limitations. If your impairment(s) does not meet the criteria of any of these listings, we must also consider whether you have an impairment(s) that satisfies the criteria of a listing in another body system.
2. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. (See § 416.926 of this chapter.) Genitourinary disorders may be associated with disorders in other body systems, and we consider the combined effects of multiple impairments when we determine whether they medically equal a listing. If your impairment(s) does not medically equal a listing, we will also consider whether it functionally equals the listings. (See § 416.926a of this chapter.) We use the rules in § 416.994a of this chapter when we decide whether you continue to be disabled.
106.01 Category of Impairments, Genitourinary Disorders
106.03 Chronic kidney disease, with chronic hemodialysis or peritoneal dialysis (see 106.00C1).
106.04 Chronic kidney disease, with kidney transplant. Consider under a disability for 1 year following the transplant; thereafter, evaluate the residual impairment (see 106.00C2).
106.05 Chronic kidney disease, with impairment of kidney function, with one of the following documented on at least two occasions at least 90 days apart during a consecutive 12-month period:
A. Serum creatinine of 3 mg/dL or greater;
OR
B. Creatinine clearance of 30 ml/min/1.73m2 or less;
OR
C. Estimated glomerular filtration rate (eGFR) of 30 ml/min/1.73m2 or less.
106.06 Nephrotic syndrome, with A and B:
A. Laboratory findings as described in 1 or 2, documented on at least two occasions at least 90 days apart during a consecutive 12-month period:
1. Serum albumin of 3.0 g/dL or less, or
2. Proteinuria of 40 mg/m2/hr or greater;
AND
B. Anasarca (see 106.00C3) persisting for at least 90 days despite prescribed treatment.
106.07 Congenital genitourinary disorder (see 106.00C4) requiring urologic surgical procedures at least three times in a consecutive 12-month period, with at least 30 days between procedures. Consider under a disability for 1 year following the date of the last surgery; thereafter, evaluate the residual impairment.
106.09 Complications of chronic kidney disease (see 106.00C5) requiring at least three hospitalizations within a consecutive 12-month period and occurring at least 30 days apart. Each hospitalization must last at least 48 hours, including hours in a hospital emergency department immediately before the hospitalization.
106.08 Growth failure due to any chronic renal disease (see 106.00C5), with:
A. Serum creatinine of 2 mg/dL or greater, documented at least two times within a consecutive 12-month period with at least 60 days between measurements.
AND
B. Growth failure as required in 1 or 2:
1. For children from birth to attainment of age 2, three weight-for-length measurements that are:
a. Within a consecutive 12-month period; and
b. At least 60 days apart; and
c. Less than the third percentile on the appropriate weight-for-length table under 105.08B1; or
2. For children age 2 to attainment of age 18, three BMI-for-age measurements that are:
a. Within a consecutive 12-month period; and
b. At least 60 days apart; and
c. Less than the third percentile on the appropriate BMI-for-age table under 105.08B2.
107.00 Hematological Disorders
A. What hematological disorders do we evaluate under these listings?
1. We evaluate non-malignant (non-cancerous) hematological disorders, such as hemolytic anemias (107.05), disorders of thrombosis and hemostasis (107.08), and disorders of bone marrow failure (107.10). These disorders disrupt the normal development and function of white blood cells, red blood cells, platelets, and clotting-factor proteins (factors).
2. We evaluate malignant (cancerous) hematological disorders, such as lymphoma, leukemia, and multiple myeloma, under the appropriate listings in 113.00, except for two lymphomas associated with human immunodeficiency virus (HIV) infection. We evaluate primary central nervous system lymphoma associated with HIV infection under 114.11B, and primary effusion lymphoma associated with HIV infection under 114.11C.
B. What evidence do we need to document that you have a hematological disorder?
We need the following evidence to document that you have a hematological disorder:
1. A laboratory report of a definitive test that establishes a hematological disorder, signed by a physician; or
2. A laboratory report of a definitive test that establishes a hematological disorder that is not signed by a physician and a report from a physician that states you have the disorder; or
3. When we do not have a laboratory report of a definitive test, a persuasive report from a physician that a diagnosis of your hematological disorder was confirmed by appropriate laboratory analysis or other diagnostic method(s). To be persuasive, this report must state that you had the appropriate definitive laboratory test or tests for diagnosing your disorder and provide the results, or explain how your diagnosis was established by other diagnostic method(s) consistent with the prevailing state of medical knowledge and clinical practice.
4. We will make every reasonable effort to obtain the results of appropriate laboratory testing you have had. We will not purchase complex, costly, or invasive tests, such as tests of clotting-factor proteins, and bone marrow aspirations.
C. What are hemolytic anemias, and how do we evaluate them under 107.05?
1. Hemolytic anemias, both congenital and acquired, are disorders that result in premature destruction of red blood cells (RBCs). Hemolytic anemias include abnormalities of hemoglobin structure (hemoglobinopathies), abnormal RBC enzyme content and function, and RBC membrane (envelope) defects that are congenital or acquired. The diagnosis of hemolytic anemia is based on hemoglobin electrophoresis or analysis of the contents of the RBC (enzymes) and membrane. Examples of congenital hemolytic anemias include sickle cell disease, thalassemia, and their variants, and hereditary spherocytosis. Acquired hemolytic anemias may result from autoimmune disease (for example, systemic lupus erythematosus) or mechanical devices (for example, heart valves, intravascular patches).
2. The hospitalizations in 107.05B do not all have to be for the same complication of the hemolytic anemia. They may be for three different complications of the disorder. Examples of complications of hemolytic anemia that may result in hospitalization include dactylitis, osteomyelitis, painful (vaso-occlusive) crisis, pulmonary infections or infarctions, acute chest syndrome, pulmonary hypertension, chronic heart failure, gallbladder disease, hepatic (liver) failure, renal (kidney) failure, nephrotic syndrome, aplastic crisis, and strokes. We will count the hours you receive emergency treatment in a comprehensive sickle cell disease center immediately before the hospitalization if this treatment is comparable to the treatment provided in a hospital emergency department.
3. For 107.05C, we do not require hemoglobin to be measured during a period in which you are free of pain or other symptoms of your disorder. We will accept hemoglobin measurements made while you are experiencing complications of your hemolytic anemia.
4. 107.05D refers to the most serious type of beta thalassemia major in which the bone marrow cannot produce sufficient numbers of normal RBCs to maintain life. The only available treatments for beta thalassemia major are life-long RBC transfusions (sometimes called hypertransfusion) or bone marrow transplantation. For purposes of 107.05D, we do not consider prophylactic RBC transfusions to prevent strokes or other complications in sickle cell disease and its variants to be of equal significance to life-saving RBC transfusions for beta thalassemia major. However, we will consider the functional limitations associated with prophylactic RBC transfusions and any associated side effects (for example, iron overload) under functional equivalence and any affected body system(s). We will also evaluate strokes and resulting complications under 111.00 and 112.00.
D. What are disorders of thrombosis and hemostasis, and how do we evaluate them under 107.08?
1. Disorders of thrombosis and hemostasis include both clotting and bleeding disorders, and may be congenital or acquired. These disorders are characterized by abnormalities in blood clotting that result in hypercoagulation (excessive blood clotting) or hypocoagulation (inadequate blood clotting). The diagnosis of a thrombosis or hemostasis disorder is based on evaluation of plasma clotting-factor proteins (factors) and platelets. Protein C or protein S deficiency and Factor V Leiden are examples of hypercoagulation disorders. Hemophilia, von Willebrand disease, and thrombocytopenia are examples of hypocoagulation disorders. Acquired excessive blood clotting may result from blood protein defects and acquired inadequate blood clotting (for example, acquired hemophilia A) may be associated with inhibitor autoantibodies.
2. The hospitalizations in 107.08 do not all have to be for the same complication of a disorder of thrombosis and hemostasis. They may be for three different complications of the disorder. Examples of complications that may result in hospitalization include anemias, thromboses, embolisms, and uncontrolled bleeding requiring multiple factor concentrate infusions or platelet transfusions. We will also consider any surgery that you have, even if it is not related to your hematological disorder, to be a complication of your disorder of thrombosis and hemostasis if you require treatment with clotting-factor proteins (for example, factor VIII or IX) or anticoagulant medication to control bleeding or coagulation in connection with your surgery. We will count the hours you receive emergency treatment in a comprehensive hemophilia treatment center immediately before the hospitalization if this treatment is comparable to the treatment provided in a hospital emergency department.
E. What are disorders of bone marrow failure, and how do we evaluate them under 107.10?
1. Disorders of bone marrow failure may be congenital or acquired, characterized by bone marrow that does not make enough healthy RBCs, platelets, or granulocytes (specialized types of white blood cells); there may also be a combined failure of these bone marrow-producing cells. The diagnosis is based on peripheral blood smears and bone marrow aspiration or bone marrow biopsy, but not peripheral blood smears alone. Examples of these disorders are myelodysplastic syndromes, aplastic anemia, granulocytopenia, and myelofibrosis. Acquired disorders of bone marrow failure may result from viral infections, chemical exposure, or immunologic disorders.
2. The hospitalizations in 107.10A do not all have to be for the same complication of bone marrow failure. They may be for three different complications of the disorder. Examples of complications that may result in hospitalization include uncontrolled bleeding, anemia, and systemic bacterial, viral, or fungal infections.
3. For 107.10B, the requirement of life-long RBC transfusions to maintain life in myelodysplastic syndromes or aplastic anemias has the same meaning as it does for beta thalassemia major. (See 107.00C4.)
F. How do we evaluate bone marrow or stem cell transplantation under 107.17?
We will consider you to be disabled for 12 months from the date of bone marrow or stem cell transplantation, or we may consider you to be disabled for a longer period if you are experiencing any serious post-transplantation complications, such as graft-versus-host (GVH) disease, frequent infections after immunosuppressive therapy, or significant deterioration of organ systems. We do not restrict our determination of the onset of disability to the date of the transplantation in 107.17. We may establish an earlier onset of disability due to your transplantation if evidence in your case record supports such a finding.
G. How do we consider your symptoms, including your pain, severe fatigue, and malaise?
Your symptoms, including pain, severe fatigue, and malaise, may be important factors in our determination whether your hematological disorder meets or medically equals a listing, or in our determination whether you otherwise have marked and severe functional limitations. We cannot consider your symptoms unless you have medical signs or laboratory findings showing the existence of a medically determinable impairment(s) that could reasonably be expected to produce the symptoms. If you have such an impairment(s), we will evaluate the intensity, persistence, and functional effects of your symptoms using the rules throughout 107.00 and in our other regulations. (See sections 416.921 and 416.929 of this chapter.) Additionally, when we assess the credibility of your complaints about your symptoms and their functional effects, we will not draw any inferences from the fact that you do not receive treatment or that you are not following treatment without considering all of the relevant evidence in your case record, including any explanations you provide on why you are not receiving or following treatment.
H. How do we evaluate episodic events in hematological disorders?
Some of the listings in this body system require a specific number of events within a consecutive 12-month period. (See 107.05, 107.08, and 107.10A.) When we use such criteria, a consecutive 12-month period means a period of 12 consecutive months, all or part of which must occur within the period we are considering in connection with your application or continuing disability review. These events must occur at least 30 days apart to ensure that we are evaluating separate events.
I. How do we evaluate hematological disorders that do not meet one of these listings?
1. These listings are only common examples of hematological disorders that we consider severe enough to result in marked and severe functional limitations. If your disorder does not meet the criteria of any of these listings, we must consider whether you have a disorder that satisfies the criteria of a listing in another body system. For example, we will evaluate hemophilic joint deformity under 101.00; polycythemia vera under 103.00, 104.00, or 111.00; chronic iron overload resulting from repeated RBC transfusion (transfusion hemosiderosis) under 103.00, 104.00, or 105.00; and the effects of intracranial bleeding or stroke under 111.00 or 112.00.
2. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. (See section 416.926 of this chapter.) Hematological disorders may be associated with disorders in other body systems, and we consider the combined effects of multiple impairments when we determine whether they medically equal a listing. If your impairment(s) does not medically equal a listing, we will also consider whether it functionally equals the listings. (See section 416.926a of this chapter.) We use the rules in § 416.994a of this chapter when we decide whether you continue to be disabled.
107.01 Category of Impairments, Hematological Disorders
107.05 Hemolytic anemias, including sickle cell disease, thalassemia, and their variants (see 107.00C), with:
A. Documented painful (vaso-occlusive) crises requiring parenteral (intravenous or intramuscular) narcotic medication, occurring at least six times within a 12-month period with at least 30 days between crises.
OR
B. Complications of hemolytic anemia requiring at least three hospitalizations within a 12-month period and occurring at least 30 days apart. Each hospitalization must last at least 48 hours, which can include hours in a hospital emergency department or comprehensive sickle cell disease center immediately before the hospitalization (see 107.00C2).
OR
C. Hemoglobin measurements of 7.0 grams per deciliter (g/dL) or less, occurring at least three times within a 12-month period with at least 30 days between measurements.
OR
D. Beta thalassemia major requiring life-long RBC transfusions at least once every 6 weeks to maintain life (see 107.00C4).
107.08 Disorders of thrombosis and hemostasis, including hemophilia and thrombocytopenia (see 107.00D), with complications requiring at least three hospitalizations within a 12-month period and occurring at least 30 days apart. Each hospitalization must last at least 48 hours, which can include hours in a hospital emergency department or comprehensive hemophilia treatment center immediately before the hospitalization (see 107.00D2).
107.10 Disorders of bone marrow failure, including myelodysplastic syndromes, aplastic anemia, granulocytopenia, and myelofibrosis (see 107.00E), with:
A. Complications of bone marrow failure requiring at least three hospitalizations within a 12-month period and occurring at least 30 days apart. Each hospitalization must last at least 48 hours, which can include hours in a hospital emergency department immediately before the hospitalization (see 107.00E2).
OR
B. Myelodysplastic syndromes or aplastic anemias requiring life-long RBC transfusions at least once every 6 weeks to maintain life (see 107.00E3).
107.17 Hematological disorders treated by bone marrow or stem cell transplantation (see 107.00F). Consider under a disability for at least 12 consecutive months from the date of transplantation. After that, evaluate any residual impairment(s) under the criteria for the affected body system.
108.00 Skin Disorders
A. What skin disorders do we evaluate with these listings? We use these listings to evaluate skin disorders that may result from hereditary, congenital, or acquired pathological processes. The kinds of impairments covered by these listings are: Ichthyosis, bullous diseases, chronic infections of the skin or mucous membranes, dermatitis, hidradenitis suppurativa, genetic photosensitivity disorders, and burns.
B. What documentation do we need? When we evaluate the existence and severity of your skin disorder, we generally need information about the onset, duration, frequency of flareups, and prognosis of your skin disorder; the location, size, and appearance of lesions; and, when applicable, history of exposure to toxins, allergens, or irritants, familial incidence, seasonal variation, stress factors, and your ability to function outside of a highly protective environment. To confirm the diagnosis, we may need laboratory findings (for example, results of a biopsy obtained independently of Social Security disability evaluation or blood tests) or evidence from other medically acceptable methods consistent with the prevailing state of medical knowledge and clinical practice.
C. How do we assess the severity of your skin disorders(s)? We generally base our assessment of severity on the extent of your skin lesions, the frequency of flareups of your skin lesions, how your symptoms (including pain) limit you, the extent of your treatment, and how your treatment affects you.
1. Extensive skin lesions. Extensive skin lesions are those that involve multiple body sites or critical body areas, and result in a very serious limitation. Examples of extensive skin lesions that result in a very serious limitation include but are not limited to:
a. Skin lesions that interfere with the motion of your joints and that very seriously limit your use of more than one extremity; that is, two upper extremities, two lower extremities, or one upper and one lower extremity.
b. Skin lesions on the palms of both hands that very seriously limit your ability to do fine and gross motor movements.
c. Skin lesions on the soles of both feet, the perineum, or both inguinal areas that very seriously limit your ability to ambulate.
2. Frequency of flareups. If you have skin lesions, but they do not meet the requirements of any of the listings in this body system, you may still have an impairment that results in marked and severe functional limitations when we consider your condition over time, especially if your flareups result in extensive skin lesions, as defined in C1 of this section. Therefore, if you have frequent flareups, we may find that your impairment(s) is medically equal to one of these listings even though you have some periods during which your condition is in remission. We will consider how frequent and serious your flareups are, how quickly they resolve, and how you function between flareups to determine whether you have marked and severe functional limitations that have lasted for a continuous period of at least 12 months or that can be expected to last for a continuous period of at least 12 months. We will also consider the frequency of your flareups when we determine whether you have a severe impairment and when we need to assess functional equivalence.
3. Symptoms (including pain). Symptoms (including pain) may be important factors contributing to the severity of your skin disorder(s). We assess the impact of symptoms as explained in §§ 416.921 and 416.929 of this chapter.
4. Treatment. We assess the effects of medication, therapy, surgery, and any other form of treatment you receive when we determine the severity and duration of your impairment(s). Skin disorders frequently respond to treatment; however, response to treatment can vary widely, with some impairments becoming resistant to treatment. Some treatments can have side effects that can in themselves result in limitations.
a. We assess the effects of continuing treatment as prescribed by determining if there is improvement in the symptoms, signs, and laboratory findings of your disorder, and if you experience side effects that result in functional limitations. To assess the effects of your treatment, we may need information about:
i. The treatment you have been prescribed (for example, the type, dosage, method and frequency of administration of medication or therapy);
ii. Your response to the treatment;
iii. Any adverse effects of the treatment; and
iv. The expected duration of the treatment.
b. Because treatment itself or the effects of treatment may be temporary, in most cases sufficient time must elapse to allow us to evaluate the impact and expected duration of treatment and its side effects. Except under 108.07 and 108.08, you must follow continuing treatment as prescribed for at least 3 months before your impairment can be determined to meet the requirements of a skin disorder listing. (See 108.00H if you are not undergoing treatment or did not have treatment for 3 months.) We consider your specific response to treatment when we evaluate the overall severity of your impairment.
D. How do we assess impairments that may affect the skin and other body systems? When your impairment affects your skin and has effects in other body systems, we first evaluate the predominant feature of your impairment under the appropriate body system. Examples include, but are not limited to the following.
1. Tuberous sclerosis primarily affects the brain. The predominant features are seizures, which we evaluate under the neurological listings in 111.00, and developmental delays or other mental disorders, which we evaluate under the mental disorders listings in 112.00.
2. Malignant tumors of the skin (for example, malignant melanoma) are cancers, or neoplastic diseases, which we evaluate under the listings in 113.00.
3. Autoimmune disorders and other immune system disorders (for example, systemic lupus erythematosus (SLE), scleroderma, human immunodeficiency virus (HIV) infection, and Sjögren's syndrome) often involve more than one body system. We first evaluate these disorders under the immune system disorders listings in 114.00. We evaluate SLE under 114.02, scleroderma under 114.04, Sjögren's syndrome under 114.10, and HIV infection under 114.11.
4. Disfigurement or deformity resulting from skin lesions may result in loss of sight, hearing, speech, and the ability to chew (mastication). We evaluate these impairments and their effects under the special senses and speech listings in 102.00 and the digestive system listings in 105.00. Facial disfigurement or other physical deformities may also have effects we evaluate under the mental disorders listings in 112.00, such as when they affect mood or social functioning.
5. We evaluate erythropoietic porphyrias under the hemic and lymphatic listings in 107.00.
6. We evaluate hemangiomas associated with thrombocytopenia and hemorrhage (for example, Kasabach-Merritt syndrome) involving coagulation defects, under the hemic and lymphatic listings in 107.00. But, when hemangiomas impinge on vital structures or interfere with function, we evaluate their primary effects under the appropriate body system.
E. How do we evaluate genetic photosensitivity disorders?
1. Xeroderma pigmentosum (XP). When you have XP, your impairment meets the requirements of 108.07A if you have clinical and laboratory findings showing that you have the disorder. (See 108.00E3.) People who have XP have a lifelong hypersensitivity to all forms of ultraviolet light and generally lead extremely restricted lives in highly protective environments in order to prevent skin cancers from developing. Some people with XP also experience problems with their eyes, neurological problems, mental disorders, and problems in other body systems.
2. Other genetic photosensitivity disorders. Other genetic photosensitivity disorders may vary in their effects on different people, and may not result in marked and severe functional limitations for a continuous period of at least 12 months. Therefore, if you have a genetic photosensitivity disorder other than XP (established by clinical and laboratory findings as described in 108.00E3), you must show that you have either extensive skin lesions or an inability to function outside of a highly protective environment to meet the requirements of 108.07B. You must also show that your impairment meets the duration requirement. By inability to function outside of a highly protective environment we mean that you must avoid exposure to ultraviolet light (including sunlight passing through windows and light from unshielded fluorescent bulbs), wear protective clothing and eyeglasses, and use opaque broad-spectrum sunscreens in order to avoid skin cancer or other serious effects. Some genetic photosensitivity disorders can have very serious effects in other body systems, especially special senses and speech (102.00), neurological (111.00), mental (112.00), and neoplastic (113.00). We will evaluate the predominant feature of your impairment under the appropriate body system, as explained in 108.00D.
3. Clinical and laboratory findings.
a. General. We need documentation from an acceptable medical source to establish that you have a medically determinable impairment. In general, we must have evidence of appropriate laboratory testing showing that you have XP or another genetic photosensitivity disorder. We will find that you have XP or another genetic photosensitivity disorder based on a report from an acceptable medical source indicating that you have the impairment, supported by definitive genetic laboratory studies documenting appropriate chromosomal changes, including abnormal DNA repair or another DNA or genetic abnormality specific to your type of photosensitivity disorder.
b. What we will accept as medical evidence instead of the actual laboratory report. When we do not have the actual laboratory report, we need evidence from an acceptable medical source that includes appropriate clinical findings for your impairment and that is persuasive that a positive diagnosis has been confirmed by appropriate laboratory testing at some time prior to our evaluation. To be persuasive, the report must state that the appropriate definitive genetic laboratory study was conducted and that the results confirmed the diagnosis. The report must be consistent with other evidence in your case record.
F. How do we evaluate burns? Electrical, chemical, or thermal burns frequently affect other body systems; for example, musculoskeletal, special senses and speech, respiratory, cardiovascular, renal, neurological, or mental. Consequently, we evaluate burns the way we evaluate other disorders that can affect the skin and other body systems, using the listing for the predominant feature of your impairment. For example, if your soft tissue injuries are under continuing surgical management (as defined in 101.00M), we will evaluate your impairment under 101.08. However, if your burns do not meet the requirements of 101.08 and you have extensive skin lesions that result in a very serious limitation (as defined in 108.00C1) that has lasted or can be expected to last for a continuous period of at least 12 months, we will evaluate them under 108.08.
G. How do we determine if your skin disorder(s) will continue at a disabling level of severity in order to meet the duration requirement? For all of these skin disorder listings except 108.07 and 108.08, we will find that your impairment meets the duration requirement if your skin disorder results in extensive skin lesions that persist for at least 3 months despite continuing treatment as prescribed. By persist, we mean that the longitudinal clinical record shows that, with few exceptions, your lesions have been at the level of severity specified in the listing. For 108.07A, we will presume that you meet the duration requirement. For 108.07B and 108.08, we will consider all of the relevant medical and other information in your case record to determine whether your skin disorder meets the duration requirement.
H. How do we assess your skin disorder(s) if your impairment does not meet the requirements of one of these listings?
1. These listings are only examples of common skin disorders that we consider severe enough to result in marked and severe functional limitations. For most of these listings, if you do not have continuing treatment as prescribed, if your treatment has not lasted for at least 3 months, or if you do not have extensive skin lesions that have persisted for at least 3 months, your impairment cannot meet the requirements of these skin disorder listings. (This provision does not apply to 108.07 and 108.08.) However, we may still find that you are disabled because your impairment(s) meets the requirements of a listing in another body system, medically equals (see §§ 404.1526 and 416.926 of this chapter) the severity of a listing, or functionally equals the severity of the listings.
2. If you have not received ongoing treatment or do not have an ongoing relationship with the medical community despite the existence of a severe impairment(s), or if your skin lesions have not persisted for at least 3 months but you are undergoing continuing treatment as prescribed, you may still have an impairment(s) that meets a listing in another body system or that medically equals a listing. If you do not have an impairment(s) that meets or medically equals a listing, we will consider whether your impairment(s) functionally equals the listings. (See § 416.924 of this chapter.) When we decide whether you continue to be disabled, we use the rules in § 416.994a of this chapter.
108.01 Category of Impairments, Skin Disorders
108.02 Ichthyosis, with extensive skin lesions that persist for at least 3 months despite continuing treatment as prescribed.
108.03 Bullous disease (for example, pemphigus, erythema multiforme bullosum, epidermolysis bullosa, bullous pemphigoid, dermatitis herpetiformis), with extensive skin lesions that persist for at least 3 months despite continuing treatment as prescribed.
108.04 Chronic infections of the skin or mucous membranes, with extensive fungating or extensive ulcerating skin lesions that persist for at least 3 months despite continuing treatment as prescribed.
108.05 Dermatitis (for example, psoriasis, dyshidrosis, atopic dermatitis, exfoliative dermatitis, allergic contact dermatitis), with extensive skin lesions that persist for at least 3 months despite continuing treatment as prescribed.
108.06 Hidradenitis suppurativa, with extensive skin lesions involving both axillae, both inguinal areas, or the perineum that persist for at least 3 months despite continuing treatment as prescribed.
108.07 Genetic photosensitivity disorders, established as described in 108.00E.
A. Xeroderma pigmentosum. Consider the individual disabled from birth.
B. Other genetic photosensitivity disorders, with:
1. Extensive skin lesions that have lasted or can be expected to last for a continuous period of at least 12 months, or
2. Inability to function outside of a highly protective environment for a continuous period of at least 12 months (see 108.00E2).
108.08 Burns, with extensive skin lesions that have lasted or can be expected to last for a continuous period of at least 12 months. (See 108.00F).
109.00 Endocrine Disorders
A. What is an endocrine disorder?
An endocrine disorder is a medical condition that causes a hormonal imbalance. When an endocrine gland functions abnormally, producing either too much of a specific hormone (hyperfunction) or too little (hypofunction), the hormonal imbalance can cause various complications in the body. The major glands of the endocrine system are the pituitary, thyroid, parathyroid, adrenal, and pancreas.
B. How do we evaluate the effects of endocrine disorders? The only listing in this body system addresses children from birth to the attainment of age 6 who have diabetes mellitus (DM) and require daily insulin. We evaluate other impairments that result from endocrine disorders under the listings for other body systems. For example:
1. Pituitary gland disorders can disrupt hormone production and normal functioning in other endocrine glands and in many body systems. The effects of pituitary gland disorders vary depending on which hormones are involved. For example, when pituitary growth hormone deficiency in growing children limits bone maturation and results in pathological short stature, we evaluate this linear growth impairment under 100.00. When pituitary hypofunction affects water and electrolyte balance in the kidney and leads to diabetes insipidus, we evaluate the effects of recurrent dehydration under 106.00.
2. Thyroid gland disorders affect the sympathetic nervous system and normal metabolism. We evaluate thyroid-related changes in linear growth under 100.00; thyroid-related changes in blood pressure and heart rate that cause cardiac arrhythmias or other cardiac dysfunction under 104.00; thyroid-related weight loss under 105.00; and cognitive limitations, mood disorders, and anxiety under 112.00.
3. Parathyroid gland disorders affect calcium levels in bone, blood, nerves, muscle, and other body tissues. We evaluate parathyroid-related osteoporosis and fractures under 101.00; abnormally elevated calcium levels in the blood (hypercalcemia) that lead to cataracts under 102.00; kidney failure under 106.00; and recurrent abnormally low blood calcium levels (hypocalcemia) that lead to increased excitability of nerves and muscles, such as tetany and muscle spasms, under 111.00.
4. Adrenal gland disorders affect bone calcium levels, blood pressure, metabolism, and mental status. We evaluate adrenal-related linear growth impairments under 100.00; adrenal-related osteoporosis with fractures that compromises the ability to walk or to use the upper extremities under 101.00; adrenal-related hypertension that worsens heart failure or causes recurrent arrhythmias under 104.00; adrenal-related weight loss under 105.00; and mood disorders under 112.00.
5. Diabetes mellitus and other pancreatic gland disorders disrupt the production of several hormones, including insulin, that regulate metabolism and digestion. Insulin is essential to the absorption of glucose from the bloodstream into body cells for conversion into cellular energy. The most common pancreatic gland disorder is diabetes mellitus (DM). There are two major types of DM: type 1 and type 2. Both type 1 and type 2 DM are chronic disorders that can have serious, disabling complications that meet the duration requirement. Type 1 DM - previously known as “juvenile diabetes” or “insulin-dependent diabetes mellitus” (IDDM) - is an absolute deficiency of insulin secretion that commonly begins in childhood and continues throughout adulthood. Treatment of type 1 DM always requires lifelong daily insulin. With type 2 DM - previously known as “adult-onset diabetes mellitus” or “non-insulin-dependent diabetes mellitus” (NIDDM) - the body's cells resist the effects of insulin, impairing glucose absorption and metabolism. Type 2 is less common than type 1 DM in children, but physicians are increasingly diagnosing type 2 DM before age 18. Treatment of type 2 DM generally requires lifestyle changes, such as increased exercise and dietary modification, and sometimes insulin in addition to other medications. While both type 1 and type 2 DM are usually controlled, some children do not achieve good control for a variety of reasons including, but not limited to, hypoglycemia unawareness, other disorders that can affect blood glucose levels, inability to manage DM due to a mental disorder, or inadequate treatment.
a. Hyperglycemia. Both types of DM cause hyperglycemia, which is an abnormally high level of blood glucose that may produce acute and long-term complications. Acute complications of hyperglycemia include diabetic ketoacidosis. Long-term complications of chronic hyperglycemia include many conditions affecting various body systems but are rare in children.
b. Diabetic ketoacidosis (DKA). DKA is an acute, potentially life-threatening complication of DM in which the chemical balance of the body becomes dangerously hyperglycemic and acidic. It results from a severe insulin deficiency, which can occur due to missed or inadequate daily insulin therapy or in association with an acute illness. It usually requires hospital treatment to correct the acute complications of dehydration, electrolyte imbalance, and insulin deficiency. You may have serious complications resulting from your treatment, which we evaluate under the affected body system. For example, we evaluate cardiac arrhythmias under 104.00, intestinal necrosis under 105.00, and cerebral edema and seizures under 111.00. Recurrent episodes of DKA in adolescents may result from mood or eating disorders, which we evaluate under 112.00.
c. Hypoglycemia. Children with DM may experience episodes of hypoglycemia, which is an abnormally low level of blood glucose. Most children age 6 and older recognize the symptoms of hypoglycemia and reverse them by consuming substances containing glucose; however, some do not take this step because of hypoglycemia unawareness. Severe hypoglycemia can lead to complications, including seizures or loss of consciousness, which we evaluate under 111.00, or altered mental status, cognitive deficits, and permanent brain damage, which we evaluate under 112.00.
C. How do we evaluate DM in children? Listing 109.08 is only for children with DM who have not attained age 6 and who require daily insulin. For all other children (that is, children with DM who are age 6 or older and require daily insulin, and children of any age with DM who do not require daily insulin), we follow our rules for determining whether the DM is severe, alone or in combination with another impairment, whether it meets or medically equals the criteria of a listing in another body system, or functionally equals the listings under the criteria in § 416.926a of this chapter, considering the factors in § 416.924a of this chapter. The management of DM in children can be complex and variable from day to day, and all children with DM require some level of adult supervision. For example, if a child age 6 or older has a medical need for 24-hour-a-day adult supervision of insulin treatment, food intake, and physical activity to ensure survival, we will find that the child's impairment functionally equals the listings based on the example in § 416.926a(m)(2) of this chapter.
D. How do we evaluate other endocrine disorders that do not have effects that meet or medically equal the criteria of any listing in other body systems? If your impairment(s) does not meet or medically equal a listing in another body system, we will consider whether your impairment(s) functionally equals the listings under the criteria in § 416.926a, considering the factors in § 416.924a. When we decide whether you continue to be disabled, we use the rules in § 416.994a.
109.01 Category of Impairments, Endocrine
109.08 Any type of diabetes mellitus in a child who requires daily insulin and has not attained age 6. Consider under a disability until the attainment of age 6. Thereafter, evaluate the diabetes mellitus according to the rules in 109.00B5 and C.
110.00 Congenital Disorders That Affect Multiple Body Systems
A. Which disorders do we evaluate under this body system? We evaluate non-mosaic Down syndrome and catastrophic congenital disorders under this body system.
B. What is non-mosaic Down syndrome? Non-mosaic Down syndrome is a genetic disorder. Most children with non-mosaic Down syndrome have three copies of chromosome 21 in all of their cells (chromosome 21 trisomy); some have an extra copy of chromosome 21 attached to a different chromosome in all of their cells (chromosome 21 translocation). Virtually all children with non-mosaic Down syndrome have characteristic facial or other physical features, delayed physical development, and intellectual disability. Children with non-mosaic Down syndrome may also have congenital heart disease, impaired vision, hearing problems, and other disorders. We evaluate non-mosaic Down syndrome under 110.06. If you have non-mosaic Down syndrome documented as described in 110.00C, we consider you disabled from birth.
C. What evidence do we need to document non-mosaic Down syndrome under 110.06?
1. Under 110.06A, we will find you disabled based on laboratory findings.
a. To find that your disorder meets 110.06A, we need a copy of the laboratory report of karyotype analysis, which is the definitive test to establish non-mosaic Down syndrome. We will not purchase karyotype analysis. We will not accept a fluorescence in situ hybridization (FISH) test because it does not distinguish between the mosaic and non-mosaic forms of Down syndrome.
b. If a physician (see §§ 404.1513(a)(1) and 416.913(a)(1) of this chapter) has not signed the laboratory report of karyotype analysis, the evidence must also include a physician's statement that you have Down syndrome.
c. For purposes of 110.06A, we do not require evidence stating that you have the distinctive facial or other physical features of Down syndrome.
2. If we do not have a laboratory report of karyotype analysis documenting that you have non-mosaic Down syndrome, we may find you disabled under 110.06B or 110.06C.
a. Under 110.06B, we need a physician's report stating: (i) your karyotype diagnosis or evidence that documents your type of Down syndrome that is consistent with prior karyotype analysis (for example, reference to a diagnosis of “trisomy 21”) and (ii) that you have the distinctive facial or other physical features of Down syndrome. We do not require a detailed description of the facial or other physical features of the disorder. However, we will not find that your disorder meets 110.06B if we have evidence - such as evidence of functioning inconsistent with the diagnosis - that indicates that you do not have non-mosaic Down syndrome.
b. If we do not have evidence of prior karyotype analysis (you did not have testing, or you had testing but we do not have information from a physician about the test results), we will find that your disorder meets 110.06C if we have: (i) a physician's report stating that you have the distinctive facial or other physical features of Down syndrome and (ii) evidence that your functioning is consistent with a diagnosis of non-mosaic Down syndrome. This evidence may include medical or nonmedical information about your physical and mental abilities, including information about your development, education, work history, or the results of psychological testing. However, we will not find that your disorder meets 110.06C if we have evidence - such as evidence of functioning inconsistent with the diagnosis - that indicates that you do not have non-mosaic Down syndrome.
D. What are catastrophic congenital disorders? Some catastrophic congenital disorders, such as anencephaly, cyclopia, chromosome 13 trisomy (Patau syndrome or trisomy D), and chromosome 18 trisomy (Edwards' syndrome or trisomy E), are usually expected to result in early death. Others such as cri du chat syndrome (chromosome 5p deletion syndrome) and the infantile onset form of Tay-Sachs disease interfere very seriously with development. We evaluate catastrophic congenital disorders under 110.08. The term “very seriously” in 110.08 has the same meaning as in the term “extreme” in § 416.926a(e)(3) of this chapter.
E. What evidence do we need under 110.08?
We need one of the following to determine if your disorder meets 110.08A or B:
1. A laboratory report of the definitive test that documents your disorder (for example, genetic analysis or evidence of biochemical abnormalities) signed by a physician.
2. A laboratory report of the definitive test that documents your disorder that is not signed by a physician and a report from a physician stating that you have the disorder.
3. A report from a physician stating that you have the disorder with the typical clinical features of the disorder and that you had definitive testing that documented your disorder. In this case, we will find that your disorder meets 110.08A or B unless we have evidence that indicates that you do not have the disorder.
4. If we do not have the definitive laboratory evidence we need under E1, E2, or E3, we will find that your disorder meets 110.08A or B if we have: (i) a report from a physician stating that you have the disorder and that you have the typical clinical features of the disorder, and (ii) other evidence that supports the diagnosis. This evidence may include medical or nonmedical information about your development and functioning.
5. For obvious catastrophic congenital anomalies that are expected to result in early death, such as anencephaly and cyclopia, we need evidence from a physician that demonstrates that the infant has the characteristic physical features of the disorder. In these rare cases, we do not need laboratory testing or any other evidence that confirms the disorder.
F. How do we evaluate mosaic Down syndrome and other congenital disorders that affect multiple body systems?
1. Mosaic Down syndrome. Approximately 2 percent of children with Down syndrome have the mosaic form. In mosaic Down syndrome, there are some cells with an extra copy of chromosome 21 and other cells with the normal two copies of chromosome 21. Mosaic Down syndrome can be so slight as to be undetected clinically, but it can also be profound and disabling, affecting various body systems.
2. Other congenital disorders that affect multiple body systems. Other congenital disorders, such as congenital anomalies, chromosomal disorders, dysmorphic syndromes, inborn metabolic syndromes, and perinatal infectious diseases, can cause deviation from, or interruption of, the normal function of the body or can interfere with development. Examples of these disorders include both the juvenile and late-onset forms of Tay-Sachs disease, trisomy X syndrome (XXX syndrome), fragile X syndrome, phenylketonuria (PKU), caudal regression syndrome, and fetal alcohol syndrome. For these disorders and other disorders like them, the degree of deviation, interruption, or interference, as well as the resulting functional limitations and their progression, may vary widely from child to child and may affect different body systems.
3. Evaluating the effects of mosaic Down syndrome or another congenital disorder under the listings. When the effects of mosaic Down syndrome or another congenital disorder that affects multiple body systems are sufficiently severe we evaluate the disorder under the appropriate affected body system(s), such as musculoskeletal, special senses and speech, neurological, or mental disorders. Otherwise, we evaluate the specific functional limitations that result from the disorder under our other rules described in 110.00G.
G. What if your disorder does not meet a listing? If you have a severe medically determinable impairment(s) that does not meet a listing, we will consider whether your impairment(s) medically equals a listing. See § 416.926 of this chapter. If your impairment(s) does not meet or medically equal a listing, we will consider whether it functionally equals the listings. See §§ 416.924a and 416.926a of this chapter. We use the rules in § 416.994a of this chapter when we decide whether you continue to be disabled.
110.01 Category of Impairments, Congenital Disorders That Affect Multiple Body Systems
110.06 Non-mosaic Down syndrome (chromosome 21 trisomy or chromosome 21 translocation), documented by:
A. A laboratory report of karyotype analysis signed by a physician, or both a laboratory report of karyotype analysis not signed by a physician and a statement by a physician that the child has Down syndrome (see 110.00C1), or
B. A physician's report stating that the child has chromosome 21 trisomy or chromosome 21 translocation consistent with karyotype analysis with the distinctive facial or other physical features of Down syndrome (see 110.00C2a), or
C. A physician's report stating that the child has Down syndrome with the distinctive facial or other physical features and evidence demonstrating that the child is functioning at the level of a child with non-mosaic Down syndrome (see 110.00C2b).
110.08 A catastrophic congenital disorder (see 110.00D and 110.00E) with:
A. Death usually expected within the first months of life, or
B. Very serious interference with development or functioning.
111.00 Neurological Disorders
A. Which neurological disorders do we evaluate under these listings? We evaluate epilepsy, coma or persistent vegetative state (PVS), and neurological disorders that cause disorganization of motor function, bulbar and neuromuscular dysfunction, or communication impairment. Under this body system, we evaluate the limitations resulting from the impact of the neurological disease process itself. If you have a neurological disorder(s) that affects your physical and mental functioning, we will evaluate your impairments under the rules we use to determine functional equivalence. If your neurological disorder results in only mental impairment or if you have a co-occurring mental condition that is not caused by your neurological disorder (for example, Autism spectrum disorder), we will evaluate your mental impairment under the mental disorders body system, 112.00.
B. What evidence do we need to document your neurological disorder?
1. We need both medical and non-medical evidence (signs, symptoms, and laboratory findings) to assess the effects of your neurological disorder. Medical evidence should include your medical history, examination findings, relevant laboratory tests, and the results of imaging. Imaging refers to medical imaging techniques, such as x-ray, computerized tomography (CT), magnetic resonance imaging (MRI), and electroencephalography (EEG). The imaging must be consistent with the prevailing state of medical knowledge and clinical practice as the proper technique to support the evaluation of the disorder. In addition, the medical evidence may include descriptions of any prescribed treatment and your response to it. We consider non-medical evidence such as statements you or others make about your impairments, your restrictions, your daily activities, or, if you are an adolescent, your efforts to work.
2. We will make every reasonable effort to obtain the results of your laboratory and imaging evidence. When the results of any of these tests are part of the existing evidence in your case record, we will evaluate the test results and all other relevant evidence. We will not purchase imaging, or other diagnostic tests or laboratory tests that are complex, may involve significant risk, or that are invasive. We will not routinely purchase tests that are expensive or not readily available.
C. How do we consider adherence to prescribed treatment in neurological disorders? In 111.02 (Epilepsy) and 111.12 (Myasthenia gravis), we require that limitations from these neurological disorders exist despite adherence to prescribed treatment. “Despite adherence to prescribed treatment” means that you have taken medication(s) or followed other treatment procedures for your neurological disorder(s) as prescribed by a physician for three consecutive months but your impairment continues to meet the other listing requirements despite this treatment. You may receive your treatment at a health care facility that you visit regularly, even if you do not see the same physician on each visit.
D. What do we mean by disorganization of motor function?
1. Disorganization of motor function means interference, due to your neurological disorder, with movement of two extremities; i.e., the lower extremities, or upper extremities (including fingers, wrists, hands, arms, and shoulders). By two extremities we mean both lower extremities, or both upper extremities, or one upper extremity and one lower extremity. All listings in this body system, except for 111.02 (Epilepsy) and 111.20 (Coma and persistent vegetative state), include criteria for disorganization of motor function that results in an extreme limitation in your ability to:
a. Stand up from a seated position; or
b. Balance while standing or walking; or
c. Use the upper extremities (e.g., fingers, wrists, hands, arms, and shoulders).
2. Extreme limitation means the inability to stand up from a seated position, maintain balance in a standing position and while walking, or use your upper extremities to independently initiate, sustain, and complete age-appropriate activities. The assessment of motor function depends on the degree of interference with standing up; balancing while standing or walking; or using the upper extremities (including fingers, hands, arms, and shoulders).
a. Inability to stand up from a seated position means that once seated you are unable to stand and maintain an upright position without the assistance of another person or the use of an assistive device, such as a walker, two crutches, or two canes.
b. Inability to maintain balance in a standing position means that you are unable to maintain an upright position while standing or walking without the assistance of another person or an assistive device, such as a walker, two crutches, or two canes.
c. Inability to use your upper extremities means that you have a loss of function of both upper extremities (e.g., fingers, wrists, hands, arms, and shoulders) that very seriously limits your ability to independently initiate, sustain, and complete age- appropriate activities involving fine and gross motor movements. Inability to perform fine and gross motor movements could include not being able to pinch, manipulate, and use your fingers; or not being able to use your hands, arms, and shoulders to perform gross motor movements, such as handling, gripping, grasping, holding, turning, and reaching; or not being able to engage in exertional movements such a lifting, carrying, pushing, and pulling.
3. For children who are not yet able to balance, stand up, or walk independently, we consider their function based on assessments of limitations in the ability to perform comparable age-appropriate activities with the lower and upper extremities, given normal developmental milestones. For such children, an extreme level of limitation means developmental milestones at less than one-half of the child's chronological age.
E. What do we mean by bulbar and neuromuscular dysfunction? The bulbar region of the brain is responsible for controlling the bulbar muscles in the throat, tongue, jaw, and face. Bulbar and neuromuscular dysfunction refers to weakness in these muscles, resulting in breathing, swallowing, and speaking impairments. Listings 111.12 (Myasthenia gravis) and 111.22 (Motor neuron disorders) include criteria for evaluating bulbar and neuromuscular dysfunction. If your neurological disorder has resulted in a breathing disorder, we may evaluate that condition under the respiratory system, 103.00.
F. What is epilepsy, and how do we evaluate it under 111.02?
1. Epilepsy is a pattern of recurrent and unprovoked seizures that are manifestations of abnormal electrical activity in the brain. There are various types of generalized and “focal” or partial seizures. In children, the most common potentially disabling seizure types are generalized tonic-clonic seizures, dyscognitive seizures (formerly complex partial seizures), and absence seizures. However, psychogenic nonepileptic seizures and pseudoseizures are not epileptic seizures for the purpose of 111.02. We evaluate psychogenic seizures and pseudoseizures under the mental disorders body system, 112.00.
a. Generalized tonic-clonic seizures are characterized by loss of consciousness accompanied by a tonic phase (sudden muscle tensing causing the child to lose postural control) followed by a clonic phase (rapid cycles of muscle contraction and relaxation, also called convulsions). Tongue biting and incontinence may occur during generalized tonic-clonic seizures, and injuries may result from falling.
b. Dyscognitive seizures are characterized by alteration of consciousness without convulsions or loss of muscle control. During the seizure, blank staring, change of facial expression, and automatisms (such as lip smacking, chewing or swallowing, or repetitive simple actions, such as gestures or verbal utterances) may occur. During its course, a dyscognitive seizure may progress into a generalized tonic-clonic seizure (see 111.00F1a).
c. Absence seizures (petit mal) are also characterized by an alteration in consciousness, but are shorter than other generalized seizures (e.g., tonic-clonic and dyscognitive) seizures, generally lasting for only a few seconds rather than minutes. They may present with blank staring, change of facial expression, lack of awareness and responsiveness, and a sense of lost time after the seizure. An aura never precedes absence seizures. Although absence seizures are brief, frequent occurrence may limit functioning. This type of seizure usually does not occur after adolescence.
d. Febrile seizures may occur in young children in association with febrile illnesses. We will consider seizures occurring during febrile illnesses. To meet 111.02, we require documentation of seizures during nonfebrile periods and epilepsy must be established.
2. Description of seizure. We require at least one detailed description of your seizures from someone, preferably a medical professional, who has observed at least one of your typical seizures. If you experience more than one type of seizure, we require a description of each type.
3. Serum drug levels. We do not require serum drug levels; therefore, we will not purchase them. However, if serum drug levels are available in your medical records, we will evaluate them in the context of the other evidence in your case record.
4. Counting seizures. The period specified in 111.02A or B cannot begin earlier than one month after you began prescribed treatment. The required number of seizures must occur within the period we are considering in connection with your application or continuing disability review. When we evaluate the frequency of your seizures, we also consider your adherence to prescribed treatment (see 111.00C). When we determine the number of seizures you have had in the specified period, we will:
a. Count multiple seizures occurring in a 24-hour period as one seizure.
b. Count status epilepticus (a continuous series of seizures without return to consciousness between seizures) as one seizure.
c. Count a dyscognitive seizure that progresses into a generalized tonic-clonic seizure as one generalized tonic-clonic seizure.
d. We do not count seizures that occur during a period when you are not adhering to prescribed treatment without good reason. When we determine that you had a good reason for not adhering to prescribed treatment, we will consider your physical, mental, educational, and communicative limitations (including any language barriers). We will consider you to have good reason for not following prescribed treatment if, for example, the treatment is very risky for you due to its consequences or unusual nature, or if you are unable to afford prescribed treatment that you are willing to accept, but for which no free community resources are available. We will follow guidelines found in our policy, such as § 416.930(c) of this chapter, when we determine whether you have a good reason for not adhering to prescribed treatment.
e. We do not count psychogenic nonepileptic seizures or pseudoseizures under 111.02.We evaluate these seizures under the mental disorders body system, 112.00.
5. Electroencephalography (EEG) testing. We do not require EEG test results; therefore, we will not purchase them. However, if EEG test results are available in your medical records, we will evaluate them in the context of the other evidence in your case record.
G. What is vascular insult to the brain, and how do we evaluate it under 111.04?
1. Vascular insult to the brain (cerebrum, cerebellum, or brainstem), commonly referred to as stroke or cerebrovascular accident (CVA), is brain cell death caused by an interruption of blood flow within or leading to the brain, or by a hemorrhage from a ruptured blood vessel or aneurysm in the brain. If you have a vision impairment resulting from your vascular insult, we may evaluate that impairment under the special senses body system, 102.00.
2. We generally need evidence from at least 3 months after the vascular insult to determine whether you have disorganization of motor function under 111.04. In some cases, evidence of your vascular insult is sufficient to allow your claim within 3 months post-vascular insult. If we are unable to allow your claim within 3 months after your vascular insult, we will defer adjudication of the claim until we obtain evidence of your neurological disorder at least 3 months post-vascular insult.
H. What are benign brain tumors, and how do we evaluate them under 111.05? Benign brain tumors are noncancerous (nonmalignant) abnormal growths of tissue in or on the brain that invade healthy brain tissue or apply pressure on the brain or cranial nerves. We evaluate their effects on your functioning as discussed in 111.00D. We evaluate malignant brain tumors under the cancer body system in 113.00. If you have a vision impairment resulting from your benign brain tumor, we may evaluate that impairment under the special senses body system, 102.00.
I. What is cerebral palsy, and how do we evaluate it under 111.07?
1. Cerebral palsy (CP) is a term that describes a group of static, nonprogressive disorders caused by abnormalities within the brain that disrupt the brain's ability to control movement, muscle coordination, and posture. The resulting motor deficits manifest very early in a child's development, with delayed or abnormal progress in attaining developmental milestones; deficits may become more obvious as the child grows and matures over time.
2. We evaluate your signs and symptoms, such as ataxia, spasticity, flaccidity, athetosis, chorea, and difficulty with precise movements when we determine your ability to stand up, balance, walk, or perform fine and gross motor movements. We will also evaluate your signs, such as dysarthria and apraxia of speech, and receptive and expressive language problems when we determine your ability to communicate.
3. We will consider your other impairments or signs and symptoms that develop secondary to the disorder, such as post-impairment syndrome (a combination of pain, fatigue, and weakness due to muscle abnormalities); overuse syndromes (repetitive motion injuries); arthritis; abnormalities of proprioception (perception of the movements and position of the body); abnormalities of stereognosis (perception and identification of objects by touch); learning problems; anxiety; and depression.
J. What are spinal cord disorders, and how do we evaluate them under 111.08?
1. Spinal cord disorders may be congenital or caused by injury to the spinal cord. Motor signs and symptoms of spinal cord disorders include paralysis, flaccidity, spasticity, and weakness.
2. Spinal cord disorders with complete loss of function (111.08A) addresses spinal cord disorders that result in complete lack of motor, sensory, and autonomic function of the affected part(s) of the body.
3. Spinal cord disorders with disorganization of motor function (111.08B) addresses spinal cord disorders that result in less than complete loss of function of the affected part(s) of the body, reducing, but not eliminating, motor, sensory, and autonomic function.
4. When we evaluate your spinal cord disorder, we generally need evidence from at least 3 months after your symptoms began in order to evaluate your disorganization of motor function. In some cases, evidence of your spinal cord disorder may be sufficient to allow your claim within 3 months after the spinal cord disorder. If the medical evidence demonstrates total cord transection causing a loss of motor and sensory functions below the level of injury, we will not wait 3 months but will make the allowance decision immediately.
K. What are communication impairments associated with neurological disorders, and how do we evaluate them under 111.09?
1. Communication impairments result from medically determinable neurological disorders that cause dysfunction in the parts of the brain responsible for speech and language. Under 111.09, we must have recent comprehensive evaluation including all areas of affective and effective communication, performed by a qualified professional, to document a communication impairment associated with a neurological disorder.
2. Under 111.09A, we need documentation from a qualified professional that your neurological disorder has resulted in a speech deficit that significantly affects your ability to communicate. Significantly affects means that you demonstrate a serious limitation in communicating, and a person who is unfamiliar with you cannot easily understand or interpret your speech.
3. Under 111.09B, we need documentation from a qualified professional that shows that your neurological disorder has resulted in a comprehension deficit that results in ineffective verbal communication for your age. For the purposes of 111.09B, comprehension deficit means a deficit in receptive language. Ineffective verbal communication means that you demonstrate serious limitation in your ability to communicate orally on the same level as other children of the same age and level of development.
4. Under 111.09C, we need documentation of a neurological disorder that has resulted in hearing loss. Your hearing loss will be evaluated under listing 102.10 or 102.11.
5. We evaluate speech deficits due to non-neurological disorders under 2.09.
L. What are neurodegenerative disorders of the central nervous system, such as Juvenile-onset Huntington's disease and Friedreich's ataxia, and how do we evaluate them under 111.17? Neurodegenerative disorders of the central nervous system are disorders characterized by progressive and irreversible degeneration of neurons or their supporting cells. Over time, these disorders impair many of the body's motor or cognitive and other mental functions. We consider neurodegenerative disorders of the central nervous system under 111.17 that we do not evaluate elsewhere in section 111.00, such as juvenile-onset Huntington's disease (HD) and Friedreich's ataxia. When these disorders result in solely cognitive and other mental functional limitations, we will evaluate the disorder under the mental disorder listings, 112.00.
M. What is traumatic brain injury, and how do we evaluate it under 111.18?
1. Traumatic brain injury (TBI) is damage to the brain resulting from skull fracture, collision with an external force leading to a closed head injury, or penetration by an object that enters the skull and makes contact with brain tissue. We evaluate a TBI that results in coma or persistent vegetative state (PVS) under 111.20.
2. We generally need evidence from at least 3 months after the TBI to evaluate whether you have disorganization of motor function under 111.18. In some cases, evidence of your TBI is sufficient to determine disability. If we are unable to allow your claim within 3 months post-TBI, we will defer adjudication of the claim until we obtain evidence of your neurological disorder at least 3 months post-TBI. If a finding of disability still is not possible at that time, we will again defer adjudication of the claim until we obtain evidence at least 6 months after your TBI.
N. What are coma and persistent vegetative state, and how do we evaluate them under 111.20? Coma is a state of unconsciousness in which a child does not exhibit a sleep/wake cycle, and is unable to perceive or respond to external stimuli. Children who do not fully emerge from coma may progress into persistent vegetative state (PVS). PVS is a condition of partial arousal in which a child may have a low level of consciousness but is still unable to react to external stimuli. In contrast to coma, a child in a PVS retains sleep/wake cycles and may exhibit some key lower brain functions, such as spontaneous movement, opening and moving eyes, and grimacing. Coma or PVS may result from a TBI, a nontraumatic insult to the brain (such as a vascular insult, infection, or brain tumor), or a neurodegenerative or metabolic disorder. Medically induced comas should be considered under the section pertaining to the underlying reason the coma was medically induced and not under this section.
O. What is multiple sclerosis, and how do we evaluate it under 111.21?
1. Multiple sclerosis (MS) is a chronic, inflammatory, degenerative disorder that damages the myelin sheath surrounding the nerve fibers in the brain and spinal cord. The damage disrupts the normal transmission of nerve impulses within the brain and between the brain and other parts of the body causing impairment in muscle coordination, strength, balance, sensation, and vision. There are several forms of MS, ranging from slightly to highly aggressive. Milder forms generally involve acute attacks (exacerbations) with partial or complete recovery from signs and symptoms (remissions). Aggressive forms generally exhibit a steady progression of signs and symptoms with few or no remissions. The effects of all forms vary from child to child.
2. We evaluate your signs and symptoms, such as flaccidity, spasticity, spasms, incoordination, imbalance, tremor, physical fatigue, muscle weakness, dizziness, tingling, and numbness when we determine your ability to stand up, balance, walk, or perform fine and gross motor movements, such as using your arms, hands, and fingers. If you have a vision impairment resulting from your MS, we may evaluate that impairment under the special senses body system, 102.00.
P. What are motor neuron disorders, and how do we evaluate them under 111.22? Motor neuron disorders are progressive neurological disorders that destroy the cells that control voluntary muscle activity, such as walking, breathing, swallowing, and speaking. The most common motor neuron disorders in children are progressive bulbar palsy and spinal muscular dystrophy syndromes. We evaluate the effects of these disorders on motor functioning or bulbar and neuromuscular functioning.
Q. How do we consider symptoms of fatigue in these listings? Fatigue is one of the most common and limiting symptoms of some neurological disorders, such as multiple sclerosis and myasthenia gravis. These disorders may result in physical fatigue (lack of muscle strength) or mental fatigue (decreased awareness or attention). When we evaluate your fatigue, we will consider the intensity, persistence, and effects of fatigue on your functioning. This may include information such as the clinical and laboratory data and other objective evidence concerning your neurological deficit, a description of fatigue considered characteristic of your disorder, and information about your functioning. We consider the effects of physical fatigue on your ability to stand up, balance, walk, or perform fine and gross motor movements using the criteria described in 111.00D.
R. How do we evaluate your neurological disorder when it does not meet one of these listings?
1. If your neurological disorder does not meet the criteria of any of these listings, we must also consider whether your impairment(s) meets the criteria of a listing in another body system. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. See § 416.926 of this chapter.
2. If your impairment(s) does not meet or medically equal a listing, we will consider whether your impairment(s) functionally equals the listings. See § 416.926a of this chapter.
3. We use the rules in § 416.994a of this chapter when we decide whether you continue to be disabled.
111.01 Category of Impairments, Neurological Disorders
111.02 Epilepsy, documented by a detailed description of a typical seizure and characterized by A or B:
A. Generalized tonic-clonic seizures (see 111.00F1a), occurring at least once a month for at least 3 consecutive months (see 111.00F4) despite adherence to prescribed treatment (see 111.00C); or
B. Dyscognitive seizures (see 111.00F1b) or absence seizures (see 111.00F1c), occurring at least once a week for at least 3 consecutive months (see 111.00F4) despite adherence to prescribed treatment (see 111.00C).
111.03 [Reserved]
111.04 Vascular insult to the brain, characterized by disorganization of motor function in two extremities (see 111.00D1), resulting in an extreme limitation (see 111.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities, persisting for at least 3 consecutive months after the insult.
111.05 Benign brain tumors, characterized by disorganization of motor function in two extremities (see 111.00D1), resulting in an extreme limitation (see 111.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities.
111.06 [Reserved]
111.07 Cerebral palsy, characterized by disorganization of motor function in two extremities (see 111.00D1), resulting in an extreme limitation (see 111.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities.
111.08 Spinal cord disorders, characterized by A or B:
A. Complete loss of function, as described in 111.00J2, persisting for 3 consecutive months after the disorder (see 111.00J4); or
B. Disorganization of motor function in two extremities (see 111.00D1), resulting in an extreme limitation (see 111.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities persisting for 3 consecutive months after the disorder (see 111.00J4).
111.09 Communication impairment, associated with documented neurological disorder and one of the following:
A. Documented speech deficit that significantly affects (see 111.00K1) the clarity and content of the speech; or
B. Documented comprehension deficit resulting in ineffective verbal communication (see 111.00K2) for age; or
C. Impairment of hearing as described under the criteria in 102.10 or 102.11.
111.10 [Reserved]
111.11 [Reserved]
111.12 Myasthenia gravis, characterized by A or B despite adherence to prescribed treatment for at least 3 months (see 111.00C):
A. Disorganization of motor function in two extremities (see 111.00D1), resulting in an extreme limitation (see 111.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities; or
B. Bulbar and neuromuscular dysfunction (see 111.00E), resulting in:
1. One myasthenic crisis requiring mechanical ventilation; or
2. Need for supplemental enteral nutrition via a gastrostomy or parenteral nutrition via a central venous catheter.
111.13 Muscular dystrophy, characterized by disorganization of motor function in two extremities (see 111.00D1), resulting in an extreme limitation (see 111.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities.
111.14 Peripheral neuropathy, characterized by disorganization of motor function in two extremities (see 111.00D1), resulting in an extreme limitation (see 111.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities.
111.15 [Reserved]
111.16 [Reserved]
111.17 Neurodegenerative disorders of the central nervous system, such as Juvenile-onset Huntington's disease and Friedreich's ataxia, characterized by disorganization of motor function in two extremities (see 111.00D1), resulting in an extreme limitation (see 111.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities.
111.18 Traumatic brain injury, characterized by disorganization of motor function in two extremities (see 111.00D1), resulting in an extreme limitation (see 111.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities, persisting for at least 3 consecutive months after the injury.
111.19 [Reserved]
111.20 Coma or persistent vegetative state, persisting for at least 1 month.
111.21 Multiple sclerosis, characterized by disorganization of motor function in two extremities (see 111.00D1), resulting in an extreme limitation (see 111.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities.
111.22 Motor neuron disorders, characterized by A or B:
A. Disorganization of motor function in two extremities (see 111.00D1), resulting in an extreme limitation (see 111.00D2) in the ability to stand up from a seated position, balance while standing or walking, or use the upper extremities; or
B. Bulbar and neuromuscular dysfunction (see 111.00E), resulting in:
1. Acute respiratory failure requiring invasive mechanical ventilation; or
2. Need for supplemental enteral nutrition via a gastrostomy or parenteral nutrition via a central venous catheter.
112.00 Mental Disorders
A. How are the listings for mental disorders for children arranged, and what do they require?
1. The listings for mental disorders for children are arranged in 12 categories: neurocognitive disorders (112.02); schizophrenia spectrum and other psychotic disorders (112.03); depressive, bipolar and related disorders (112.04); intellectual disorder (112.05); anxiety and obsessive-compulsive disorders (112.06); somatic symptom and related disorders (112.07); personality and impulse-control disorders (112.08); autism spectrum disorder (112.10); neurodevelopmental disorders (112.11); eating disorders (112.13); developmental disorders in infants and toddlers (112.14); and trauma- and stressor-related disorders (112.15). All of these listings, with the exception of 112.14, apply to children from age three to attainment of age 18. Listing 112.14 is for children from birth to attainment of age 3.
2. Listings 112.07, 112.08, 112.10, 112.11, 112.13, and 112.14 have two paragraphs, designated A and B; your mental disorder must satisfy the requirements of both paragraphs A and B. Listings 112.02, 112.03, 112.04, 112.06, and 112.15 have three paragraphs, designated A, B, and C; your mental disorder must satisfy the requirements of both paragraphs A and B, or the requirements of both paragraphs A and C. Listing 112.05 has two paragraphs that are unique to that listing (see 112.00A3); your mental disorder must satisfy the requirements of either paragraph A or paragraph B.
a. Paragraph A of each listing (except 112.05) includes the medical criteria that must be present in your medical evidence.
b. Paragraph B of each listing (except 112.05) provides the functional criteria we assess to evaluate how your mental disorder limits your functioning. For children ages 3 to 18, these criteria represent the areas of mental functioning a child uses to perform age-appropriate activities. They are: understand, remember, or apply information; interact with others; concentrate, persist, or maintain pace; and adapt or manage oneself. (See 112.00I for a discussion of the criteria for children from birth to attainment of age 3 under 112.14.) We will determine the degree to which your medically determinable mental impairment affects the four areas of mental functioning and your ability to function age-appropriately in a manner comparable to that of other children your age who do not have impairments. (Hereinafter, the words “age-appropriately” incorporate the qualifying statement, “in a manner comparable to that of other children your age who do not have impairments.”) To satisfy the paragraph B criteria, your mental disorder must result in “extreme” limitation of one, or “marked” limitation of two, of the four areas of mental functioning. (When we refer to “paragraph B criteria” or “area[s] of mental functioning” in the introductory text of this body system, we mean the criteria in paragraph B of every listing except 112.05 and 112.14.)
c. Paragraph C of listings 112.02, 112.03, 112.04, 112.06, and 112.15 provides the criteria we use to evaluate “serious and persistent mental disorders.” To satisfy the paragraph C criteria, your mental disorder must be “serious and persistent”; that is, there must be a medically documented history of the existence of the disorder over a period of at least 2 years, and evidence that satisfies the criteria in both C1 and C2 (see 112.00G). (When we refer to “paragraph C” or “the paragraph C criteria” in the introductory text of this body system, we mean the criteria in paragraph C of listings 112.02, 112.03, 112.04, 112.06, and 112.15.)
3. Listing 112.05 has two paragraphs, designated A and B, that apply to only intellectual disorder. Each paragraph requires that you have significantly subaverage general intellectual functioning and significant deficits in current adaptive functioning.
B. Which mental disorders do we evaluate under each listing category for children?
1. Neurocognitive disorders (112.02).
a. These disorders are characterized in children by a clinically significant deviation in normal cognitive development or by a decline in cognitive functioning. Symptoms and signs may include, but are not limited to, disturbances in memory, executive functioning (that is, higher-level cognitive processes; for example, regulating attention, planning, inhibiting responses, decision-making), visual-spatial functioning, language and speech, perception, insight, and judgment.
b. Examples of disorders that we evaluate in this category include major neurocognitive disorder; mental impairments resulting from medical conditions such as a metabolic disease (for example, juvenile Tay-Sachs disease), human immunodeficiency virus infection, vascular malformation, progressive brain tumor, or traumatic brain injury; or substance-induced cognitive disorder associated with drugs of abuse, medications, or toxins. (We evaluate neurological disorders under that body system (see 111.00). We evaluate cognitive impairments that result from neurological disorders under 112.02 if they do not satisfy the requirements in 111.00. We evaluate catastrophic genetic disorders under listings in 110.00, 111.00, or 112.00, as appropriate. We evaluate genetic disorders that are not catastrophic under the affected body system(s).)
c. This category does not include the mental disorders that we evaluate under intellectual disorder (112.05), autism spectrum disorder (112.10), and neurodevelopmental disorders (112.11).
2. Schizophrenia spectrum and other psychotic disorders (112.03).
a. These disorders are characterized by delusions, hallucinations, disorganized speech, or grossly disorganized or catatonic behavior, causing a clinically significant decline in functioning. Symptoms and signs may include, but are not limited to, inability to initiate and persist in goal-directed activities, social withdrawal, flat or inappropriate affect, poverty of thought and speech, loss of interest or pleasure, disturbances of mood, odd beliefs and mannerisms, and paranoia.
b. Examples of disorders that we evaluate in this category include schizophrenia, schizoaffective disorder, delusional disorder, and psychotic disorder due to another medical condition.
3. Depressive, bipolar and related disorders (112.04).
a. These disorders are characterized by an irritable, depressed, elevated, or expansive mood, or by a loss of interest or pleasure in all or almost all activities, causing a clinically significant decline in functioning. Symptoms and signs may include, but are not limited to, feelings of hopelessness or guilt, suicidal ideation, a clinically significant change in body weight or appetite, sleep disturbances, an increase or decrease in energy, psychomotor abnormalities, disturbed concentration, pressured speech, grandiosity, reduced impulse control, sadness, euphoria, and social withdrawal. Depending on a child's age and developmental stage, certain features, such as somatic complaints, irritability, anger, aggression, and social withdrawal may be more commonly present than other features.
b. Examples of disorders that we evaluate in this category include bipolar disorders (I or II), cyclothymic disorder, disruptive mood dysregulation disorder, major depressive disorder, persistent depressive disorder (dysthymia), and bipolar or depressive disorder due to another medical condition.
4. Intellectual disorder (112.05).
a. This disorder is characterized by significantly subaverage general intellectual functioning and significant deficits in current adaptive functioning. Signs may include, but are not limited to, poor conceptual, social, or practical skills evident in your adaptive functioning.
b. The disorder that we evaluate in this category may be described in the evidence as intellectual disability, intellectual developmental disorder, or historically used terms such as “mental retardation.”
c. This category does not include the mental disorders that we evaluate under neurocognitive disorders (112.02), autism spectrum disorder (112.10), or neurodevelopmental disorders (112.11).
5. Anxiety and obsessive-compulsive disorders (112.06).
a. These disorders are characterized by excessive anxiety, worry, apprehension, and fear, or by avoidance of feelings, thoughts, activities, objects, places, or people. Symptoms and signs may include, but are not limited to, restlessness, difficulty concentrating, hyper-vigilance, muscle tension, sleep disturbance, fatigue, panic attacks, obsessions and compulsions, constant thoughts and fears about safety, and frequent physical complaints. Depending on a child's age and developmental stage, other features may also include refusal to go to school, academic failure, frequent stomachaches and other physical complaints, extreme worries about sleeping away from home, being overly clinging, and exhibiting tantrums at times of separation from caregivers.
b. Examples of disorders that we evaluate in this category include separation anxiety disorder, social anxiety disorder, panic disorder, generalized anxiety disorder, agoraphobia, and obsessive-compulsive disorder.
c. This category does not include the mental disorders that we evaluate under trauma- and stressor-related disorders (112.15).
6. Somatic symptom and related disorders (112.07).
a. These disorders are characterized by physical symptoms or deficits that are not intentionally produced or feigned, and that, following clinical investigation, cannot be fully explained by a general medical condition, another mental disorder, the direct effects of a substance, or a culturally sanctioned behavior or experience. Symptoms and signs may include, but are not limited to, pain and other abnormalities of sensation, gastrointestinal symptoms, fatigue, abnormal motor movement, pseudoseizures, and pseudoneurological symptoms, such as blindness or deafness.
b. Examples of disorders that we evaluate in this category include somatic symptom disorder and conversion disorder.
7. Personality and impulse-control disorders (112.08).
a. These disorders are characterized by enduring, inflexible, maladaptive, and pervasive patterns of behavior. Onset may occur in childhood but more typically occurs in adolescence or young adulthood. Symptoms and signs may include, but are not limited to, patterns of distrust, suspiciousness, and odd beliefs; social detachment, discomfort, or avoidance; hypersensitivity to negative evaluation; an excessive need to be taken care of; difficulty making independent decisions; a preoccupation with orderliness, perfectionism, and control; and inappropriate, intense, impulsive anger and behavioral expression grossly out of proportion to any external provocation or psychosocial stressors.
b. Examples of disorders that we evaluate in this category include paranoid, schizoid, schizotypal, borderline, avoidant, dependent, obsessive-compulsive personality disorders, and intermittent explosive disorder.
8. Autism spectrum disorder (112.10).
a. These disorders are characterized by qualitative deficits in the development of reciprocal social interaction, verbal and nonverbal communication skills, and symbolic or imaginative play; restricted repetitive and stereotyped patterns of behavior, interests, and activities; and stagnation of development or loss of acquired skills. Symptoms and signs may include, but are not limited to, abnormalities and unevenness in the development of cognitive skills; unusual responses to sensory stimuli; and behavioral difficulties, including hyperactivity, short attention span, impulsivity, aggressiveness, or self-injurious actions.
b. Examples of disorders that we evaluate in this category include autism spectrum disorder with or without accompanying intellectual impairment, and autism spectrum disorder with or without accompanying language impairment.
c. This category does not include the mental disorders that we evaluate under neurocognitive disorders (112.02), intellectual disorder (112.05), and neurodevelopmental disorders (112.11).
9. Neurodevelopmental disorders (112.11).
a. These disorders are characterized by onset during the developmental period, that is, during childhood or adolescence, although sometimes they are not diagnosed until adulthood. Symptoms and signs may include, but are not limited to, underlying abnormalities in cognitive processing (for example, deficits in learning and applying verbal or nonverbal information, visual perception, memory, or a combination of these); deficits in attention or impulse control; low frustration tolerance; excessive or poorly planned motor activity; difficulty with organizing (time, space, materials, or tasks); repeated accidental injury; and deficits in social skills. Symptoms and signs specific to tic disorders include sudden, rapid, recurrent, non-rhythmic, motor movement or vocalization.
b. Examples of disorders that we evaluate in this category include specific learning disorder, borderline intellectual functioning, and tic disorders (such as Tourette syndrome).
c. This category does not include the mental disorders that we evaluate under neurocognitive disorders (112.02), autism spectrum disorder (112.10), or personality and impulse-control disorders (112.08).
10. Eating disorders (112.13).
a. These disorders are characterized in young children by persistent eating of nonnutritive substances or repeated episodes of regurgitation and re-chewing of food, or by persistent failure to consume adequate nutrition by mouth. In adolescence, these disorders are characterized by disturbances in eating behavior and preoccupation with, and excessive self-evaluation of, body weight and shape. Symptoms and signs may include, but are not limited to, failure to make expected weight gains; restriction of energy consumption when compared with individual requirements; recurrent episodes of binge eating or behavior intended to prevent weight gain, such as self-induced vomiting, excessive exercise, or misuse of laxatives; mood disturbances, social withdrawal, or irritability; amenorrhea; dental problems; abnormal laboratory findings; and cardiac abnormalities.
b. Examples of disorders that we evaluate in this category include anorexia nervosa, bulimia nervosa, binge-eating disorder, and avoidant/restrictive food disorder.
11. Developmental disorders in infants and toddlers (112.14).
a. Developmental disorders are characterized by a delay or deficit in the development of age-appropriate skills, or a loss of previously acquired skills, involving motor planning and control, learning, relating and communicating, and self-regulating.
b. Examples of disorders that we evaluate in this category include developmental coordination disorder, separation anxiety disorder, autism spectrum disorder, and regulation disorders of sensory processing (difficulties in regulating emotions, behaviors, and motor abilities in response to sensory stimulation). Some infants and toddlers may have only a general diagnosis of “developmental delay.”
c. This category does not include eating disorders related to low birth weight and failure to thrive, which we evaluate under that body system (100.00).
12. Trauma- and stressor-related disorders (112.15).
a. These disorders are characterized by experiencing or witnessing a traumatic or stressful event, or learning of a traumatic event occurring to a close family member or close friend, and the psychological aftermath of clinically significant effects on functioning. Symptoms and signs may include, but are not limited to, distressing memories, dreams, and flashbacks related to the trauma or stressor; avoidant or withdrawn behavior; constriction of play and significant activities; increased frequency of negative emotional states (for example, fear, sadness) or reduced expression of positive emotions (for example, satisfaction, affection); anxiety; irritability; aggression; exaggerated startle response; difficulty concentrating; sleep disturbance; and a loss of previously acquired developmental skills.
b. Examples of disorders that we evaluate in this category include posttraumatic stress disorder, reactive attachment disorder, and other specified trauma- and stressor-related disorders (such as adjustment-like disorders with prolonged duration without prolonged duration of stressor).
c. This category does not include the mental disorders that we evaluate under anxiety and obsessive-compulsive disorders (112.06), and cognitive impairments that result from neurological disorders, such as a traumatic brain injury, which we evaluate under neurocognitive disorders (112.02).
C. What evidence do we need to evaluate your mental disorder?
1. General. We need objective medical evidence from an acceptable medical source to establish that you have a medically determinable mental disorder. We also need evidence to assess the severity of your mental disorder and its effects on your ability to function age-appropriately. We will determine the extent and kinds of evidence we need from medical and nonmedical sources based on the individual facts about your disorder. For additional evidence requirements for intellectual disorder (112.05), see 112.00H. For our basic rules on evidence, see §§ 416.912, 416.913, and 416.920b of this chapter. For our rules on evaluating medical opinions, see §§ 416.1520c and 416.927 of this chapter. For our rules on evidence about your symptoms, see § 416.929 of this chapter.
2. Evidence from medical sources. We will consider all relevant medical evidence about your disorder from your physician, psychologist, and other medical sources, which include health care providers such as physician assistants, psychiatric nurse practitioners, licensed clinical social workers, and clinical mental health counselors. Evidence from your medical sources may include:
a. Your reported symptoms.
b. Your developmental, medical, psychiatric, and psychological history.
c. The results of physical or mental status examinations, structured clinical interviews, psychiatric or psychological rating scales, measures of adaptive functioning, or other clinical findings.
d. Developmental assessments, psychological testing, imaging results, or other laboratory findings.
e. Your diagnosis.
f. The type, dosage, and beneficial effects of medications you take.
g. The type, frequency, duration, and beneficial effects of therapy you receive.
h. Side effects of medication or other treatment that limit your ability to function.
i. Your clinical course, including changes in your medication, therapy, or other treatment, and the time required for therapeutic effectiveness.
j. Observations and descriptions of how you function during examinations or therapy.
k. Information about sensory, motor, or speech abnormalities, or about your cultural background (for example, language or customs) that may affect an evaluation of your mental disorder.
l. The expected duration of your symptoms and signs and their effects on your ability to function age-appropriately, both currently and in the future.
3. Evidence from you and people who know you. We will consider all relevant evidence about your mental disorder and your daily functioning that we receive from you and from people who know you. If you are too young or unable to describe your symptoms and your functioning, we will ask for a description from the person who is most familiar with you. We will ask about your symptoms, your daily functioning, and your medical treatment. We will ask for information from third parties who can tell us about your mental disorder, but we must have permission to do so. This evidence may include information from your family, caregivers, teachers, other educators, neighbors, clergy, case managers, social workers, shelter staff, or other community support and outreach workers. We will consider whether your statements and the statements from third parties are consistent with the medical and other evidence we have.
4. Evidence from early intervention programs, school, vocational training, work, and work-related programs.
a. Early intervention programs. You may receive services in an Early Intervention Program (EIP) to help you with your developmental needs. If so, we will consider information from your Individualized Family Service Plan (IFSP) and the early intervention specialists who help you.
b. School. You may receive special education or related services at your preschool or school. If so, we will try to obtain information from your school sources when we need it to assess how your mental disorder affects your ability to function. Examples of this information include your Individualized Education Programs (IEPs), your Section 504 plans, comprehensive evaluation reports, school-related therapy progress notes, information from your teachers about how you function in a classroom setting, and information from special educators, nurses, school psychologists, and occupational, physical, and speech/language therapists about any special education services or accommodations you receive at school.
c. Vocational training, work, and work-related programs. You may have recently participated in or may still be participating in vocational training, work-related programs, or work activity. If so, we will try to obtain information from your training program or your employer when we need it to assess how your mental disorder affects your ability to function. Examples of this information include training or work evaluations, modifications to your work duties or work schedule, and any special supports or accommodations you have required or now require in order to work. If you have worked or are working through a community mental health program, sheltered or supported work program, rehabilitation program, or transitional employment program, we will consider the type and degree of support you have received or are receiving in order to work (see 112.00D).
5. Need for longitudinal evidence.
a. General. Longitudinal medical evidence can help us learn how you function over time, and help us evaluate any variations in the level of your functioning. We will request longitudinal evidence of your mental disorder when your medical providers have records concerning you and your mental disorder over a period of months or perhaps years (see § 416.912(d) of this chapter).
b. Non-medical sources of longitudinal evidence. Certain situations, such as chronic homelessness, may make it difficult for you to provide longitudinal medical evidence. If you have a severe mental disorder, you will probably have evidence of its effects on your functioning over time, even if you have not had an ongoing relationship with the medical community or are not currently receiving treatment. For example, family members, caregivers, teachers, neighbors, former employers, social workers, case managers, community support staff, outreach workers, or government agencies may be familiar with your mental health history. We will ask for information from third parties who can tell us about your mental disorder, but you must give us permission to do so.
c. Absence of longitudinal evidence. In the absence of longitudinal evidence, we will use current objective medical evidence and all other relevant evidence available to us in your case record to evaluate your mental disorder. If we purchase a consultative examination to document your disorder, the record will include the results of that examination (see § 416.914 of this chapter). We will take into consideration your medical history, symptoms, clinical and laboratory findings, and medical source opinions. If you do not have longitudinal evidence, the current evidence alone may not be sufficient or appropriate to show that you have a disorder that meets the criteria of one of the mental disorders listings. In that case, we will follow the rules in 112.00K.
6. Evidence of functioning in unfamiliar situations or supportive situations.
a. Unfamiliar situations. We recognize that evidence about your functioning in unfamiliar situations does not necessarily show how you would function on a sustained basis in a school or other age-appropriate setting. In one-time, time-limited, or other unfamiliar situations, you may function differently than you do in familiar situations. In unfamiliar situations, you may appear more, or less, limited than you do on a daily basis and over time.
b. Supportive situations. Your ability to function in settings that are highly structured, or that are less demanding or more supportive than settings in which children your age without impairments typically function, does not necessarily demonstrate your ability to function age-appropriately.
c. Our assessment. We must assess your ability to function age-appropriately by evaluating all the evidence, such as reports about your functioning from third parties who are familiar with you, with an emphasis on how well you can initiate, sustain, and complete age-appropriate activities despite your impairment(s), compared to other children your age who do not have impairments.
D. How do we consider psychosocial supports, structured settings, living arrangements, and treatment when we evaluate the functioning of children?
1. General. Psychosocial supports, structured settings, and living arrangements, including assistance from your family or others, may help you by reducing the demands made on you. In addition, treatment you receive may reduce your symptoms and signs and possibly improve your functioning, or may have side effects that limit your functioning. Therefore, when we evaluate the effects of your mental disorder and rate the limitation of your areas of mental functioning, we will consider the kind and extent of supports you receive, the characteristics of any structured setting in which you spend your time (compared to children your age without impairments), and the effects of any treatment. This evidence may come from reports about your functioning from third parties who are familiar with you, and other third-party statements or information. Following are some examples of the supports you may receive:
a. You receive help from family members or other people in ways that children your age without impairments typically do not need in order to function age-appropriately. For example, an aide may accompany you on the school bus to help you control your actions or to monitor you to ensure you do not injure yourself or others.
b. You receive one-on-one assistance in your classes every day; or you have a full-time personal aide who helps you to function in your classroom; or you are a student in a self-contained classroom; or you attend a separate or alternative school where you receive special education services.
c. You participate in a special education or vocational training program, or a psychosocial rehabilitation day treatment or community support program, where you receive training in daily living and entry-level work skills.
d. You participate in a sheltered, supported, or transitional work program, or in a competitive employment setting with the help of a job coach or supervisor.
e. You receive comprehensive “24/7 wrap-around” mental health services while living in a group home or transitional housing, while participating in a semi-independent living program, or while living at home.
f. You live in a residential school, hospital, or other institution with 24-hour care.
g. You receive assistance from a crisis response team, social workers, or community mental health workers who help you meet your physical needs, and who may also represent you in dealings with government or community social services.
2. How we consider different levels of support and structure in psychosocial rehabilitation programs.
a. Psychosocial rehabilitation programs are based on your specific needs. Therefore, we cannot make any assumptions about your mental disorder based solely on the fact that you are associated with such a program. We must know the details of the program(s) in which you are involved and the pattern(s) of your involvement over time.
b. The kinds and levels of supports and structures in psychosocial rehabilitation programs typically occur on a scale of “most restrictive” to “least restrictive.” Participation in a psychosocial rehabilitation program at the most restrictive level would suggest greater limitation of your areas of mental functioning than would participation at a less restrictive level. The length of time you spend at different levels in a program also provides information about your functioning. For example, you could begin participation at the most restrictive crisis intervention level but gradually improve to the point of readiness for a lesser level of support and structure and, if you are an older adolescent, possibly some form of employment.
3. How we consider the help or support you receive.
a. We will consider the complete picture of your daily functioning, including the kinds, extent, and frequency of help and support you receive, when we evaluate your mental disorder and determine whether you are able to use the four areas of mental functioning age-appropriately. The fact that you have done, or currently do, some routine activities without help or support does not necessarily mean that you do not have a mental disorder or that you are not disabled. For example, you may be able to take age-appropriate care of your personal needs, or you may be old enough and able to cook, shop, and take public transportation. You may demonstrate both strengths and deficits in your daily functioning.
b. You may receive various kinds of help and support from others that enable you to do many things that, because of your mental disorder, you might not be able to do independently. Your daily functioning may depend on the special contexts in which you function. For example, you may spend your time among only familiar people or surroundings, in a simple and steady routine or an unchanging environment, or in a highly structured classroom or alternative school. However, this does not necessarily show whether you would function age-appropriately without those supports or contexts. (See 112.00H for further discussion of these issues regarding significant deficits in adaptive functioning for the purpose of 112.05.)
4. How we consider treatment. We will consider the effect of any treatment on your functioning when we evaluate your mental disorder. Treatment may include medication(s), psychotherapy, or other forms of intervention, which you receive in a doctor's office, during a hospitalization, or in a day program at a hospital or outpatient treatment program. With treatment, you may not only have your symptoms and signs reduced, but may also be able to function age-appropriately. However, treatment may not resolve all of the limitations that result from your mental disorder, and the medications you take or other treatment you receive for your disorder may cause side effects that limit your mental or physical functioning. For example, you may experience drowsiness, blunted affect, memory loss, or abnormal involuntary movements.
E. What are the paragraph B criteria for children age 3 to the attainment of age 18?
1. Understand, remember, or apply information (paragraph B1). This area of mental functioning refers to the abilities to learn, recall, and use information to perform age-appropriate activities. Examples include: Understanding and learning terms, instructions, procedures; following one- or two-step oral instructions to carry out a task; describing an activity to someone else; asking and answering questions and providing explanations; recognizing a mistake and correcting it; identifying and solving problems; sequencing multi-step activities; and using reason and judgment to make decisions. These examples illustrate the nature of the area of mental functioning. We do not require documentation of all of the examples. How you manifest this area of mental functioning and your limitations in using it depends, in part, on your age.
2. Interact with others (paragraph B2). This area of mental functioning refers to the abilities to relate to others age-appropriately at home, at school, and in the community. Examples include: Engaging in interactive play; cooperating with others; asking for help when needed; initiating and maintaining friendships; handling conflicts with others; stating own point of view; initiating or sustaining conversation; understanding and responding to social cues (physical, verbal, emotional); responding to requests, suggestions, criticism, correction, and challenges; and keeping social interactions free of excessive irritability, sensitivity, argumentativeness, or suspiciousness. These examples illustrate the nature of this area of mental functioning. We do not require documentation of all of the examples. How you manifest this area of mental functioning and your limitations in using it depends, in part, on your age.
3. Concentrate, persist, or maintain pace (paragraph B3). This area of mental functioning refers to the abilities to focus attention on activities and stay on task age-appropriately. Examples include: Initiating and performing an activity that you understand and know how to do; engaging in an activity at home or in school at an appropriate and consistent pace; completing tasks in a timely manner; ignoring or avoiding distractions while engaged in an activity or task; changing activities without being disruptive; engaging in an activity or task close to or with others without interrupting or distracting them; sustaining an ordinary routine and regular attendance at school; and engaging in activities at home, school, or in the community without needing an unusual amount of rest. These examples illustrate the nature of this area of mental functioning. We do not require documentation of all of the examples. How you manifest this area of mental functioning and your limitations in using it depends, in part, on your age.
4. Adapt or manage oneself (paragraph B4). This area of mental functioning refers to the abilities to regulate emotions, control behavior, and maintain well-being in age-appropriate activities and settings. Examples include: Responding to demands; adapting to changes; managing your psychologically based symptoms; distinguishing between acceptable and unacceptable performance in community- or school-related activities; setting goals; making plans independently of others; maintaining personal hygiene; and protecting yourself from harm and exploitation by others. These examples illustrate the nature of this area of mental functioning. We do not require documentation of all of the examples. How you manifest this area of mental functioning and your limitations in using it depends, in part, on your age.
F. How do we use the paragraph B criteria to evaluate mental disorders in children?
1. General. We use the paragraph B criteria to rate the degree of your limitations. We consider only the limitations that result from your mental disorder(s). We will determine whether you are able to use each of the paragraph B areas of mental functioning in age-appropriate activities in a manner comparable to that of other children your age who do not have impairments. We will consider, for example, the range of your activities and whether they are age-appropriate; how well you can initiate, sustain, and complete your activities; the kinds and frequency of help or supervision you receive; and the kinds of structured or supportive settings you need in order to function age-appropriately (see 112.00D).
2. Degrees of limitation. We evaluate the effects of your mental disorder on each of the four areas of mental functioning. To satisfy the paragraph B criteria, your mental disorder must result in extreme limitation of one, or marked limitation of two, paragraph B areas of mental functioning. See §§ 416.925(b)(2)(ii) and 416.926a(e) of this chapter for the definitions of the terms marked and extreme as they apply to children.
3. Rating the limitations of your areas of mental functioning.
a. General. We use all of the relevant medical and non-medical evidence in your case record to evaluate your mental disorder: The symptoms and signs of your disorder, the reported limitations in your activities, and any help and support you receive that is necessary for you to function. The medical evidence may include descriptors regarding the diagnostic stage or level of your disorder, such as “mild” or “moderate.” Clinicians may use these terms to characterize your medical condition. However, these terms will not always be the same as the degree of your limitation in a paragraph B area of mental functioning.
b. Areas of mental functioning in daily activities. You use the same four areas of mental functioning in daily activities at home, at school, and in the community. With respect to a particular task or activity, you may have trouble using one or more of the areas. For example, you may have difficulty understanding and remembering what to do; or concentrating and staying on task long enough to do it; or engaging in the task or activity with other people; or trying to do the task without becoming frustrated and losing self-control. Information about your daily functioning in your activities at home, at school, or in your community can help us understand whether your mental disorder limits one or more of these areas; and, if so, whether it also affects your ability to function age-appropriately.
c. Overall effect of limitations. Limitation of an area of mental functioning reflects the overall degree to which your mental disorder interferes with that area. The degree of limitation does not necessarily reflect a specific type or number of activities, including activities of daily living, that you have difficulty doing. In addition, no single piece of information (including test results) can establish whether you have extreme or marked limitation of an area of mental functioning.
d. Effects of support, supervision, structure on functioning. The degree of limitation of an area of mental functioning also reflects the kind and extent of supports or supervision you receive (beyond what other children your age without impairments typically receive) and the characteristics of any structured setting where you spend your time, which enable you to function. The more extensive the support you need from others (beyond what is age-appropriate) or the more structured the setting you need in order to function, the more limited we will find you to be (see 112.00D).
e. Specific instructions for paragraphs B1, B3, and B4. For paragraphs B1, B3, and B4, the greatest degree of limitation of any part of the area of mental functioning directs the rating of limitation of that whole area of mental functioning.
(i) To do an age-appropriate activity, you must be able to understand and remember and apply information required by the activity. Similarly, you must be able to concentrate and persist and maintain pace in order to complete the activity, and adapt and manage yourself age-appropriately. Limitation in any one of these parts (understand or remember or apply; concentrate or persist or maintain pace; adapt or manage oneself) may prevent you from completing age-appropriate activities.
(ii) We will document the rating of limitation of the whole area of mental functioning, not each individual part. We will not add ratings of the parts together. For example, with respect to paragraph B3, if you have marked limitation in concentrating, but your limitations in persisting and maintaining pace do not rise to a marked level, we will find that you have marked limitation in the whole paragraph B3 area of mental functioning.
(iii) Marked limitation in more than one part of the same paragraph B area of mental functioning does not satisfy the requirement to have marked limitation in two paragraph B areas of mental functioning.
4. How we evaluate mental disorders involving exacerbations and remissions.
a. When we evaluate the effects of your mental disorder, we will consider how often you have exacerbations and remissions, how long they last, what causes your mental disorder to worsen or improve, and any other relevant information. We will assess whether your mental impairment(s) causes marked or extreme limitation of the affected paragraph B area(s) of mental functioning (see 112.00F2). We will consider whether you can use the area of mental functioning age-appropriately on a sustained basis. We will not find that you function age-appropriately solely because you have a period(s) of improvement (remission), or that you are disabled solely because you have a period of worsening (exacerbation), of your mental disorder.
b. If you have a mental disorder involving exacerbations and remissions, you may be able to use the four areas of mental functioning at home, at school, or in the community for a few weeks or months. Recurrence or worsening of symptoms and signs, however, can interfere enough to render you unable to function age-appropriately.
G. What are the paragraph C criteria, and how do we use them to evaluate mental disorders in children age 3 to the attainment of age 18?
1. General. The paragraph C criteria are an alternative to the paragraph B criteria under listings 112.02, 112.03, 112.04, 112.06, and 112.15. We use the paragraph C criteria to evaluate mental disorders that are “serious and persistent.” In the paragraph C criteria, we recognize that mental health interventions may control the more obvious symptoms and signs of your mental disorder.
2. Paragraph C criteria.
a. We find a mental disorder to be “serious and persistent” when there is a medically documented history of the existence of the mental disorder in the listing category over a period of at least 2 years, and evidence shows that your disorder satisfies both C1 and C2.
b. The criterion in C1 is satisfied when the evidence shows that you rely, on an ongoing basis, upon medical treatment, mental health therapy, psychosocial support(s), or a highly structured setting(s), to diminish the symptoms and signs of your mental disorder (see 112.00D). We consider that you receive ongoing medical treatment when the medical evidence establishes that you obtain medical treatment with a frequency consistent with accepted medical practice for the type of treatment or evaluation required for your medical condition. We will consider periods of inconsistent treatment or lack of compliance with treatment that may result from your mental disorder. If the evidence indicates that the inconsistent treatment or lack of compliance is a feature of your mental disorder, and it has led to an exacerbation of your symptoms and signs, we will not use it as evidence to support a finding that you have not received ongoing medical treatment as required by this paragraph.
c. The criterion in C2 is satisfied when the evidence shows that, despite your diminished symptoms and signs, you have achieved only marginal adjustment. “Marginal adjustment” means that your adaptation to the requirements of daily life is fragile; that is, you have minimal capacity to adapt to changes in your environment or to demands that are not already part of your daily life. We will consider that you have achieved only marginal adjustment when the evidence shows that changes or increased demands have led to exacerbation of your symptoms and signs and to deterioration in your functioning; for example, you have become unable to function outside of your home or a more restrictive setting, without substantial psychosocial supports (see 112.00D). Such deterioration may have necessitated a significant change in medication or other treatment. Similarly, because of the nature of your mental disorder, evidence may document episodes of deterioration that have required you to be hospitalized or absent from school, making it difficult for you to sustain age-appropriate activity over time.
H. How do we document and evaluate intellectual disorder under 112.05?
1. General. Listing 112.05 is based on the two elements that characterize intellectual disorder for children up to age 18: Significantly subaverage general intellectual functioning and significant deficits in current adaptive functioning.
2. Establishing significantly subaverage general intellectual functioning.
a. Definition. Intellectual functioning refers to the general mental capacity to learn, reason, plan, solve problems, and perform other cognitive functions. Under 112.05A, we identify significantly subaverage general intellectual functioning by the cognitive inability to function at a level required to participate in standardized intelligence testing. Our findings under 112.05A are based on evidence from an acceptable medical source. Under 112.05B, we identify significantly subaverage general intellectual functioning by an IQ score(s) on an individually administered standardized test of general intelligence that meets program requirements and has a mean of 100 and a standard deviation of 15. A qualified specialist (see 112.00H2c) must administer the standardized intelligence testing.
b. Psychometric standards. We will find standardized intelligence test results usable for the purposes of 112.05B1 when the measure employed meets contemporary psychometric standards for validity, reliability, normative data, and scope of measurement; and a qualified specialist has individually administered the test according to all pre-requisite testing conditions.
c. Qualified specialist. A “qualified specialist” is currently licensed or certified at the independent level of practice in the State where the test was performed, and has the training and experience to administer, score, and interpret intelligence tests. If a psychological assistant or paraprofessional administered the test, a supervisory qualified specialist must interpret the test findings and co-sign the examination report.
d. Responsibility for conclusions based on testing. We generally presume that your obtained IQ score(s) is an accurate reflection of your general intellectual functioning, unless evidence in the record suggests otherwise. Examples of this evidence include: A statement from the test administrator indicating that your obtained score is not an accurate reflection of your general intellectual functioning, prior or internally inconsistent IQ scores, or information about your daily functioning. Only qualified specialists, Federal and State agency medical and psychological consultants, and other contracted medical and psychological experts may conclude that your obtained IQ score(s) is not an accurate reflection of your general intellectual functioning. This conclusion must be well supported by appropriate clinical and laboratory diagnostic techniques and must be based on relevant evidence in the case record, such as:
(i) The data obtained in testing;
(ii) Your developmental history, including when your signs and symptoms began;
(iii) Information about how you function on a daily basis in a variety of settings; and
(iv) Clinical observations made during the testing period, such as your ability to sustain attention, concentration, and effort; to relate appropriately to the examiner; and to perform tasks independently without prompts or reminders.
3. Establishing significant deficits in adaptive functioning.
a. Definition. Adaptive functioning refers to how you learn and use conceptual, social, and practical skills in dealing with common life demands. It is your typical functioning at home, at school, and in the community, alone or among others. Under 112.05A, we identify significant deficits in adaptive functioning based on your dependence on others to care for your personal needs, such as eating and bathing (grossly in excess of age-appropriate dependence). We will base our conclusions about your adaptive functioning on evidence from a variety of sources (see 112.00H3b) and not on your statements alone. Under 112.05B2, we identify significant deficits in adaptive functioning based on whether there is extreme limitation of one, or marked limitation of two, of the paragraph B criteria (see 112.00E; 112.00F).
b. Evidence. Evidence about your adaptive functioning may come from:
(i) Medical sources, including their clinical observations;
(ii) Standardized tests of adaptive functioning (see 112.00H3c);
(iii) Third party information, such as a report of your functioning from a family member or your caregiver;
(iv) School records;
(v) A teacher questionnaire;
(vi) Reports from employers or supervisors; and
(vii) Your own statements about how you handle all of your daily activities.
c. Standardized tests of adaptive functioning. We do not require the results of an individually administered standardized test of adaptive functioning. If your case record includes these test results, we will consider the results along with all other relevant evidence; however, we will use the guidelines in 112.00E and F to evaluate and determine the degree of your deficits in adaptive functioning, as required under 112.05B2.
d. Standardized developmental assessments. We do not require the results of standardized developmental assessments, which compare your level of development to the level typically expected for your chronological age. If your case record includes test results, we will consider the results along with all other relevant evidence. However, we will use the guidelines in 112.00E and F to evaluate and determine the degree of your deficits in adaptive functioning, as required under 112.05B2.
e. How we consider common everyday activities.
(i) The fact that you engage in common everyday activities, such as caring for your personal needs, preparing simple meals, or driving a car, will not always mean that you do not have deficits in adaptive functioning as required by 112.05B2. You may demonstrate both strengths and deficits in your adaptive functioning. However, a lack of deficits in one area does not negate the presence of deficits in another area. When we assess your adaptive functioning, we will consider all of your activities and your performance of them.
(ii) Our conclusions about your adaptive functioning rest on the quality of your daily activities and whether you do them age-appropriately. If you receive help in performing your activities, we need to know the kind, extent, and frequency of help you receive in order to perform them. We will not assume that your ability to do some common everyday activities, or to do some things without help or support, demonstrates that your mental disorder does not meet the requirements of 112.05B2. (See 112.00D regarding the factors we consider when we evaluate your functioning, including how we consider any help or support you receive.)
f. How we consider work activity. The fact that you have engaged in work activity, or that you work intermittently or steadily in a job commensurate with your abilities, will not always mean that you do not have deficits in adaptive functioning as required by 112.05B2. When you have engaged in work activity, we need complete information about the work, and about your functioning in the work activity and work setting, before we reach any conclusions about your adaptive functioning. We will consider all factors involved in your work history before concluding whether your impairment satisfies the criteria for intellectual disorder under 112.05B. We will consider your prior and current work history, if any, and various other factors influencing how you function. For example, we consider whether the work was in a supported setting, whether you required more supervision than other employees, how your job duties compared to others in the same job, how much time it took you to learn the job duties, and the reason the work ended, if applicable.
I. What additional considerations do we use to evaluate developmental disorders of infants and toddlers?
1. General. We evaluate developmental disorders from birth to attainment of age 3 under 112.14. We evaluate your ability to acquire and maintain the motor, cognitive, social/communicative, and emotional skills that you need to function age-appropriately. When we rate your impairment-related limitations for this listing (see §§ 416.925(b)(2)(ii) and 416.926a(e) of this chapter), we consider only limitations you have because of your developmental disorder. If you have a chronic illness or physical abnormality(ies), we will evaluate it under the affected body system, for example, the cardiovascular or musculoskeletal system.
2. Age and typical development in early childhood.
a. Prematurity and age. If you were born prematurely, we will use your corrected chronological age (CCA) for comparison. CCA is your chronological age adjusted by a period of gestational prematurity. CCA = (chronological age)−(number of weeks premature). If you have not attained age 1, we will correct your chronological age, using the same formula. If you are over age 1, we will decide whether to correct your chronological age, based on our judgment and all the facts of your case (see § 416.924b(b) of this chapter).
b. Developmental assessment. We will use the results from a standardized developmental assessment to compare your level of development with that typically expected for your chronological age. When there are no results from a comprehensive standardized developmental assessment in the case record, we need narrative developmental reports from your medical sources in sufficient detail to assess the limitations resulting from your developmental disorder.
c. Variation. When we evaluate your developmental disorder, we will consider the wide variation in the range of normal or typical development in early childhood. At the end of a recognized milestone period, new skills typically begin to emerge. If your new skills begin to emerge later than is typically expected, the timing of their emergence may or may not indicate that you have a developmental delay or deficit that can be expected to last for 1 year.
3. Evidence.
a. Standardized developmental assessments. We use standardized test reports from acceptable medical sources or from early intervention specialists, physical or occupational therapists, and other qualified professionals. Only the qualified professional who administers the test, Federal and State agency medical and psychological consultants, and other contracted medical and psychological experts may conclude that the assessment results are not an accurate reflection of your development. This conclusion must be well supported by appropriate clinical and laboratory diagnostic techniques and must be based on relevant evidence in the case record. If the assessment results are not an accurate reflection of your development, we may purchase a new developmental assessment. If the developmental assessment is inconsistent with other information in your case record, we will follow the guidelines in § 416.920b of this chapter.
b. Narrative developmental reports. A narrative developmental report is based on clinical observations, progress notes, and well-baby check-ups, and includes your developmental history, examination findings (with abnormal findings noted on repeated examinations), and an overall assessment of your development (that is, more than one or two isolated skills) by the medical source. Although medical sources may refer to screening test results as supporting evidence in the narrative developmental report, screening test results alone cannot establish a diagnosis or the severity of developmental disorder.
4. What are the paragraph B criteria for 112.14?
a. General. The paragraph B criteria for 112.14 are slightly different from the paragraph B criteria for the other listings. They are the developmental abilities that infants and toddlers use to acquire and maintain the skills needed to function age-appropriately. An infant or toddler is expected to use his or her developmental abilities to achieve a recognized pattern of milestones, over a typical range of time, in order to acquire and maintain the skills needed to function age-appropriately. We will find that your developmental disorder satisfies the requirements of 112.14 if it results in extreme limitation of one, or marked limitation of two, of the 112.14 paragraph B criteria. (See §§ 416.925(b)(2)(ii) and 416.926a(e) of this chapter for the definitions of the terms marked and extreme as they apply to children.)
b. Definitions of the 112.14 paragraph B developmental abilities.
(i) Ability to plan and control motor movement. This criterion refers to the developmental ability to plan, remember, and execute controlled motor movements by integrating and coordinating perceptual and sensory input with motor output. Using this ability develops gross and fine motor skills, and makes it possible for you to engage in age-appropriate symmetrical or alternating motor activities. You use this ability when, for example, you grasp and hold objects with one or both hands, pull yourself up to stand, walk without holding on, and go up and down stairs with alternating feet. These examples illustrate the nature of the developmental ability. We do not require documentation of all of the examples. How you manifest this developmental ability and your limitations in using it depends, in part, on your age.
(ii) Ability to learn and remember. This criterion refers to the developmental ability to learn by exploring the environment, engaging in trial-and-error experimentation, putting things in groups, understanding that words represent things, and participating in pretend play. Using this ability develops the skills that help you understand what things mean, how things work, and how you can make things happen. You use this ability when, for example, you show interest in objects that are new to you, imitate simple actions, name body parts, understand simple cause-and-effect relationships, remember simple directions, or figure out how to take something apart. These examples illustrate the nature of the developmental ability. We do not require documentation of all of the examples. How you manifest this developmental ability and your limitations in using it depends, in part, on your age.
(iii) Ability to interact with others. This criterion refers to the developmental ability to participate in reciprocal social interactions and relationships by communicating your feelings and intents through vocal and visual signals and exchanges; physical gestures and contact; shared attention and affection; verbal turn taking; and understanding and sending increasingly complex messages. Using this ability develops the social skills that make it possible for you to influence others (for example, by gesturing for a toy or saying “no” to stop an action); invite someone to interact with you (for example, by smiling or reaching); and draw someone's attention to what interests you (for example, by pointing or taking your caregiver's hand and leading that person). You use this ability when, for example, you use vocalizations to initiate and sustain a “conversation” with your caregiver; respond to limits set by an adult with words, gestures, or facial expressions; play alongside another child; or participate in simple group activities with adult help. These examples illustrate the nature of the developmental ability. We do not require documentation of all of the examples. How you manifest this developmental ability and your limitations in using it depends, in part, on your age.
(iv) Ability to regulate physiological functions, attention, emotion, and behavior. This criterion refers to the developmental ability to stabilize biological rhythms (for example, by developing an age-appropriate sleep/wake cycle); control physiological functions (for example, by achieving regular patterns of feeding); and attend, react, and adapt to environmental stimuli, persons, objects, and events (for example, by becoming alert to things happening around you and in relation to you, and responding without overreacting or underreacting). Using this ability develops the skills you need to regulate yourself and makes it possible for you to achieve and maintain a calm, alert, and organized physical and emotional state. You use this ability when, for example, you recognize your body's needs for food or sleep, focus quickly and pay attention to things that interest you, cry when you are hurt but become quiet when your caregiver holds you, comfort yourself with your favorite toy when you are upset, ask for help when something frustrates you, or refuse help from your caregiver when trying to do something for yourself. These examples illustrate the nature of the developmental ability. We do not require documentation of all of the examples. How you manifest this developmental ability and your limitations in using it depends, in part, on your age.
5. Deferral of determination.
a. Full-term infants. In the first few months of life, full-term infants typically display some irregularities in observable behaviors (for example, sleep cycles, feeding, responding to stimuli, attending to faces, self-calming), making it difficult to assess the presence, extent, and duration of a developmental disorder. When the evidence indicates that you may have a significant developmental delay, but there is insufficient evidence to make a determination, we will defer making a disability determination under 112.14 until you are at least 6 months old. This deferral will allow us to obtain a longitudinal medical history so that we can more accurately evaluate your developmental patterns and functioning over time. In most cases, when you are at least 6 months old, any developmental delay you may have can be better assessed, and you can undergo standardized developmental testing, if indicated.
b. Premature infants. When the evidence indicates that you may have a significant developmental delay, but there is insufficient evidence to make a determination, we will defer your case until you attain a CCA (see 112.00I2a) of at least 6 months in order to better evaluate your developmental delay.
c. When we will not defer a determination. We will not defer our determination if we have sufficient evidence to determine that you are disabled under 112.14 or any other listing, or that you have an impairment or combination of impairments that functionally equals the listings. In addition, we will not defer our determination if the evidence demonstrates that you are not disabled.
J. How do we evaluate substance use disorders? If we find that you are disabled and there is medical evidence in your case record establishing that you have a substance use disorder, we will determine whether your substance use disorder is a contributing factor material to the determination of disability (see § 416.935 of this chapter).
K. How do we evaluate mental disorders that do not meet one of the mental disorders listings?
1. These listings include only examples of mental disorders that we consider serious enough to result in marked and severe functional limitations. If your severe mental disorder does not meet the criteria of any of these listings, we will consider whether you have an impairment(s) that meets the criteria of a listing in another body system. You may have another impairment(s) that is secondary to your mental disorder. For example, if you have an eating disorder and develop a cardiovascular impairment because of it, we will evaluate your cardiovascular impairment under the listings for the cardiovascular body system.
2. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing (see § 416.926 of this chapter).
3. If your impairment(s) does not meet or medically equal a listing, we will consider whether you have an impairment(s) that functionally equals the listings (see § 416.926a of this chapter).
4. Although we present these alternatives in a specific sequence above, each represents listing-level severity, and we can evaluate your claim in any order. For example, if the factors of your case indicate that the combination of your impairments may functionally equal the listings, we may start with that analysis. We use the rules in § 416.994a of this chapter, as appropriate, when we decide whether you continue to be disabled.
112.01 Category of Impairments, Mental Disorders
112.02 Neurocognitive disorders (see 112.00B1), for children age 3 to attainment of age 18, satisfied by A and B, or A and C:
A. Medical documentation of a clinically significant deviation in normal cognitive development or by significant cognitive decline from a prior level of functioning in one or more of the cognitive areas:
1. Complex attention;
2. Executive function;
3. Learning and memory;
4. Language;
5. Perceptual-motor; or
6. Social cognition.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 112.00F):
1. Understand, remember, or apply information (see 112.00E1).
2. Interact with others (see 112.00E2).
3. Concentrate, persist, or maintain pace (see 112.00E3).
4. Adapt or manage oneself (see 112.00E4).
OR
C. Your mental disorder in this listing category is “serious and persistent;” that is, you have a medically documented history of the existence of the disorder over a period of at least 2 years, and there is evidence of both:
1. Medical treatment, mental health therapy, psychosocial support(s), or a highly structured setting(s) that is ongoing and that diminishes the symptoms and signs of your mental disorder (see 112.00G2b); and
2. Marginal adjustment, that is, you have minimal capacity to adapt to changes in your environment or to demands that are not already part of your daily life (see 112.00G2c).
112.03 Schizophrenia spectrum and other psychotic disorders (see 112.00B2), for children age 3 to attainment of age 18, satisfied by A and B, or A and C:
A. Medical documentation of one or more of the following:
1. Delusions or hallucinations;
2. Disorganized thinking (speech); or
3. Grossly disorganized behavior or catatonia.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 112.00F):
1. Understand, remember, or apply information (see 112.00E1).
2. Interact with others (see 112.00E2).
3. Concentrate, persist, or maintain pace (see 112.00E3).
4. Adapt or manage oneself (see 112.00E4).
OR
C. Your mental disorder in this listing category is “serious and persistent;” that is, you have a medically documented history of the existence of the disorder over a period of at least 2 years, and there is evidence of both:
1. Medical treatment, mental health therapy, psychosocial support(s), or a highly structured setting(s) that is ongoing and that diminishes the symptoms and signs of your mental disorder (see 112.00G2b); and
2. Marginal adjustment, that is, you have minimal capacity to adapt to changes in your environment or to demands that are not already part of your daily life (see 112.00G2c).
112.04 Depressive, bipolar and related disorders (see 112.00B3), for children age 3 to attainment of age 18, satisfied by A and B, or A and C:
A. Medical documentation of the requirements of paragraph 1, 2, or 3:
1. Depressive disorder, characterized by five or more of the following:
a. Depressed or irritable mood;
b. Diminished interest in almost all activities;
c. Appetite disturbance with change in weight (or a failure to achieve an expected weight gain);
d. Sleep disturbance;
e. Observable psychomotor agitation or retardation;
f. Decreased energy;
g. Feelings of guilt or worthlessness;
h. Difficulty concentrating or thinking; or
i. Thoughts of death or suicide.
2. Bipolar disorder, characterized by three or more of the following:
a. Pressured speech;
b. Flight of ideas;
c. Inflated self-esteem;
d. Decreased need for sleep;
e. Distractibility;
f. Involvement in activities that have a high probability of painful consequences that are not recognized; or
g. Increase in goal-directed activity or psychomotor agitation.
3. Disruptive mood dysregulation disorder, beginning prior to age 10, and all of the following:
a. Persistent, significant irritability or anger;
b. Frequent, developmentally inconsistent temper outbursts; and
c. Frequent aggressive or destructive behavior.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 112.00F):
1. Understand, remember, or apply information (see 112.00E1).
2. Interact with others (see 112.00E2).
3. Concentrate, persist, or maintain pace (see 112.00E3).
4. Adapt or manage oneself (see 112.00E4).
OR
C. Your mental disorder in this listing category is “serious and persistent;” that is, you have a medically documented history of the existence of the disorder over a period of at least 2 years, and there is evidence of both:
1. Medical treatment, mental health therapy, psychosocial support(s), or a highly structured setting(s) that is ongoing and that diminishes the symptoms and signs of your mental disorder (see 112.00G2b); and
2. Marginal adjustment, that is, you have minimal capacity to adapt to changes in your environment or to demands that are not already part of your daily life (see 112.00G2c).
112.05 Intellectual disorder (see 112.00B4), for children age 3 to attainment of age 18, satisfied by A or B:
A. Satisfied by 1 and 2 (see 112.00H):
1. Significantly subaverage general intellectual functioning evident in your cognitive inability to function at a level required to participate in standardized testing of intellectual functioning; and
2. Significant deficits in adaptive functioning currently manifested by your dependence upon others for personal needs (for example, toileting, eating, dressing, or bathing) in excess of age-appropriate dependence.
OR
B. Satisfied by 1 and 2 (see 112.00H):
1. Significantly subaverage general intellectual functioning evidenced by a or b:
a. A full scale (or comparable) IQ score of 70 or below on an individually administered standardized test of general intelligence; or
b. A full scale (or comparable) IQ score of 71-75 accompanied by a verbal or performance IQ score (or comparable part score) of 70 or below on an individually administered standardized test of general intelligence; and
2. Significant deficits in adaptive functioning currently manifested by extreme limitation of one, or marked limitation of two, of the following areas of mental functioning:
a. Understand, remember, or apply information (see 112.00E1); or
b. Interact with others (see 112.00E2); or
c. Concentrate, persist, or maintain pace (see 112.00E3); or
d. Adapt or manage oneself (see 112.00E4).
112.06 Anxiety and obsessive-compulsive disorders (see 112.00B5), for children age 3 to attainment of age 18, satisfied by A and B, or A and C:
A. Medical documentation of the requirements of paragraph 1, 2, 3, or 4:
1. Anxiety disorder, characterized by one or more of the following:
a. Restlessness;
b. Easily fatigued;
c. Difficulty concentrating;
d. Irritability;
e. Muscle tension; or
f. Sleep disturbance.
2. Panic disorder or agoraphobia, characterized by one or both:
a. Panic attacks followed by a persistent concern or worry about additional panic attacks or their consequences; or
b. Disproportionate fear or anxiety about at least two different situations (for example, using public transportation, being in a crowd, being in a line, being outside of your home, being in open spaces).
3. Obsessive-compulsive disorder, characterized by one or both:
a. Involuntary, time-consuming preoccupation with intrusive, unwanted thoughts; or;
b. Repetitive behaviors that appear aimed at reducing anxiety.
4. Excessive fear or anxiety concerning separation from those to whom you are attached.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 112.00F):
1. Understand, remember, or apply information (see 112.00E1).
2. Interact with others (see 112.00E2).
3. Concentrate, persist, or maintain pace (see 112.00E3).
4. Adapt or manage oneself (see 112.00E4).
OR
C. Your mental disorder in this listing category is “serious and persistent;” that is, you have a medically documented history of the existence of the disorder over a period of at least 2 years, and there is evidence of both:
1. Medical treatment, mental health therapy, psychosocial support(s), or a highly structured setting(s) that is ongoing and that diminishes the symptoms and signs of your mental disorder (see 112.00G2b); and
2. Marginal adjustment, that is, you have minimal capacity to adapt to changes in your environment or to demands that are not already part of your daily life (see 112.00G2c).
112.07 Somatic symptom and related disorders (see 112.00B6), for children age 3 to attainment of age 18, satisfied by A and B:
A. Medical documentation of one or both of the following:
1. Symptoms of altered voluntary motor or sensory function that are not better explained by another medical or mental disorder; or
2. One or more somatic symptoms that are distressing, with excessive thoughts, feelings, or behaviors related to the symptoms.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 112.00F):
1. Understand, remember, or apply information (see 112.00E1).
2. Interact with others (see 112.00E2).
3. Concentrate, persist, or maintain pace (see 112.00E3).
4. Adapt or manage oneself (see 112.00E4).
112.08 Personality and impulse-control disorders (see 112.00B7), for children age 3 to attainment of age 18, satisfied by A and B:
A. Medical documentation of a pervasive pattern of one or more of the following:
1. Distrust and suspiciousness of others;
2. Detachment from social relationships;
3. Disregard for and violation of the rights of others;
4. Instability of interpersonal relationships;
5. Excessive emotionality and attention seeking;
6. Feelings of inadequacy;
7. Excessive need to be taken care of;
8. Preoccupation with perfectionism and orderliness; or
9. Recurrent, impulsive, aggressive behavioral outbursts.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 112.00F):
1. Understand, remember, or apply information (see 112.00E1).
2. Interact with others (see 112.00E2).
3. Concentrate, persist, or maintain pace (see 112.00E3).
4. Adapt or manage oneself (see 112.00E4).
112.09 [Reserved]
112.10 Autism spectrum disorder (see 112.00B8), for children age 3 to attainment of age 18), satisfied by A and B:
A. Medical documentation of both of the following:
1. Qualitative deficits in verbal communication, nonverbal communication, and social interaction; and
2. Significantly restricted, repetitive patterns of behavior, interests, or activities.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 112.00F):
1. Understand, remember, or apply information (see 112.00E1).
2. Interact with others (see 112.00E2).
3. Concentrate, persist, or maintain pace (see 112.00E3).
4. Adapt or manage oneself (see 112.00E4).
112.11 Neurodevelopmental disorders (see 112.00B9), for children age 3 to attainment of age 18, satisfied by A and B:
A. Medical documentation of the requirements of paragraph 1, 2, or 3:
1. One or both of the following:
a. Frequent distractibility, difficulty sustaining attention, and difficulty organizing tasks; or
b. Hyperactive and impulsive behavior (for example, difficulty remaining seated, talking excessively, difficulty waiting, appearing restless, or behaving as if being “driven by a motor”).
2. Significant difficulties learning and using academic skills; or
3. Recurrent motor movement or vocalization.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 112.00F):
1. Understand, remember, or apply information (see 112.00E1).
2. Interact with others (see 112.00E2).
3. Concentrate, persist, or maintain pace (see 112.00E3).
4. Adapt or manage oneself (see 112.00E4).
112.12 [Reserved]
112.13 Eating disorders (see 112.00B10), for children age 3 to attainment of age 18, satisfied by A and B:
A. Medical documentation of a persistent alteration in eating or eating-related behavior that results in a change in consumption or absorption of food and that significantly impairs physical or psychological health.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 112.00F):
1. Understand, remember, or apply information (see 112.00E1).
2. Interact with others (see 112.00E2).
3. Concentrate, persist, or maintain pace (see 112.00E3).
4. Adapt or manage oneself (see 112.00E4).
112.14 Developmental disorders in infants and toddlers (see 112.00B11, 112.00I), satisfied by A and B:
A. Medical documentation of one or both of the following:
1. A delay or deficit in the development of age-appropriate skills; or
2. A loss of previously acquired skills.
AND
B. Extreme limitation of one, or marked limitation of two, of the following developmental abilities (see 112.00F):
1. Plan and control motor movement (see 112.00I4b(i)).
2. Learn and remember (see 112.00I4b(ii)).
3. Interact with others (see 112.00I4b(iii)).
4. Regulate physiological functions, attention, emotion, and behavior (see 112.00I4b(iv)).
112.15 Trauma- and stressor-related disorders (see 112.00B11), for children age 3 to attainment of age 18, satisfied by A and B, or A and C:
A. Medical documentation of the requirements of paragraph 1 or 2:
1. Posttraumatic stress disorder, characterized by all of the following:
a. Exposure to actual or threatened death, serious injury, or violence;
b. Subsequent involuntary re-experiencing of the traumatic event (for example, intrusive memories, dreams, or flashbacks);
c. Avoidance of external reminders of the event;
d. Disturbance in mood and behavior (for example, developmental regression, socially withdrawn behavior); and
e. Increases in arousal and reactivity (for example, exaggerated startle response, sleep disturbance).
2. Reactive attachment disorder, characterized by two or all of the following:
a. Rarely seeks comfort when distressed;
b. Rarely responds to comfort when distressed; or
c. Episodes of unexplained emotional distress.
AND
B. Extreme limitation of one, or marked limitation of two, of the following areas of mental functioning (see 112.00F):
1. Understand, remember, or apply information (see 112.00E1).
2. Interact with others (see 112.00E2).
3. Concentrate, persist, or maintain pace (see 112.00E3).
4. Adapt or manage oneself (see 112.00E4).
OR
C. Your mental disorder in this listing category is “serious and persistent;” that is, you have a medically documented history of the existence of the disorder over a period of at least 2 years, and there is evidence of both:
1. Medical treatment, mental health therapy, psychosocial support(s), or a highly structured setting(s) that is ongoing and that diminishes the symptoms and signs of your mental disorder (see 112.00G2b); and
2. Marginal adjustment, that is, you have minimal capacity to adapt to changes in your environment or to demands that are not already part of your daily life (see 112.00G2c).
113.00 Cancer (Malignant Neoplastic Diseases)
A. What impairments do these listings cover? We use these listings to evaluate all cancers (malignant neoplastic diseases) except certain cancers associated with human immunodeficiency virus (HIV) infection. We use the criteria in 114.11B to evaluate primary central nervous system lymphoma, 114.11C to evaluate primary effusion lymphoma, and 114.11E to evaluate pulmonary Kaposi sarcoma if you also have HIV infection. We evaluate all other cancers associated with HIV infection, for example, Hodgkin lymphoma or non-pulmonary Kaposi sarcoma, under this body system or under 114.11F-I in the immune system disorders body system.
B. What do we consider when we evaluate cancer under these listings? We will consider factors including:
1. Origin of the cancer.
2. Extent of involvement.
3. Duration, frequency, and response to anticancer therapy.
4. Effects of any post-therapeutic residuals.
C. How do we apply these listings? We apply the criteria in a specific listing to a cancer originating from that specific site.
D. What evidence do we need?
1. We need medical evidence that specifies the type, extent, and site of the primary, recurrent, or metastatic lesion. When the primary site cannot be identified, we will use evidence documenting the site(s) of metastasis to evaluate the impairment under 13.27 in part A.
2. For operative procedures, including a biopsy or a needle aspiration, we generally need a copy of both the:
a. Operative note, and
b. Pathology report.
3. When we cannot get these documents, we will accept the summary of hospitalization(s) or other medical reports. This evidence should include details of the findings at surgery and, whenever appropriate, the pathological findings.
4. In some situations, we may also need evidence about recurrence, persistence, or progression of the cancer, the response to therapy, and any significant residuals. (See 113.00G.)
E. When do we need longitudinal evidence?
1. Cancer with distant metastases. Most cancer of childhood consists of a local lesion with metastases to regional lymph nodes and, less often, distant metastases. We generally do not need longitudinal evidence for cancer that has metastasized beyond the regional lymph nodes because this cancer usually meets the requirements of a listing. Exceptions are for cancer with distant metastases that we expect to respond to anticancer therapy. For these exceptions, we usually need a longitudinal record of 3 months after therapy starts to determine whether the therapy achieved its intended effect, and whether this effect is likely to persist.
2. Other cancers. When there are no distant metastases, many of the listings require that we consider your response to initial anticancer therapy; that is, the initial planned treatment regimen. This therapy may consist of a single modality or a combination of modalities; that is, multimodal therapy (see 113.00I3).
3. Types of treatment.
a. Whenever the initial planned therapy is a single modality, enough time must pass to allow a determination about whether the therapy will achieve its intended effect. If the treatment fails, the failure often happens within 6 months after treatment starts, and there will often be a change in the treatment regimen.
b. Whenever the initial planned therapy is multimodal, we usually cannot make a determination about the effectiveness of the therapy until we can determine the effects of all the planned modalities. In some cases, we may need to defer adjudication until we can assess the effectiveness of therapy. However, we do not need to defer adjudication to determine whether the therapy will achieve its intended effect if we can make a fully favorable determination or decision based on the length and effects of therapy, or the residuals of the cancer or therapy (see 113.00G).
F. How do we evaluate impairments that do not meet one of the cancer listings?
1. These listings are only examples of cancers that we consider severe enough to result in marked and severe functional limitations. If your severe impairment(s) does not meet the criteria of any of these listings, we must also consider whether you have an impairment(s) that meets the criteria of a listing in another body system.
2. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. (See §§ 404.1526 and 416.926 of this chapter.) If your impairment(s) does not meet or medically equal a listing, we will also consider whether you have an impairment(s) that functionally equals the listings. (See § 416.926a of this chapter.) We use the rules in § 416.994a of this chapter when we decide whether you continue to be disabled.
G. How do we consider the effects of anticancer therapy?
1. How we consider the effects of anticancer therapy under the listings. In many cases, cancers meet listing criteria only if the therapy is not effective and the cancer persists, progresses, or recurs. However, as explained in the following paragraphs, we will not delay adjudication if we can make a fully favorable determination or decision based on the evidence in the case record.
2. Effects can vary widely.
a. We consider each case on an individual basis because the therapy and its toxicity may vary widely. We will request a specific description of the therapy, including these items:
i. Drugs given.
ii. Dosage.
iii. Frequency of drug administration.
iv. Plans for continued drug administration.
v. Extent of surgery.
vi. Schedule and fields of radiation therapy.
b. We will also request a description of the complications or adverse effects of therapy, such as the following:
i. Continuing gastrointestinal symptoms.
ii. Persistent weakness.
iii. Neurological complications.
iv. Cardiovascular complications.
v. Reactive mental disorders.
3. Effects of therapy may change. The severity of the adverse effects of anticancer therapy may change during treatment; therefore, enough time must pass to allow us to evaluate the therapy's effect. The residual effects of treatment are temporary in most instances; however, on occasion, the effects may be disabling for a consecutive period of at least 12 months. In some situations, very serious adverse effects may interrupt and prolong multimodal anticancer therapy for a continuous period of almost 12 months. In these situations, we may determine there is an expectation that your impairment will preclude you from engaging in any age-appropriate activities for at least 12 months.
4. When the initial anticancer therapy is effective. We evaluate any post-therapeutic residual impairment(s) not included in these listings under the criteria for the affected body system. We must consider any complications of therapy. When the residual impairment(s) does not meet a listing, we must consider whether it medically equals a listing, or, as appropriate, functionally equals the listings.
H. How long do we consider your impairment to be disabling?
1. In some listings, we specify that we will consider your impairment to be disabling until a particular point in time (for example, until at least 12 months from the date of transplantation). We may consider your impairment to be disabling beyond this point when the medical and other evidence justifies it.
2. When a listing does not contain such a specification, we will consider an impairment(s) that meets or medically equals a listing in this body system to be disabling until at least 3 years after onset of complete remission. When the impairment(s) has been in complete remission for at least 3 years, that is, the original tumor or a recurrence (or relapse) and any metastases have not been evident for at least 3 years, the impairment(s) will no longer meet or medically equal the criteria of a listing in this body system.
3. Following the appropriate period, we will consider any residuals, including residuals of the cancer or therapy (see 113.00G), in determining whether you are disabled. If you have a recurrence or relapse of your cancer, your impairment may meet or medically equal one of the listings in this body system again.
I. What do we mean by the following terms?
1. Anticancer therapy means surgery, radiation, chemotherapy, hormones, immunotherapy, or bone marrow or stem cell transplantation. When we refer to surgery as an anticancer treatment, we mean surgical excision for treatment, not for diagnostic purposes.
2. Metastases means the spread of cancer cells by blood, lymph, or other body fluid. This term does not include the spread of cancer cells by direct extension of the cancer to other tissues or organs.
3. Multimodal therapy means anticancer therapy that is a combination of at least two types of treatment given in close proximity as a unified whole and usually planned before any treatment has begun. There are three types of treatment modalities: Surgery, radiation, and systemic drug therapy (chemotherapy, hormone therapy, and immunotherapy or biological modifier therapy). Examples of multimodal therapy include:
a. Surgery followed by chemotherapy or radiation.
b. Chemotherapy followed by surgery.
c. Chemotherapy and concurrent radiation.
4. Persistent means the planned initial anticancer therapy failed to achieve a complete remission of your cancer; that is, your cancer is evident, even if smaller, after the therapy has ended.
5. Progressive means the cancer becomes more extensive after treatment; that is, there is evidence that your cancer is growing after you have completed at least half of your planned initial anticancer therapy.
6. Recurrent or relapse means the cancer that was in complete remission or entirely removed by surgery has returned.
J. Can we establish the existence of a disabling impairment prior to the date of the evidence that shows the cancer satisfies the criteria of a listing? Yes. We will consider factors such as:
1. The type of cancer and its location.
2. The extent of involvement when the cancer was first demonstrated.
3. Your symptoms.
K. How do we evaluate specific cancers?
1. Lymphoma.
a. We provide criteria for evaluating lymphomas that are disseminated or have not responded to anticancer therapy in 113.05.
b. Lymphoblastic lymphoma is treated with leukemia-based protocols, so we evaluate this type of cancer under 113.06.
2. Leukemia.
a. Acute leukemia. The initial diagnosis of acute leukemia, including the accelerated or blast phase of chronic myelogenous (granulocytic) leukemia, is based on definitive bone marrow examination. Additional diagnostic information is based on chromosomal analysis, cytochemical and surface marker studies on the abnormal cells, or other methods consistent with the prevailing state of medical knowledge and clinical practice. Recurrent disease must be documented by peripheral blood, bone marrow, or cerebrospinal fluid examination, or by testicular biopsy. The initial and follow-up pathology reports should be included.
b. Chronic myelogenous leukemia (CML). We need a diagnosis of CML based on documented granulocytosis, including immature forms such as differentiated or undifferentiated myelocytes and myeloblasts, and a chromosomal analysis that demonstrates the Philadelphia chromosome. In the absence of a chromosomal analysis, or if the Philadelphia chromosome is not present, the diagnosis may be made by other methods consistent with the prevailing state of medical knowledge and clinical practice. The requirement for CML in the accelerated or blast phase is met in 113.06B if laboratory findings show the proportion of blast (immature) cells in the peripheral blood or bone marrow is 10 percent or greater.
c. Juvenile chronic myelogenous leukemia (JCML). JCML is a rare, Philadelphia-chromosome-negative childhood leukemia that is aggressive and clinically similar to acute myelogenous leukemia. We evaluate JCML under 113.06A.
d. Elevated white cell count. In cases of chronic leukemia (either myelogenous or lymphocytic), an elevated white cell count, in itself, is not a factor in determining the severity of the impairment.
3. Malignant solid tumors. The tumors we consider under 113.03 include the histiocytosis syndromes except for solitary eosinophilic granuloma. We do not evaluate thyroid cancer (see 113.09), retinoblastomas (see 113.12), primary central nervous system (CNS) cancers (see 113.13), neuroblastomas (see 113.21), or malignant melanoma (see 113.29) under this listing.
4. Primary central nervous system (CNS) cancers. We use the criteria in 113.13 to evaluate cancers that originate within the CNS (that is, brain and spinal cord cancers).
a. The CNS cancers listed in 113.13A are highly malignant and respond poorly to treatment, and therefore we do not require additional criteria to evaluate them. We do not list pituitary gland cancer (for example, pituitary gland carcinoma) in 113.13A, although this CNS cancer is highly malignant and responds poorly to treatment. We evaluate pituitary gland cancer under 113.13A and do not require additional criteria to evaluate it.
b. We consider a CNS tumor to be malignant if it is classified as Grade II, Grade III, or Grade IV under the World Health Organization (WHO) classification of tumors of the CNS (WHO Classification of Tumours of the Central Nervous System, 2007).
c. We evaluate benign (for example, WHO Grade I) CNS tumors under 111.05. We evaluate metastasized CNS cancers from non-CNS sites under the primary cancers (see 113.00C). We evaluate any complications of CNS cancers, such as resultant neurological or psychological impairments, under the criteria for the affected body system.
5. Retinoblastoma. The treatment for bilateral retinoblastoma usually results in a visual impairment. We will evaluate any resulting visual impairment under 102.02.
6. Melanoma. We evaluate malignant melanoma that affects the skin (cutaneous melanoma), eye (ocular melanoma), or mucosal membranes (mucosal melanoma) under 113.29. We evaluate melanoma that is not malignant that affects the skin (benign melanocytic tumor) under the listings in 108.00 or other affected body systems.
L. How do we evaluate cancer treated by bone marrow or stem cell transplantation, including transplantation using stem cells from umbilical cord blood? Bone marrow or stem cell transplantation is performed for a variety of cancers. We require the transplantation to occur before we evaluate it under these listings. We do not need to restrict our determination of the onset of disability to the date of transplantation (113.05 or 113.06). We may be able to establish an earlier onset date of disability due to your transplantation if the evidence in your case record supports such a finding.
1. Acute leukemia (including all types of lymphoblastic lymphomas and JCML) or accelerated or blast phase of CML. If you undergo bone marrow or stem cell transplantation for any of these disorders, we will consider you to be disabled until at least 24 months from the date of diagnosis or relapse, or at least 12 months from the date of transplantation, whichever is later.
2. Lymphoma or chronic phase of CML. If you undergo bone marrow or stem cell transplantation for any of these disorders, we will consider you to be disabled until at least 12 months from the date of transplantation.
3. Evaluating disability after the appropriate time period has elapsed. We consider any residual impairment(s), such as complications arising from:
a. Graft-versus-host (GVH) disease.
b. Immunosuppressant therapy, such as frequent infections.
c. Significant deterioration of other organ systems.
113.01 Category of Impairments, Cancer (Malignant Neoplastic Diseases)
113.01 Category of Impairments, Malignant Neoplastic Diseases
113.03 Malignant solid tumors. Consider under a disability:
A. For 24 months from the date of initial diagnosis. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
OR
B. For 24 months from the date of recurrence of active disease. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
113.05 Lymphoma (excluding all types of lymphoblastic lymphomas - 113.06). (See 113.00K1.)
A. Non-Hodgkin lymphoma (including Burkitt's and anaplastic large cell), with either 1 or 2:
1. Bone marrow, brain, spinal cord, liver, or lung involvement at initial diagnosis. Consider under a disability for 24 months from the date of diagnosis. Thereafter, evaluate under 113.05A2, or any residual impairments(s) under the criteria for the affected body system.
2. Persistent or recurrent following initial anticancer therapy.
OR
B. Hodgkin lymphoma, with either 1 or 2:
1. Bone marrow, brain, spinal cord, liver, or lung involvement at initial diagnosis. Consider under a disability for 24 months from the date of diagnosis. Thereafter, evaluate under 113.05B2, or any residual impairment(s) under the criteria for the affected body system.
2. Persistent or recurrent following initial anticancer therapy.
OR
C. With bone marrow or stem cell transplantation. Consider under a disability until at least 12 months from the date of transplantation. Thereafter, evaluate any residual impairment(s) under the criteria of the affected body system.
OR
D. Mantle cell lymphoma.
113.06 Leukemia. (See 113.00K2.)
A. Acute leukemia (including all types of lymphoblastic lymphomas and juvenile chronic myelogenous leukemia (JCML)). Consider under a disability until at least 24 months from the date of diagnosis or relapse, or at least 12 months from the date of bone marrow or stem cell transplantation, whichever is later. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
OR
B. Chronic myelogenous leukemia (except JCML), as described in 1 or 2:
1. Accelerated or blast phase (see 113.00K2b). Consider under a disability until at least 24 months from the date of diagnosis or relapse, or at least 12 months from the date of bone marrow or stem cell transplantation, whichever is later. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
2. Chronic phase, as described in a or b:
a. Consider under a disability until at least 12 months from the date of bone marrow or stem cell transplantation. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
b. Progressive disease following initial antineoplastic therapy.
113.09 Thyroid gland.
A. Anaplastic (undifferentiated) carcinoma.
OR
B. Carcinoma with metastases beyond the regional lymph nodes progressive despite radioactive iodine therapy.
OR
C. Medullary carcinoma with metastases beyond the regional lymph nodes.
113.12 Retinoblastoma.
A. With extension beyond the orbit.
OR
B. Persistent or recurrent following initial anticancer therapy.
OR
C. With regional or distant metastases.
113.13 Nervous system. (See 113.00K4.) Primary central nervous system (CNS; that is, brain and spinal cord) cancers, as described in A, B, or C:
A. Glioblastoma multiforme, ependymoblastoma, and diffuse intrinsic brain stem gliomas (see 113.00K4a).
B. Any Grade III or Grade IV CNS cancer (see 113.00K4b), including astrocytomas, sarcomas, and medulloblastoma and other primitive neuroectodermal tumors (PNETs).
C. Any primary CNS cancer, as described in 1 or 2:
1. Metastatic.
2. Progressive or recurrent following initial anticancer therapy.
113.21 Neuroblastoma.
A. With extension across the midline.
OR
B. With distant metastases.
OR
C. Recurrent.
OR
D. With onset at age 1 year or older.
113.29 Malignant melanoma (including skin, ocular, or mucosal melanomas), as described in either A, B, or C:
A. Recurrent (except an additional primary melanoma at a different site, which is not considered to be recurrent disease) following either 1 or 2:
1. Wide excision (skin melanoma).
2. Enucleation of the eye (ocular melanoma).
OR
B. With metastases as described in 1, 2, or 3:
1. Metastases to one or more clinically apparent nodes; that is, nodes that are detected by imaging studies (excluding lymphoscintigraphy) or by clinical evaluation (palpable).
2. If the nodes are not clinically apparent, with metastases to four or more nodes.
3. Metastases to adjacent skin (satellite lesions) or distant sites (for example, liver, lung, or brain).
OR
C. Mucosal melanoma.
114.00 Immune System Disorders
A. What disorders do we evaluate under the immune system disorders listings?
1. We evaluate immune system disorders that cause dysfunction in one or more components of your immune system.
a. The dysfunction may be due to problems in antibody production, impaired cell-mediated immunity, a combined type of antibody/cellular deficiency, impaired phagocytosis, or complement deficiency.
b. Immune system disorders may result in recurrent and unusual infections, or inflammation and dysfunction of the body's own tissues. Immune system disorders can cause a deficit in a single organ or body system that results in extreme (that is, very serious) loss of function. They can also cause lesser degrees of limitations in two or more organs or body systems, and when associated with symptoms or signs, such as severe fatigue, fever, malaise, diffuse musculoskeletal pain, or involuntary weight loss, can also result in extreme limitation. In children, immune system disorders or their treatment may also affect growth, development, and the performance of age-appropriate activities.
c. We organize the discussions of immune system disorders in three categories: Autoimmune disorders; Immune deficiency disorders, excluding human immunodeficiency virus (HIV) infection; and HIV infection.
2. Autoimmune disorders (114.00D). Autoimmune disorders are caused by dysfunctional immune responses directed against the body's own tissues, resulting in chronic, multisystem impairments that differ in clinical manifestations, course, and outcome. They are sometimes referred to as rheumatic diseases, connective tissue disorders, or collagen vascular disorders. Some of the features of autoimmune disorders in children differ from the features of the same disorders in adults. The impact of the disorders or their treatment on physical, psychological, and developmental growth of pre-pubertal children may be considerable, and often differs from that of post-pubertal adolescents or adults.
3. Immune deficiency disorders, excluding HIV infection (114.00E). Immune deficiency disorders are characterized by recurrent or unusual infections that respond poorly to treatment, and are often associated with complications affecting other parts of the body. Immune deficiency disorders are classified as either primary (congenital) or acquired. Children with immune deficiency disorders also have an increased risk of malignancies and of having autoimmune disorders.
4. Human immunodeficiency virus (HIV) infection (114.00F). HIV infection may be characterized by increased susceptibility to common infections as well as opportunistic infections, cancers, or other conditions listed in 114.11.
B. What information do we need to show that you have an immune system disorder?
Generally, we need your medical history, a report(s) of a physical examination, a report(s) of laboratory findings, and in some instances, appropriate medically acceptable imaging or tissue biopsy reports to show that you have an immune system disorder. Therefore, we will make every reasonable effort to obtain your medical history, medical findings, and results of laboratory tests. We explain the information we need in more detail in the sections below.
C. Definitions
1. Appropriate medically acceptable imaging includes, but is not limited to, angiography, x-ray imaging, computerized axial tomography (CAT scan) or magnetic resonance imaging (MRI), with or without contrast material, myelography, and radionuclear bone scans. “Appropriate” means that the technique used is the proper one to support the evaluation and diagnosis of the impairment.
2. Constitutional symptoms or signs, as used in these listings, means severe fatigue, fever, malaise, or involuntary weight loss. Severe fatigue means a frequent sense of exhaustion that results in significantly reduced physical activity or mental function. Malaise means frequent feelings of illness, bodily discomfort, or lack of well-being that result in significantly reduced physical activity or mental function.
3. Disseminated means that a condition is spread over a considerable area. The type and extent of the spread will depend on your specific disease.
4. Dysfunction means that one or more of the body regulatory mechanisms are impaired, causing either an excess or deficiency of immunocompetent cells or their products.
5. Extra-articular means “other than the joints”; for example, an organ(s) such as the heart, lungs, kidneys, or skin.
6. Documented medical need has the same meaning as in 101.00C6a.
7. Fine and gross movements has the same meaning as in 101.00E4.
8. Major joint of an upper or a lower extremity has the same meaning as in 101.00I2 and 101.00I3.
9. Persistent means that a sign(s) or symptom(s) has continued over time. The precise meaning will depend on the specific immune system disorder, the usual course of the disorder, and the other circumstances of your clinical course.
10. Recurrent means that a condition that previously responded adequately to an appropriate course of treatment returns after a period of remission or regression. The precise meaning, such as the extent of response or remission and the time periods involved, will depend on the specific disease or condition you have, the body system affected, the usual course of the disorder and its treatment, and the other facts of your particular case.
11. Resistant to treatment means that a condition did not respond adequately to an appropriate course of treatment. Whether a response is adequate or a course of treatment is appropriate will depend on the specific disease or condition you have, the body system affected, the usual course of the disorder and its treatment, and the other facts of your particular case.
12. Severe means medical severity as used by the medical community. The term does not have the same meaning as it does when we use it in connection with a finding at the second step of the sequential evaluation process in § 416.920 of this chapter.
D. How do we document and evaluate the listed autoimmune disorders?
1. Systemic lupus erythematosus (114.02).
a. General. Systemic lupus erythematosus (SLE) is a chronic inflammatory disease that can affect any organ or body system. It is frequently, but not always, accompanied by constitutional symptoms or signs (severe fatigue, fever, malaise, involuntary weight loss). Major organ or body system involvement can include: Respiratory (pleuritis, pneumonitis), cardiovascular (endocarditis, myocarditis, pericarditis, vasculitis), renal (glomerulonephritis), hematologic (anemia, leukopenia, thrombocytopenia), skin (photosensitivity), neurologic (seizures), mental (anxiety, fluctuating cognition (“lupus fog”), mood disorders, organic brain syndrome, psychosis), or immune system disorders (inflammatory arthritis). Immunologically, there is an array of circulating serum auto-antibodies and pro- and anti-coagulant proteins that may occur in a highly variable pattern.
b. Documentation of SLE. Generally, but not always, the medical evidence will show that your SLE satisfies the criteria in the current “Criteria for the Classification of Systemic Lupus Erythematosus” by the American College of Rheumatology found in the most recent edition of the Primer on the Rheumatic Diseases published by the Arthritis Foundation.
2. Systemic vasculitis (114.03).
a. General.
(i) Vasculitis is an inflammation of blood vessels. It may occur acutely in association with adverse drug reactions, certain chronic infections, and occasionally, malignancies. More often, it is chronic and the cause is unknown. Symptoms vary depending on which blood vessels are involved. Systemic vasculitis may also be associated with other autoimmune disorders; for example, SLE or dermatomyositis.
(ii) Children can develop the vasculitis of Kawasaki disease, of which the most serious manifestation is formation of coronary artery aneurysms and related complications. We evaluate heart problems related to Kawasaki disease under the criteria in the cardiovascular listings (104.00). Children can also develop the vasculitis of anaphylactoid purpura (Henoch-Schoenlein purpura), which may cause intestinal and renal disorders. We evaluate intestinal and renal disorders related to vasculitis of anaphylactoid purpura under the criteria in the digestive (105.00) or genitourinary (106.00) listings. Other clinical patterns include, but are not limited to, polyarteritis nodosa, Takayasu's arteritis (aortic arch arteritis), and Wegener's granulomatosis.
b. Documentation of systemic vasculitis. Angiography or tissue biopsy confirms a diagnosis of systemic vasculitis when the disease is suspected clinically. When you have had angiography or tissue biopsy for systemic vasculitis, we will make every reasonable effort to obtain reports of the results of that procedure. However, we will not purchase angiography or tissue biopsy.
3. Systemic sclerosis (scleroderma) (114.04).
a. General. Systemic sclerosis (scleroderma) constitutes a spectrum of disease in which thickening of the skin is the clinical hallmark. Raynaud's phenomenon, often medically severe and progressive, is present frequently and may be the peripheral manifestation of a vasospastic abnormality in the heart, lungs, and kidneys. The CREST syndrome (calcinosis, Raynaud's phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia) is a variant that may slowly progress over years to the generalized process, systemic sclerosis.
b. Diffuse cutaneous systemic sclerosis. In diffuse cutaneous systemic sclerosis (also known as diffuse scleroderma), major organ or systemic involvement can include the gastrointestinal tract, lungs, heart, kidneys, and muscle in addition to skin or blood vessels. Although arthritis can occur, joint dysfunction results primarily from soft tissue/cutaneous thickening, fibrosis, and contractures.
c. Localized scleroderma (linear scleroderma and morphea).
(i) Localized scleroderma (linear scleroderma and morphea) is more common in children than systemic scleroderma. To assess the severity of the impairment, we need a description of the extent of involvement of linear scleroderma and the location of the lesions. For example, linear scleroderma involving the arm but not crossing any joints is not as functionally limiting as sclerodactyly (scleroderma localized to the fingers). Linear scleroderma of a lower extremity involving skin thickening and atrophy of underlying muscle or bone can result in contractures and leg length discrepancy. In such cases, we may evaluate your impairment under the musculoskeletal listings (101.00).
(ii) When there is isolated morphea of the face causing facial disfigurement from unilateral hypoplasia of the mandible, maxilla, zygoma, or orbit, adjudication may be more appropriate under the criteria in the affected body system, such as special senses and speech (102.00) or mental disorders (112.00).
(iii) Chronic variants of these syndromes include disseminated morphea, Shulman's disease (diffuse fasciitis with eosinophilia), and eosinophilia-myalgia syndrome (often associated with toxins such as toxic oil or contaminated tryptophan), all of which can impose medically severe musculoskeletal dysfunction and may also lead to restrictive pulmonary disease. We evaluate these variants of the disease under the criteria in the musculoskeletal listings (101.00) or respiratory system listings (103.00).
d. Documentation of systemic sclerosis (scleroderma). Documentation involves differentiating the clinical features of systemic sclerosis (scleroderma) from other autoimmune disorders. However, there may be an overlap.
4. Polymyositis and dermatomyositis (114.05).
a. General.
(i) Polymyositis and dermatomyositis are related disorders that are characterized by an inflammatory process in striated muscle, occurring alone or in association with other autoimmune disorders. The most common manifestations are symmetric weakness, and less frequently, pain and tenderness of the proximal limb-girdle (shoulder or pelvic) musculature. There may also be involvement of the cervical, cricopharyngeal, esophageal, intercostal, and diaphragmatic muscles.
(ii) Polymyositis occurs rarely in children; the more common presentation in children is dermatomyositis with symmetric proximal muscle weakness and characteristic skin findings. The clinical course of dermatomyositis can be more severe when it is accompanied by systemic vasculitis rather than just localized to striated muscle. Late in the disease, some children with dermatomyositis develop calcinosis of the skin and subcutaneous tissues, muscles, and joints. We evaluate the involvement of other organs/body systems under the criteria for the listings in the affected body system.
b. Documentation of polymyositis and dermatomyositis. Generally, but not always, polymyositis is associated with elevated serum muscle enzymes (creatine phosphokinase (CPK), aminotransferases, and aldolase), and characteristic abnormalities on electromyography and muscle biopsy. In children, the diagnosis of dermatomyositis is supported largely by medical history, findings on physical examination that include the characteristic skin findings, and elevated serum muscle enzymes. Muscle inflammation or vasculitis depicted on MRI is additional evidence supporting the diagnosis of childhood dermatomyositis. When you have had electromyography, muscle biopsy, or MRI for polymyositis or dermatomyositis, we will make every reasonable effort to obtain reports of the results of that procedure. However, we will not purchase electromyography, muscle biopsy, or MRI.
c. Additional information about how we evaluate polymyositis and dermatomyositis under the listings.
(i) In newborn and younger infants (birth to attainment of age 1), we consider muscle weakness that affects motor skills, such as head control, reaching, grasping, taking solids, or self-feeding, under 114.05A. In older infants and toddlers (age 1 to attainment of age 3), we also consider muscle weakness affecting your ability to roll over, sit, crawl, or walk under 114.05A.
(ii) If you are of preschool age through adolescence (age 3 to attainment of age 18), weakness of your pelvic girdle muscles that results in your inability to rise independently from a squatting or sitting position or to climb stairs may be an indication that you are unable to walk without assistance. Weakness of your shoulder girdle muscles may result in your inability to perform lifting, carrying, and reaching overhead, and also may seriously affect your ability to perform activities requiring fine movements. We evaluate these limitations under 114.05A.
5. Undifferentiated and mixed connective tissue disease (114.06).
a. General. This listing includes syndromes with clinical and immunologic features of several autoimmune disorders, but which do not satisfy the criteria for any of the specific disorders described. For example, you may have clinical features of SLE and systemic vasculitis, and the serologic (blood test) findings of rheumatoid arthritis. The most common pattern of undifferentiated autoimmune disorders in children is mixed connective tissue disease (MCTD).
b. Documentation of undifferentiated and mixed connective tissue disease. Undifferentiated connective tissue disease is diagnosed when clinical features and serologic (blood test) findings, such as rheumatoid factor or antinuclear antibody (consistent with an autoimmune disorder) are present but do not satisfy the criteria for a specific disease. Children with MCTD have laboratory findings of extremely high antibody titers to extractable nuclear antigen (ENA) or ribonucleoprotein (RNP) without high titers of anti-dsDNA or anti-SM antibodies. There are often clinical findings suggestive of SLE or childhood dermatomyositis. Many children later develop features of scleroderma.
6. Inflammatory arthritis (114.09).
a. General. The spectrum of inflammatory arthritis includes a vast array of disorders that differ in cause, course, and outcome. Clinically, inflammation of major joints in an upper or a lower extremity may be the dominant manifestation causing difficulties with walking or fine and gross movements; there may be joint pain, swelling, and tenderness. The arthritis may affect other joints, or cause less limitation in walking or fine and gross movements. However, in combination with extra-articular features, including constitutional symptoms or signs (severe fatigue, fever, malaise, and involuntary weight loss), inflammatory arthritis may result in an extreme limitation.
b. Inflammatory arthritis involving the axial spine (spondyloarthropathy). In children, inflammatory arthritis involving the axial spine may be associated with disorders such as:
(i) Reactive arthropathies;
(ii) Juvenile ankylosing spondylitis;
(iii) Psoriatic arthritis;
(iv) SEA syndrome (seronegative enthesopathy arthropathy syndrome);
(v) Behçet's disease; and
(vi) Inflammatory bowel disease.
c. Inflammatory arthritis involving the peripheral joints. In children, inflammatory arthritis involving peripheral joints may be associated with disorders such as:
(i) Juvenile rheumatoid arthritis;
(ii) Sjöogren's syndrome;
(iii) Psoriatic arthritis;
(iv) Crystal deposition disorders (gout and pseudogout);
(v) Lyme disease; and
(vi) Inflammatory bowel disease.
d. Documentation of inflammatory arthritis. Generally, but not always, the diagnosis of inflammatory arthritis is based on the clinical features and serologic findings described in the most recent edition of the Primer on the Rheumatic Diseases published by the Arthritis Foundation.
e. How we evaluate inflammatory arthritis under the listings.
(i) Listing-level severity in 114.09A and 114.09C1 is shown by the presence of an impairment-related physical limitation of functioning. In 114.09C1, if you have the required ankylosis (fixation) of your cervical or dorsolumbar spine, we will find that you have a listing-level impairment-related physical limitation in your ability to see in front of you, above you, and to the side, even though you might not require bilateral upper limb assistance.
(ii) Listing-level severity in 114.09B and 114.09C2 is shown by inflammatory arthritis that involves various combinations of complications (such as inflammation or deformity, extra-articular features, repeated manifestations, and constitutional symptoms and signs) of one or more major joints in an upper or a lower extremity (see 114.00C8) or other joints. Extra-articular impairments may also meet listings in other body systems.
(iii) Extra-articular features of inflammatory arthritis may involve any body system; for example: Musculoskeletal (heel enthesopathy), ophthalmologic (iridocyclitis, keratoconjunctivitis sicca, uveitis), pulmonary (pleuritis, pulmonary fibrosis or nodules, restrictive lung disease), cardiovascular (aortic valve insufficiency, arrhythmias, coronary arteritis, myocarditis, pericarditis, Raynaud's phenomenon, systemic vasculitis), renal (amyloidosis of the kidney), hematologic (chronic anemia, thrombocytopenia), neurologic (peripheral neuropathy, radiculopathy, spinal cord or cauda equina compression with sensory and motor loss), mental (cognitive dysfunction, poor memory), and immune system (Felty's syndrome (hypersplenism with compromised immune competence)).
(iv) If both inflammation and chronic deformities are present, we evaluate your impairment under the criteria of any appropriate listing.
7. Sjögren's syndrome (114.10).
a. General.
(i) Sjögren's syndrome is an immune-mediated disorder of the exocrine glands. Involvement of the lacrimal and salivary glands is the hallmark feature, resulting in symptoms of dry eyes and dry mouth, and possible complications, such as corneal damage, blepharitis (eyelid inflammation), dysphagia (difficulty in swallowing), dental caries, and the inability to speak for extended periods of time. Involvement of the exocrine glands of the upper airways may result in persistent dry cough.
(ii) Many other organ systems may be involved, including musculoskeletal (arthritis, myositis), respiratory (interstitial fibrosis), gastrointestinal (dysmotility, dysphagia, involuntary weight loss), genitourinary (interstitial cystitis, renal tubular acidosis), skin (purpura, vasculitis,), neurologic (central nervous system disorders, cranial and peripheral neuropathies), mental (cognitive dysfunction, poor memory), and neoplastic (lymphoma). Severe fatigue and malaise are frequently reported. Sjögren's syndrome may be associated with other autoimmune disorders (for example, rheumatoid arthritis or SLE); usually the clinical features of the associated disorder predominate.
b. Documentation of Sjögren's syndrome. If you have Sjögren's syndrome, the medical evidence will generally, but not always, show that your disease satisfies the criteria in the current “Criteria for the Classification of Sjögren's Syndrome” by the American College of Rheumatology found in the most recent edition of the Primer on the Rheumatic Diseases published by the Arthritis Foundation.
E. How do we document and evaluate immune deficiency disorders, excluding HIV infection?
1. General.
a. Immune deficiency disorders can be classified as:
(i) Primary (congenital); for example, X-linked agammaglobulinemia, thymic hypoplasia (DiGeorge syndrome), severe combined immunodeficiency (SCID), chronic granulomatous disease (CGD), C1 esterase inhibitor deficiency.
(ii) Acquired; for example, medication-related.
b. Primary immune deficiency disorders are seen mainly in children. However, recent advances in the treatment of these disorders have allowed many affected children to survive well into adulthood. Occasionally, these disorders are first diagnosed in adolescence or adulthood.
2. Documentation of immune deficiency disorders. The medical evidence must include documentation of the specific type of immune deficiency. Documentation may be by laboratory evidence or by other generally acceptable methods consistent with the prevailing state of medical knowledge and clinical practice.
3. Immune deficiency disorders treated by stem cell transplantation.
a. Evaluation in the first 12 months. If you undergo stem cell transplantation for your immune deficiency disorder, we will consider you disabled until at least 12 months from the date of the transplant.
b. Evaluation after the 12-month period has elapsed. After the 12-month period has elapsed, we will consider any residuals of your immune deficiency disorder as well as any residual impairment(s) resulting from the treatment, such as complications arising from:
(i) Graft-versus-host (GVH) disease.
(ii) Immunosuppressant therapy, such as frequent infections.
(iii) Significant deterioration of other organ systems.
4. Medication-induced immune suppression. Medication effects can result in varying degrees of immune suppression, but most resolve when the medication is ceased. However, if you are prescribed medication for long-term immune suppression, such as after an organ transplant, we will evaluate:
a. The frequency and severity of infections.
b. Residuals from the organ transplant itself, after the 12-month period has elapsed.
c. Significant deterioration of other organ systems.
F. How do we document and evaluate HIV infection? Any child with HIV infection, including one with a diagnosis of acquired immune deficiency syndrome (AIDS), may be found disabled under 114.11 if his or her impairment meets the criteria in that listing or is medically equivalent to the criteria in that listing.
1. Documentation of HIV infection.
a. Definitive documentation of HIV infection. We may document a diagnosis of HIV infection by positive findings on one or more of the following definitive laboratory tests:
(i) HIV antibody screening test (for example, enzyme immunoassay, or EIA), confirmed by a supplemental HIV antibody test such as the Western blot (immunoblot) or immunofluorescence assay, for any child age 18 months or older.
(ii) HIV nucleic acid (DNA or RNA) detection test (for example, polymerase chain reaction, or PCR).
(iii) HIV p24 antigen (p24Ag) test, for any child age 1 month or older.
(iv) Isolation of HIV in viral culture.
(v) Other tests that are highly specific for detection of HIV and that are consistent with the prevailing state of medical knowledge.
b. We will make every reasonable effort to obtain the results of your laboratory testing. Pursuant to § 416.919f of this chapter, we will purchase examinations or tests necessary to make a determination in your claim if no other acceptable documentation exists.
c. Other acceptable documentation of HIV infection. We may also document HIV infection without definitive laboratory evidence.
(i) We will accept a persuasive report from a physician that a positive diagnosis of your HIV infection was confirmed by an appropriate laboratory test(s), such as those described in 114.00F1a. To be persuasive, this report must state that you had the appropriate definitive laboratory test(s) for diagnosing your HIV infection and provide the results. The report must also be consistent with the remaining evidence of record.
(ii) We may also document HIV infection by the medical history, clinical and laboratory findings, and diagnosis(es) indicated in the medical evidence, provided that such documentation is consistent with the prevailing state of medical knowledge and clinical practice and is consistent with the other evidence in your case record. For example, we will accept a diagnosis of HIV infection without definitive laboratory evidence of the HIV infection if you have an opportunistic disease that is predictive of a defect in cell-mediated immunity (for example, toxoplasmosis of the brain or Pneumocystis pneumonia (PCP)), and there is no other known cause of diminished resistance to that disease (for example, long-term steroid treatment or lymphoma). In such cases, we will make every reasonable effort to obtain full details of the history, medical findings, and results of testing.
2. Documentation of the manifestations of HIV infection.
a. Definitive documentation of manifestations of HIV infection. We may document manifestations of HIV infection by positive findings on definitive laboratory tests, such as culture, microscopic examination of biopsied tissue or other material (for example, bronchial washings), serologic tests, or on other generally acceptable definitive tests consistent with the prevailing state of medical knowledge and clinical practice.
b. We will make every reasonable effort to obtain the results of your laboratory testing. Pursuant to § 416.919f of this chapter, we will purchase examinations or tests necessary to make a determination of your claim if no other acceptable documentation exists.
c. Other acceptable documentation of manifestations of HIV infection. We may also document manifestations of HIV infection without definitive laboratory evidence.
(i) We will accept a persuasive report from a physician that a positive diagnosis of your manifestation of HIV infection was confirmed by an appropriate laboratory test(s). To be persuasive, this report must state that you had the appropriate definitive laboratory test(s) for diagnosing your manifestation of HIV infection and provide the results. The report must also be consistent with the remaining evidence of record.
(ii) We may also document manifestations of HIV infection without the definitive laboratory evidence described in 114.00F2a, provided that such documentation is consistent with the prevailing state of medical knowledge and clinical practice and is consistent with the other evidence in your case record. For example, many conditions are now commonly diagnosed based on some or all of the following: Medical history, clinical manifestations, laboratory findings (including appropriate medically acceptable imaging), and treatment responses. In such cases, we will make every reasonable effort to obtain full details of the history, medical findings, and results of testing.
3. Disorders associated with HIV infection (114.11A-E).
a. Multicentric Castleman disease (MCD, 114.11A) affects multiple groups of lymph nodes and organs containing lymphoid tissue. This widespread involvement distinguishes MCD from localized (or unicentric) Castleman disease, which affects only a single set of lymph nodes. While not a cancer, MCD is known as a lymphoproliferative disorder. Its clinical presentation and progression is similar to that of lymphoma, and its treatment may include radiation or chemotherapy. We require characteristic findings on microscopic examination of the biopsied lymph nodes or other generally acceptable methods consistent with the prevailing state of medical knowledge and clinical practice to establish the diagnosis. Localized (or unicentric) Castleman disease does not meet or medically equal the criterion in 114.11A, but we may evaluate it under the criteria in 114.11G or 14.11I in part A.
b. Primary central nervous system lymphoma (PCNSL, 114.11B) originates in the brain, spinal cord, meninges, or eye. Imaging tests (for example, MRI) of the brain, while not diagnostic, may show a single lesion or multiple lesions in the white matter of the brain. We require characteristic findings on microscopic examination of the cerebral spinal fluid or of the biopsied brain tissue, or other generally acceptable methods consistent with the prevailing state of medical knowledge and clinical practice to establish the diagnosis.
c. Primary effusion lymphoma (PEL, 114.11C) is also known as body cavity lymphoma. We require characteristic findings on microscopic examination of the effusion fluid or of the biopsied tissue from the affected internal organ, or other generally acceptable methods consistent with the prevailing state of medical knowledge and clinical practice to establish the diagnosis.
d. Progressive multifocal leukoencephalopathy (PML, 114.11D) is a progressive neurological degenerative syndrome caused by the John Cunningham (JC) virus in immunosuppressed children. Clinical findings of PML include clumsiness, progressive weakness, and visual and speech changes. Personality and cognitive changes may also occur. We require appropriate clinical findings, characteristic white matter lesions on MRI, and a positive PCR test for the JC virus in the cerebrospinal fluid to establish the diagnosis. We also accept a positive brain biopsy for JC virus or other generally acceptable methods consistent with the prevailing state of medical knowledge and clinical practice to establish the diagnosis.
e. Pulmonary Kaposi sarcoma (Kaposi sarcoma in the lung, 114.11E) is the most serious form of Kaposi sarcoma (KS). Other internal KS tumors (for example, tumors of the gastrointestinal tract) have a more variable prognosis. We require characteristic findings on microscopic examination of the induced sputum, bronchoalveolar lavage washings, or of the biopsied transbronchial tissue, or other generally acceptable methods consistent with the prevailing state of medical knowledge and clinical practice to establish the diagnosis.
4. CD4 measurement (114.11F). To evaluate your HIV infection under 114.11F, we require one measurement of your absolute CD4 count (also known as CD4 count or CD4+ T-helper lymphocyte count) or CD4 percentage for children from birth to attainment of age 5, or one measurement of your absolute CD4 count for children from age 5 to attainment of age 18. These measurements (absolute CD4 count or CD4 percentage) must occur within the period we are considering in connection with your application or continuing disability review. If you have more than one CD4 measurement within this period, we will use your lowest absolute CD4 count or your lowest CD4 percentage.
5. Complications of HIV infection requiring hospitalization (114.11G).
a. Complications of HIV infection may include infections (common or opportunistic), cancers, and other conditions. Examples of complications that may result in hospitalization include: Depression; diarrhea; immune reconstitution inflammatory syndrome; malnutrition; and PCP and other severe infections.
b. Under 114.11G, we require three hospitalizations within a 12-month period that are at least 30 days apart and that result from a complication(s) of HIV infection. The hospitalizations may be for the same complication or different complications of HIV infection and are not limited to the examples of complications that may result in hospitalization listed in 114.00F5a. All three hospitalizations must occur within the period we are considering in connection with your application or continuing disability review. Each hospitalization must last at least 48 hours, including hours in a hospital emergency department immediately before the hospitalization.
c. We will use the rules on medical equivalence in § 416.926 of this chapter to evaluate your HIV infection if you have fewer, but longer, hospitalizations, or more frequent, but shorter, hospitalizations, or if you receive nursing, rehabilitation, or other care in alternative settings.
6. Neurological manifestations specific to children (114.11H). The methods of identifying and evaluating neurological manifestations may vary depending on a child's age. For example, in an infant, impaired brain growth can be documented by a decrease in the growth rate of the head. In an older child, impaired brain growth may be documented by brain atrophy on a CT scan or MRI. Neurological manifestations may present in the loss of acquired developmental milestones (developmental regression) in infants and young children or, in the loss of acquired intellectual abilities in school-age children and adolescents. A child may demonstrate loss of intellectual abilities by a decrease in IQ scores, by forgetting information previously learned, by inability to learn new information, or by a sudden onset of a new learning disability. When infants and young children present with serious developmental delays (without regression), we evaluate the child's impairment(s) under 112.00.
7. Growth failure due to HIV immune suppression (114.11I).
a. To evaluate growth failure due to HIV immune suppression, we require documentation of the laboratory values described in 114.11I1 and the growth measurements in 114.11I2 or 114.11I3 within the same consecutive 12-month period. The dates of laboratory findings may be different from the dates of growth measurements.
b. Under 114.11I2 and 114.11I3, we use the appropriate table under 105.08B in the digestive system to determine whether a child's growth is less than the third percentile.
(i) For children from birth to attainment of age 2, we use the weight-for-length table corresponding to the child's gender (Table I or Table II).
(ii) For children from age 2 to attainment of age 18, we use the body mass index (BMI)-for-age corresponding to the child's gender (Table III or Table IV).
(iii) BMI is the ratio of a child's weight to the square of his or her height. We calculate BMI using the formulas in 105.00G2c.
G. How do we consider the effects of treatment in evaluating your autoimmune disorder, immune deficiency disorder, or HIV infection?
1. General. If your impairment does not otherwise meet the requirements of a listing, we will consider your medical treatment in terms of its effectiveness in improving the signs, symptoms, and laboratory abnormalities of your specific immune system disorder or its manifestations, and in terms of any side effects that limit your functioning. We will make every reasonable effort to obtain a specific description of the treatment you receive (including surgery) for your immune system disorder. We consider:
a. The effects of medications you take.
b. Adverse side effects (acute and chronic).
c. The intrusiveness and complexity of your treatment (for example, the dosing schedule, need for injections).
d. The effect of treatment on your mental functioning (for example, cognitive changes, mood disturbance).
e. Variability of your response to treatment (see 114.00G2).
f. The interactive and cumulative effects of your treatments. For example, many children with immune system disorders receive treatment both for their immune system disorders and for the manifestations of the disorders or co-occurring impairments, such as treatment for HIV infection and hepatitis C. The interactive and cumulative effects of these treatments may be greater than the effects of each treatment considered separately.
g. The duration of your treatment.
h. Any other aspects of treatment that may interfere with your ability to function.
2. Variability of your response to treatment. Your response to treatment and the adverse or beneficial consequences of your treatment may vary widely. The effects of your treatment may be temporary or long term. For example, some children may show an initial positive response to a drug or combination of drugs followed by a decrease in effectiveness. When we evaluate your response to treatment and how your treatment may affect you, we consider such factors as disease activity before treatment, requirements for changes in therapeutic regimens, the time required for therapeutic effectiveness of a particular drug or drugs, the limited number of drug combinations that may be available for your impairment(s), and the time-limited efficacy of some drugs. For example, a child with HIV infection or another immune deficiency disorder who develops otitis media may not respond to the same antibiotic regimen used in treating children without HIV infection or another immune deficiency disorder, or may not respond to an antibiotic that he or she responded to before. Therefore, we must consider the effects of your treatment on an individual basis, including the effects of your treatment on your ability to function.
3. How we evaluate the effects of treatment for autoimmune disorders on your ability to function. Some medications may have acute or long-term side effects. When we consider the effects of corticosteroids or other treatments for autoimmune disorders on your ability to function, we consider the factors in 114.00G1 and 114.00G2. Long-term corticosteroid treatment can cause ischemic necrosis of bone, posterior subcapsular cataract, impaired growth, weight gain, glucose intolerance, increased susceptibility to infection, and osteopenia that may result in a loss of function. In addition, medications used in the treatment of autoimmune disorders may also have effects on mental functioning, including cognition (for example, memory), concentration, and mood.
4. How we evaluate the effects of treatment for immune deficiency disorders, excluding HIV infection, on your ability to function. When we consider the effects of your treatment for your immune deficiency disorder on your ability to function, we consider the factors in 114.00G1 and 114.00G2. A frequent need for treatment such as intravenous immunoglobulin and gamma interferon therapy can be intrusive and interfere with your ability to function. We will also consider whether you have chronic side effects from these or other medications, including severe fatigue, fever, headaches, high blood pressure, joint swelling, muscle aches, nausea, shortness of breath, or limitations in mental function including cognition (for example, memory) concentration, and mood.
5. How we evaluate the effects of treatment for HIV infection on your ability to function.
a. General. When we consider the effects of antiretroviral drugs (including the effects of highly active antiretroviral therapy (HAART)) and the effects of treatments for the manifestations of HIV infection on your ability to function, we consider the factors in 114.00G1 and 114.00G2. Side effects of antiretroviral drugs include, but are not limited to: Bone marrow suppression, pancreatitis, gastrointestinal intolerance (nausea, vomiting, diarrhea), neuropathy, rash, hepatotoxicity, lipodystrophy (fat redistribution, such as “buffalo hump”), glucose intolerance, and lactic acidosis. In addition, medications used in the treatment of HIV infection may also have effects on mental functioning, including cognition (for example, memory), concentration, and mood, and may result in malaise, severe fatigue, joint and muscle pain, and insomnia. The symptoms of HIV infection and the side effects of medication may be indistinguishable from each other. We will consider all of your functional limitations, whether they result from your symptoms or signs of HIV infection or the side effects of your treatment.
b. Structured treatment interruptions. A structured treatment interruption (STI, also called a “drug holiday”) is a treatment practice during which your treating source advises you to stop taking your medications temporarily. An STI in itself does not imply that your medical condition has improved; nor does it imply that you are noncompliant with your treatment because you are following your treating source's advice. Therefore, if you have stopped taking medication because your treating source prescribed or recommended an STI, we will not find that you are failing to follow treatment or draw inferences about the severity of your impairment on this fact alone. We will consider why your treating source has prescribed or recommended an STI and all the other information in your case record when we determine the severity of your impairment.
6. When there is no record of ongoing treatment. If you have not received ongoing treatment or have not had an ongoing relationship with the medical community despite the existence of a severe impairment(s), we will evaluate the medical severity and duration of your immune system disorder on the basis of the current objective medical evidence and other evidence in your case record, taking into consideration your medical history, symptoms, clinical and laboratory findings, and medical source opinions. If you have just begun treatment and we cannot determine whether you are disabled based on the evidence we have, we may need to wait to determine the effect of the treatment on your ability to develop and function in an age-appropriate manner. The amount of time we need to wait will depend on the facts of your case. If you have not received treatment, you may not be able to show an impairment that meets the criteria of one of the immune system disorders listings, but your immune system disorder may medically equal a listing or functionally equal the listings.
H. How do we consider your symptoms, including your pain, severe fatigue, and malaise?
Your symptoms, including pain, severe fatigue, and malaise, may be important factors in our determination whether your immune system disorder(s) meets or medically equals a listing or in our determination whether you otherwise have marked and severe functional limitations. In order for us to consider your symptoms, you must have medical signs or laboratory findings showing the existence of a medically determinable impairment(s) that could reasonably be expected to produce the symptoms. If you have such an impairment(s), we will evaluate the intensity, persistence, and functional effects of your symptoms using the rules throughout 114.00 and in our other regulations. See §§ 416.921 and 416.929. Additionally, when we assess the credibility of your complaints about your symptoms and their functional effects, we will not draw any inferences from the fact that you do not receive treatment or that you are not following treatment without considering all of the relevant evidence in your case record, including any explanations you provide that may explain why you are not receiving or following treatment.
I. How do we consider the impact of your immune system disorder on your functioning?
1. We will consider all relevant information in your case record to determine the full impact of your immune system disorder, including HIV infection, on your ability to function. Functional limitation may result from the impact of the disease process itself on your mental functioning, physical functioning, or both your mental and physical functioning. This could result from persistent or intermittent symptoms, such as depression, diarrhea, severe fatigue, or pain, resulting in a limitation of your ability to acquire information, to concentrate, to persevere at a task, to interact with others, to move about, or to cope with stress. You may also have limitations because of your treatment and its side effects (see 114.00G).
2. Important factors we will consider when we evaluate your functioning include, but are not limited to: Your symptoms (see 114.00H), the frequency and duration of manifestations of your immune system disorder, periods of exacerbation and remission, and the functional impact of your treatment, including the side effects of your medication (see 114.00G). See §§ 416.924a and 416.926a of this chapter for additional guidance on the factors we consider when we evaluate your functioning.
3. We will use the rules in §§ 416.924a and 416.926a of this chapter to evaluate your functional limitations and determine whether your impairment functionally equals the listings.
J. How do we evaluate your immune system disorder when it does not meet one of these listings?
1. These listings are only examples of immune system disorders that we consider severe enough to result in marked and severe functional limitations. If your impairment(s) does not meet the criteria of any of these listings, we must also consider whether you have an impairment(s) that satisfies the criteria of a listing in another body system.
2. Children with immune system disorders, including HIV infection, may manifest signs or symptoms of a mental impairment or of another physical impairment. For example, HIV infection may accelerate the onset of conditions such as diabetes or affect the course of or treatment options for diseases such as cardiovascular disease or hepatitis. We may evaluate these impairments under the affected body system. For example, we will evaluate:
a. Growth impairment under 100.00.
b. Musculoskeletal involvement, such as surgical reconstruction of a joint, under 101.00.
c. Ocular involvement, such as dry eye, under 102.00.
d. Respiratory impairments, such as pleuritis, under 103.00.
e. Cardiovascular impairments, such as cardiomyopathy, under 104.00.
f. Digestive impairments, such as hepatitis (including hepatitis C) or weight loss as a result of HIV infection that affects the digestive system, under 105.00.
g. Genitourinary impairments, such as nephropathy, under 106.00.
h. Hematologic abnormalities, such as anemia, granulocytopenia, and thrombocytopenia, under 107.00.
i. Skin impairments, such as persistent fungal and other infectious skin eruptions, and photosensitivity, under 108.00.
j. Neurologic impairments, such as neuropathy or seizures, under 111.00.
k. Mental disorders, such as depression, anxiety, or cognitive deficits, under 112.00.
l. Allergic disorders, such as asthma or atopic dermatitis, under 103.00 or 108.00 or under the criteria in another affected body system.
m. Syphilis or neurosyphilis under the criteria for the affected body system, for example, 102.00 Special senses and speech, 104.00 Cardiovascular system, or 111.00 Neurological.
3. If you have a severe medically determinable impairment(s) that does not meet a listing, we will determine whether your impairment(s) medically equals a listing. (See § 416.926.) If it does not, we will also consider whether you have an impairment(s) that functionally equals the listings. (See § 416.926a.) We use the rules in § 416.994a when we decide whether you continue to be disabled.
114.01 Category of Impairments, Immune System Disorders.
114.02 Systemic lupus erythematosus, as described in 114.00D1. With involvement of two or more organs/body systems, and with:
A. One of the organs/body systems involved to at least a moderate level of severity;
AND
B. At least two of the constitutional symptoms and signs (severe fatigue, fever, malaise, or involuntary weight loss).
114.03 Systemic vasculitis, as described in 114.00D2. With involvement of two or more organs/body systems, and with:
A. One of the organs/body systems involved to at least a moderate level of severity;
AND
B. At least two of the constitutional symptoms and signs (severe fatigue, fever, malaise, or involuntary weight loss).
114.04 Systemic sclerosis (scleroderma). As described in 114.00D3. With:
A. Involvement of two or more organs/body systems, with:
1. One of the organs/body systems involved to at least a moderate level of severity; and
2. At least two of the constitutional symptoms or signs (severe fatigue, fever, malaise, or involuntary weight loss).
or
B. One of the following:
1. Toe contractures or fixed deformity of one or both feet and medical documentation of at least one of the following:
a. A documented medical need (see 114.00C6) for a walker, bilateral canes, or bilateral crutches (see 101.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 101.00C6e(i)); or
b. An inability to use one upper extremity to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 114.00C7), and a documented medical need (see 114.00C6) for a one-handed, hand-held assistive device (see 101.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 101.00C6e(ii)); or
2. Finger contractures or fixed deformity in both hands and medical documentation of an inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 114.00C7); or
3. Atrophy with irreversible damage in one or both lower extremities and medical documentation of at least one of the following:
a. A documented medical need (see 114.00C6) for a walker, bilateral canes, or bilateral crutches (see 101.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 101.00C6e(i)); or
b. An inability to use one upper extremity to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 114.00C7), and a documented medical need (see 114.00C6) for a one-handed, hand-held assistive device (see 101.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 101.00C6e(ii)); or
4. Atrophy with irreversible damage in both upper extremities and medical documentation of an inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 114.00C7); or
C. Raynaud's phenomenon, characterized by:
B. One of the following:
1. Toe contractures or fixed deformity of one or both feet and medical documentation of at least one of the following:
a. A documented medical need (see 114.00C6) for a walker, bilateral canes, or bilateral crutches (see 101.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 101.00C6e(i)); or
b. An inability to use one upper extremity to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 114.00C7), and a documented medical need (see 114.00C6) for a one-handed, hand-held assistive device (see 101.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 101.00C6e(ii)); or
2. Finger contractures or fixed deformity in both hands and medical documentation of an inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 114.00C7); or
3. Atrophy with irreversible damage in one or both lower extremities and medical documentation of at least one of the following:
a. A documented medical need (see 114.00C6) for a walker, bilateral canes, or bilateral crutches (see 101.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 101.00C6e(i)); or
b. An inability to use one upper extremity to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 114.00C7), and a documented medical need (see 114.00C6) for a one-handed, hand-held assistive device (see 101.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 101.00C6e(ii)); or
4. Atrophy with irreversible damage in both upper extremities and medical documentation of an inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 114.00C7); or
C. Raynaud's phenomenon, characterized by:
1. Gangrene involving at least two extremities; or
2. Ischemia with ulcerations of toes or fingers and medical documentation of at least one of the following:
a. A documented medical need (see 114.00C6) for a walker, bilateral canes, or bilateral crutches (see 101.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 101.00C6e(i)); or
b. An inability to use one upper extremity to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 114.00C7), and a documented medical need (see 114.00C6) for a one-handed, hand-held assistive device (see 101.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 101.00C6e(ii)); or
c. An inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 114.00C7).
114.05 Polymyositis and dermatomyositis. As described in 114.00D4. With:
A. Proximal limb-girdle (pelvic or shoulder) muscle weakness and medical documentation of at least one of the following:
1. A documented medical need (see 114.00C6) for a walker, bilateral canes, or bilateral crutches (see 101.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 101.00C6e(i)); or
2. An inability to use one upper extremity to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 114.00C7), and a documented medical need (see 114.00C6) for a one-handed, hand-held assistive device (see 101.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 101.00C6e(ii)); or
3. An inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 114.00C7); or
B. Impaired swallowing (dysphagia) with aspiration due to muscle weakness.
or
C. Impaired respiration due to intercostal and diaphragmatic muscle weakness.
or
D. Diffuse calcinosis with limitation of joint mobility or intestinal motility.
114.06 Undifferentiated and mixed connective tissue disease, as described in 114.00D5. With involvement of two or more organs/body systems, and with:
A. One of the organs/body systems involved to at least a moderate level of severity;
AND
B. At least two of the constitutional symptoms and signs (severe fatigue, fever, malaise, or involuntary weight loss).
114.07 Immune deficiency disorders, excluding HIV infection. As described in 114.00E. With:
A. One or more of the following infections. The infection(s) must either be resistant to treatment or require hospitalization or intravenous treatment three or more times in a 12-month period.
1. Sepsis; or
2. Meningitis; or
3. Pneumonia; or
4. Septic arthritis; or
5. Endocarditis; or
6. Sinusitis documented by appropriate medically acceptable imaging.
or
B. Stem cell transplantation as described under 114.00E3. Consider under a disability until at least 12 months from the date of transplantation. Thereafter, evaluate any residual impairment(s) under the criteria for the affected body system.
114.08 [Reserved]
114.09 Inflammatory arthritis. As described in 114.00D6. With:
A. Persistent inflammation or persistent deformity of:
1. One or more major joints in a lower extremity (see 114.00C8) and medical documentation of at least one of the following:
a. A documented medical need (see 114.00C6) for a walker, bilateral canes, or bilateral crutches (see 101.00C6d) or a wheeled and seated mobility device involving the use of both hands (see 101.00C6e(i)); or
b. An inability to use one upper extremity to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 114.00C7), and a documented medical need (see 114.00C6) for a one-handed, hand-held assistive device (see 101.00C6d) that requires the use of the other upper extremity or a wheeled and seated mobility device involving the use of one hand (see 101.00C6e(ii)); or
2. One or more major joints in each upper extremity (see 114.00C8) and medical documentation of an inability to use both upper extremities to the extent that neither can be used to independently initiate, sustain, and complete age-appropriate activities involving fine and gross movements (see 114.00C7); or
B. Inflammation or deformity in one or more major joints of an upper or lower extremity (see 114.00C8) with:
1. Involvement of two or more organs/body systems with one of the organs/body systems involved to at least a moderate level of severity; and
2. At least two of the constitutional symptoms or signs (severe fatigue, fever, malaise, or involuntary weight loss).
or
C. Ankylosing spondylitis or other spondyloarthropathies, with:
1. Ankylosis (fixation) of the dorsolumbar or cervical spine as shown by appropriate medically acceptable imaging and measured on physical examination at 45° or more of flexion from the vertical position (zero degrees); or
2. Ankylosis (fixation) of the dorsolumbar or cervical spine as shown by appropriate medically acceptable imaging and measured on physical examination at 30° or more of flexion (but less than 45°) measured from the vertical position (zero degrees), and involvement of two or more organs/body systems with one of the organs/body systems involved to at least a moderate level of severity.
114.10 Sjögren's syndrome, as described in 114.00D7. With involvement of two or more organs/body systems, and with:
A. One of the organs/body systems involved to at least a moderate level of severity;
AND
B. At least two of the constitutional symptoms and signs (severe fatigue, fever, malaise, or involuntary weight loss).
114.11 Human immunodeficiency virus (HIV) infection. With documentation as described in 114.00F1 and one of the following:
A. Multicentric (not localized or unicentric) Castleman disease affecting multiple groups of lymph nodes or organs containing lymphoid tissue (see 114.00F3a).
OR
B. Primary central nervous system lymphoma (see 114.00F3b).
OR
C. Primary effusion lymphoma (see 114.00F3c).
OR
D. Progressive multifocal leukoencephalopathy (see 114.00F3d).
OR
E. Pulmonary Kaposi sarcoma (see 114.00F3e).
OR
F. Absolute CD4 count or CD4 percentage (see 114.00F4):
1. For children from birth to attainment of age 1, absolute CD4 count of 500 cells/mm3 or less, or CD4 percentage of less than 15 percent; or
2. For children from age 1 to attainment of age 5, absolute CD4 count of 200 cells/mm3 or less, or CD4 percentage of less than 15 percent; or
3. For children from age 5 to attainment of age 18, absolute CD4 count of 50 cells/mm3 or less.
OR
G. Complication(s) of HIV infection requiring at least three hospitalizations within a 12-month period and at least 30 days apart (see 114.00F5). Each hospitalization must last at least 48 hours, including hours in a hospital emergency department immediately before the hospitalization.
OR
H. A neurological manifestation of HIV infection (for example, HIV encephalopathy or peripheral neuropathy) (see 114.00F6) resulting in one of the following:
1. Loss of previously acquired developmental milestones or intellectual ability (including the sudden onset of a new learning disability), documented on two examinations at least 60 days apart; or
2. Progressive motor dysfunction affecting gait and station or fine and gross motor skills, documented on two examinations at least 60 days apart; or
3. Microcephaly with head circumference that is less than the third percentile for age, documented on two examinations at least 60 days apart; or
4. Brain atrophy, documented by appropriate medically acceptable imaging.
OR
I. Immune suppression and growth failure (see 114.00F7) documented by 1 and 2, or by 1 and 3:
1. CD4 measurement:
a. For children from birth to attainment of age 5, CD4 percentage of less than 20 percent; or
b. For children from age 5 to attainment of age 18, absolute CD4 count of less than 200 cells/mm3 or CD4 percentage of less than 14 percent; and
2. For children from birth to attainment of age 2, three weight-for-length measurements that are:
a. Within a consecutive 12-month period; and
b. At least 60 days apart; and
c. Less than the third percentile on the appropriate weight-for-length table under 105.08B1; or
3. For children from age 2 to attainment of age 18, three BMI-for-age measurements that are:
a. Within a consecutive 12-month period; and
b. At least 60 days apart; and
c. Less than the third percentile on the appropriate BMI-for-age table under 105.08B2.
[50 FR 35066, Aug. 28, 1985]
Appendix 2 to Subpart P of Part 404—Medical-Vocational Guidelines
Sec.
200.00 Introduction.
201.00 Maximum sustained work capability limited to sedentary work as a result of severe medically determinable impairment(s).
202.00 Maximum sustained work capability limited to light work as a result of severe medically determinable impairment(s).
203.00 Maximum sustained work capability limited to medium work as a result of severe medically determinable impairment(s).
204.00 Maximum sustained work capability limited to heavy work (or very heavy work) as a result of severe medically determinable impairment(s).
200.00 Introduction. (a) The following rules reflect the major functional and vocational patterns which are encountered in cases which cannot be evaluated on medical considerations alone, where an individual with a severe medically determinable physical or mental impairment(s) is not engaging in substantial gainful activity and the individual's impairment(s) prevents the performance of his or her vocationally relevant past work. They also reflect the analysis of the various vocational factors (i.e., age, education, and work experience) in combination with the individual's residual functional capacity (used to determine his or her maximum sustained work capability for sedentary, light, medium, heavy, or very heavy work) in evaluating the individual's ability to engage in substantial gainful activity in other than his or her vocationally relevant past work. Where the findings of fact made with respect to a particular individual's vocational factors and residual functional capacity coincide with all of the criteria of a particular rule, the rule directs a conclusion as to whether the individual is or is not disabled. However, each of these findings of fact is subject to rebuttal and the individual may present evidence to refute such findings. Where any one of the findings of fact does not coincide with the corresponding criterion of a rule, the rule does not apply in that particular case and, accordingly, does not direct a conclusion of disabled or not disabled. In any instance where a rule does not apply, full consideration must be given to all of the relevant facts of the case in accordance with the definitions and discussions of each factor in the appropriate sections of the regulations.
(b) The existence of jobs in the national economy is reflected in the “Decisions” shown in the rules; i.e., in promulgating the rules, administrative notice has been taken of the numbers of unskilled jobs that exist throughout the national economy at the various functional levels (sedentary, light, medium, heavy, and very heavy) as supported by the “Dictionary of Occupational Titles” and the “Occupational Outlook Handbook,” published by the Department of Labor; the “County Business Patterns” and “Census Surveys” published by the Bureau of the Census; and occupational surveys of light and sedentary jobs prepared for the Social Security Administration by various State employment agencies. Thus, when all factors coincide with the criteria of a rule, the existence of such jobs is established. However, the existence of such jobs for individuals whose remaining functional capacity or other factors do not coincide with the criteria of a rule must be further considered in terms of what kinds of jobs or types of work may be either additionally indicated or precluded.
(c) In the application of the rules, the individual's residual functional capacity (i.e., the maximum degree to which the individual retains the capacity for sustained performance of the physical-mental requirements of jobs), age, education, and work experience must first be determined. When assessing the person's residual functional capacity, we consider his or her symptoms (such as pain), signs, and laboratory findings together with other evidence we obtain.
(d) The correct disability decision (i.e., on the issue of ability to engage in substantial gainful activity) is found by then locating the individual's specific vocational profile. If an individual's specific profile is not listed within this appendix 2, a conclusion of disabled or not disabled is not directed. Thus, for example, an individual's ability to engage in substantial gainful work where his or her residual functional capacity falls between the ranges of work indicated in the rules (e.g., the individual who can perform more than light but less than medium work), is decided on the basis of the principles and definitions in the regulations, giving consideration to the rules for specific case situations in this appendix 2. These rules represent various combinations of exertional capabilities, age, education and work experience and also provide an overall structure for evaluation of those cases in which the judgments as to each factor do not coincide with those of any specific rule. Thus, when the necessary judgments have been made as to each factor and it is found that no specific rule applies, the rules still provide guidance for decisionmaking, such as in cases involving combinations of impairments. For example, if strength limitations resulting from an individual's impairment(s) considered with the judgments made as to the individual's age, education and work experience correspond to (or closely approximate) the factors of a particular rule, the adjudicator then has a frame of reference for considering the jobs or types of work precluded by other, nonexertional impairments in terms of numbers of jobs remaining for a particular individual.
(e) Since the rules are predicated on an individual's having an impairment which manifests itself by limitations in meeting the strength requirements of jobs, they may not be fully applicable where the nature of an individual's impairment does not result in such limitations, e.g., certain mental, sensory, or skin impairments. In addition, some impairments may result solely in postural and manipulative limitations or environmental restrictions. Environmental restrictions are those restrictions which result in inability to tolerate some physical feature(s) of work settings that occur in certain industries or types of work, e.g., an inability to tolerate dust or fumes.
(1) In the evaluation of disability where the individual has solely a nonexertional type of impairment, determination as to whether disability exists shall be based on the principles in the appropriate sections of the regulations, giving consideration to the rules for specific case situations in this appendix 2. The rules do not direct factual conclusions of disabled or not disabled for individuals with solely nonexertional types of impairments.
(2) However, where an individual has an impairment or combination of impairments resulting in both strength limitations and nonexertional limitations, the rules in this subpart are considered in determining first whether a finding of disabled may be possible based on the strength limitations alone and, if not, the rule(s) reflecting the individual's maximum residual strength capabilities, age, education, and work experience provide a framework for consideration of how much the individual's work capability is further diminished in terms of any types of jobs that would be contraindicated by the nonexertional limitations. Also, in these combinations of nonexertional and exertional limitations which cannot be wholly determined under the rules in this appendix 2, full consideration must be given to all of the relevant facts in the case in accordance with the definitions and discussions of each factor in the appropriate sections of the regulations, which will provide insight into the adjudicative weight to be accorded each factor.
201.00 Maximum sustained work capability limited to sedentary work as a result of severe medically determinable impairment(s). (a) Most sedentary occupations fall within the skilled, semi-skilled, professional, administrative, technical, clerical, and benchwork classifications. Approximately 200 separate unskilled sedentary occupations can be identified, each representing numerous jobs in the national economy. Approximately 85 percent of these jobs are in the machine trades and benchwork occupational categories. These jobs (unskilled sedentary occupations) may be performed after a short demonstration or within 30 days.
(b) These unskilled sedentary occupations are standard within the industries in which they exist. While sedentary work represents a significantly restricted range of work, this range in itself is not so prohibitively restricted as to negate work capability for substantial gainful activity.
(c) Vocational adjustment to sedentary work may be expected where the individual has special skills or experience relevant to sedentary work or where age and basic educational competences provide sufficient occupational mobility to adapt to the major segment of unskilled sedentary work. Inability to engage in substantial gainful activity would be indicated where an individual who is restricted to sedentary work because of a severe medically determinable impairment lacks special skills or experience relevant to sedentary work, lacks educational qualifications relevant to most sedentary work (e.g., has a limited education or less) and the individual's age, though not necessarily advanced, is a factor which significantly limits vocational adaptability.
(d) The adversity of functional restrictions to sedentary work at advanced age (55 and over) for individuals with no relevant past work or who can no longer perform vocationally relevant past work and have no transferable skills, warrants a finding of disabled in the absence of the rare situation where the individual has recently completed education which provides a basis for direct entry into skilled sedentary work. Advanced age and a history of unskilled work or no work experience would ordinarily offset any vocational advantages that might accrue by reason of any remote past education, whether it is more or less than limited education.
(e) The presence of acquired skills that are readily transferable to a significant range of skilled work within an individual's residual functional capacity would ordinarily warrant a finding of ability to engage in substantial gainful activity regardless of the adversity of age, or whether the individual's formal education is commensurate with his or her demonstrated skill level. The acquisition of work skills demonstrates the ability to perform work at the level of complexity demonstrated by the skill level attained regardless of the individual's formal educational attainments.
(f) In order to find transferability of skills to skilled sedentary work for individuals who are of advanced age (55 and over), there must be very little, if any, vocational adjustment required in terms of tools, work processes, work settings, or the industry.
(g) Individuals approaching advanced age (age 50-54) may be significantly limited in vocational adaptability if they are restricted to sedentary work. When such individuals have no past work experience or can no longer perform vocationally relevant past work and have no transferable skills, a finding of disabled ordinarily obtains. However, recently completed education which provides for direct entry into sedentary work will preclude such a finding. For this age group, even a high school education or more (ordinarily completed in the remote past) would have little impact for effecting a vocational adjustment unless relevant work experience reflects use of such education.
(h)
(1) The term younger individual is used to denote an individual age 18 through 49. For individuals who are age 45-49, age is a less advantageous factor for making an adjustment to other work than for those who are age 18-44. Accordingly, a finding of “disabled” is warranted for individuals age 45-49 who:
(i) Are restricted to sedentary work,
(ii) Are unskilled or have no transferable skills,
(iii) Have no past relevant work or can no longer perform past relevant work, and
(iv) Are illiterate.
(2) For individuals who are under age 45, age is a more advantageous factor for making an adjustment to other work. It is usually not a significant factor in limiting such individual's ability to make an adjustment to other work, including an adjustment to unskilled sedentary work, even when the individuals are illiterate.
(3) Nevertheless, a decision of “disabled” may be appropriate for some individuals under age 45 (or individuals age 45-49 for whom rule 201.17 does not direct a decision of disabled) who do not have the ability to perform a full range of sedentary work. However, the inability to perform a full range of sedentary work does not necessarily equate with a finding of “disabled.” Whether an individual will be able to make an adjustment to other work requires an adjudicative assessment of factors such as the type and extent of the individual's limitations or restrictions and the extent of the erosion of the occupational base. It requires an individualized determination that considers the impact of the limitations or restrictions on the number of sedentary, unskilled occupations or the total number of jobs to which the individual may be able to adjust, considering his or her age, education and work experience, including any transferable skills or education providing for direct entry into skilled work.
(4) “Sedentary work” represents a significantly restricted range of work, and individuals with a maximum sustained work capability limited to sedentary work have very serious functional limitations. Therefore, as with any case, a finding that an individual is limited to less than the full range of sedentary work will be based on careful consideration of the evidence of the individual's medical impairment(s) and the limitations and restrictions attributable to it. Such evidence must support the finding that the individual's residual functional capacity is limited to less than the full range of sedentary work.
(i) While illiteracy may significantly limit an individual's vocational scope, the primary work functions in most unskilled occupations involve working with things (rather than with data or people). In these work functions, education has the least significance. Similarly the lack of relevant work experience would have little significance since the bulk of unskilled jobs require no qualifying work experience. Thus, the functional capacity for a full range of sedentary work represents sufficient numbers of jobs to indicate substantial vocational scope for those individuals age 18-44, even if they are illiterate.
Table No. 1—Residual Functional Capacity: Maximum Sustained Work Capability Limited to Sedentary Work as a Result of Severe Medically Determinable Impairment(s)
| Rule | Age | Education | Previous work experience | Decision |
|---|---|---|---|---|
| 201.01 | Advanced age | Limited or less | Unskilled or none | Disabled |
| 201.02 | ......do | ......do | Skilled or semiskilled—skills not transferable1 | Do. |
| 201.03 | ......do | ......do | Skilled or semiskilled—skills transferable1 | Not disabled |
| 201.04 | ......do | High school graduate or more—does not provide for direct entry into skilled work2 | Unskilled or none | Disabled |
| 201.05 | ......do | High school graduate or more—provides for direct entry into skilled work2 | ......do | Not disabled |
| 201.06 | ......do | High school graduate or more—does not provide for direct entry into skilled work2 | Skilled or semiskilled—skills not transferable1 | Disabled |
| 201.07 | ......do | ......do | Skilled or semiskilled—skills transferable1 | Not disabled |
| 201.08 | ......do | High school graduate or more—provides for direct entry into skilled work2 | Skilled or semiskilled—skills not transferable1 | Do. |
| 201.09 | Closely approaching advanced age | Limited or less | Unskilled or none | Disabled |
| 201.10 | ......do | ......do | Skilled or semiskilled—skills not transferable | Do. |
| 201.11 | ......do | ......do | Skilled or semiskilled—skills transferable | Not disabled |
| 201.12 | ......do | High school graduate or more—does not provide for direct entry into skilled work3 | Unskilled or none | Disabled |
| 201.13 | ......do | High school graduate or more—provides for direct entry into skilled work3 | ......do | Not disabled |
| 201.14 | ......do | High school graduate or more—does not provide for direct entry into skilled work3 | Skilled or semiskilled—skills not transferable | Disabled |
| 201.15 | ......do | ......do | Skilled or semiskilled—skills transferable | Not disabled |
| 201.16 | ......do | High school graduate or more—provides for direct entry into skilled work3 | Skilled or semiskilled—skills not transferable | Do. |
| 201.17 | Younger individual age 45-49 | Illiterate | Unskilled or none | Disabled. |
| 201.18 | ......do | Limited or Marginal, but not Illiterate | ......do | Not disabled. |
| 201.19 | ......do | Limited or less | Skilled or semiskilled—skills not transferable | Do. |
| 201.20 | ......do | ......do | Skilled or semiskilled—skills transferable | Do. |
| 201.21 | ......do | High school graduate or more | Skilled or semiskilled—skills not transferable | Do. |
| 201.22 | ......do | ......do | Skilled or semiskilled—skills transferable | Do. |
| 201.23 | Younger individual age 18-44 | Illiterate | Unskilled or none | 4 Do. |
| 201.24 | ......do | Limited or Marginal, but not Illiterate | ......do | 4 Do. |
| 201.25 | ......do | Limited or less | Skilled or semiskilled—skills not transferable | Do.4 |
| 201.26 | ......do | ......do | Skilled or semiskilled—skills transferable | Do.4 |
| 201.27 | ......do | High school graduate or more | Unskilled or none | Do.4 |
| 201.28 | ......do | ......do | Skilled or semiskilled—skills not transferable | Do.4 |
| 201.29 | ......do | ......do | Skilled or semiskilled—skills transferable | Do.4 |
202.00 Maximum sustained work capability limited to light work as a result of severe medically determinable impairment(s). (a) The functional capacity to perform a full range of light work includes the functional capacity to perform sedentary as well as light work. Approximately 1,600 separate sedentary and light unskilled occupations can be identified in eight broad occupational categories, each occupation representing numerous jobs in the national economy. These jobs can be performed after a short demonstration or within 30 days, and do not require special skills or experience.
(b) The functional capacity to perform a wide or full range of light work represents substantial work capability compatible with making a work adjustment to substantial numbers of unskilled jobs and, thus, generally provides sufficient occupational mobility even for severely impaired individuals who are not of advanced age and have sufficient educational competences for unskilled work.
(c) However, for individuals of advanced age who can no longer perform vocationally relevant past work and who have a history of unskilled work experience, or who have only skills that are not readily transferable to a significant range of semi-skilled or skilled work that is within the individual's functional capacity, or who have no work experience, the limitations in vocational adaptability represented by functional restriction to light work warrant a finding of disabled. Ordinarily, even a high school education or more which was completed in the remote past will have little positive impact on effecting a vocational adjustment unless relevant work experience reflects use of such education.
(d) A finding of disabled is warranted where the same factors in paragraph (c) of this section regarding education and previous work experience are present, but where age, though not advanced, is a factor which significantly limits vocational adaptability (i.e., closely approaching advanced age, 50-54) and an individual's vocational scope is further significantly limited by illiteracy.
(e) The presence of acquired skills that are readily transferable to a significant range of semi-skilled or skilled work within an individual's residual functional capacity would ordinarily warrant a finding of not disabled regardless of the adversity of age, or whether the individual's formal education is commensurate with his or her demonstrated skill level. The acquisition of work skills demonstrates the ability to perform work at the level of complexity demonstrated by the skill level attained regardless of the individual's formal educational attainments.
(f) For a finding of transferability of skills to light work for persons of advanced age who are closely approaching retirement age (age 60 or older), there must be very little, if any, vocational adjustment required in terms of tools, work processes, work settings, or the industry.
(g) While illiteracy may significantly limit an individual's vocational scope, the primary work functions in most unskilled occupations relate to working with things (rather than data or people). In these work functions, education has the least significance. Similarly, the lack of relevant work experience would have little significance since the bulk of unskilled jobs require no qualifying work experience. The capability for light work, which includes the ability to do sedentary work, represents the capability for substantial numbers of such jobs. This, in turn, represents substantial vocational scope for younger individuals (age 18-49), even if they are illiterate.
Table No. 2—Residual Functional Capacity: Maximum Sustained Work Capability Limited to Light Work as a Result of Severe Medically Determinable Impairment(s)
| Rule | Age | Education | Previous work experience | Decision |
|---|---|---|---|---|
| 202.01 | Advanced age | Limited or less | Unskilled or none | Disabled. |
| 202.02 | ......do | ......do | Skilled or semiskilled—skills not transferable | Do. |
| 202.03 | ......do | ......do | Skilled or semiskilled—skills transferable1 | Not disabled. |
| 202.04 | ......do | High school graduate or more—does not provide for direct entry into skilled work2 | Unskilled or none | Disabled. |
| 202.05 | ......do | High school graduate or more—provides for direct entry into skilled work2 | ......do | Not disabled. |
| 202.06 | ......do | High school graduate or more—does not provide for direct entry into skilled work2 | Skilled or semiskilled—skills not transferable | Disabled. |
| 202.07 | ......do | ......do | Skilled or semiskilled—skills transferable2 | Not disabled. |
| 202.08 | ......do | High school graduate or more—provides for direct entry into skilled work2 | Skilled or semiskilled—skills not transferable | Do. |
| 202.09 | Closely approaching advanced age | Illiterate | Unskilled or none | Disabled. |
| 202.10 | ......do | Limited or Marginal, but not Illiterate | ......do | Not disabled. |
| 202.11 | ......do | Limited or less | Skilled or semiskilled—skills not transferable | Do. |
| 202.12 | ......do | ......do | Skilled or semiskilled—skills transferable | Do. |
| 202.13 | ......do | High school graduate or more | Unskilled or none | Do. |
| 202.14 | ......do | ......do | Skilled or semiskilled—skills not transferable | Do. |
| 202.15 | ......do | ......do | Skilled or semiskilled—skills transferable | Do. |
| 202.16 | Younger individual | Illiterate | Unskilled or none | Do. |
| 202.17 | ......do | Limited or Marginal, but not Illiterate | ......do | Do. |
| 202.18 | ......do | Limited or less | Skilled or semiskilled—skills not transferable | Do. |
| 202.19 | ......do | ......do | Skilled or semiskilled—skills transferable | Do. |
| 202.20 | ......do | High school graduate or more | Unskilled or none | Do. |
| 202.21 | ......do | ......do | Skilled or semiskilled—skills not transferable | Do. |
| 202.22 | ......do | ......do | Skilled or semiskilled—skills transferable | Do. |
203.00 Maximum sustained work capability limited to medium work as a result of severe medically determinable impairment(s). (a) The functional capacity to perform medium work includes the functional capacity to perform sedentary, light, and medium work. Approximately 2,500 separate sedentary, light, and medium occupations can be identified, each occupation representing numerous jobs in the national economy which do not require skills or previous experience and which can be performed after a short demonstration or within 30 days.
(b) The functional capacity to perform medium work represents such substantial work capability at even the unskilled level that a finding of disabled is ordinarily not warranted in cases where a severely impaired person retains the functional capacity to perform medium work. Even the adversity of advanced age (55 or over) and a work history of unskilled work may be offset by the substantial work capability represented by the functional capacity to perform medium work. However, we will find that a person who (1) has a marginal education, (2) has work experience of 35 years or more doing only arduous unskilled physical labor, (3) is not working, and (4) is no longer able to do this kind of work because of a severe impairment(s) is disabled, even though the person is able to do medium work. (See § 404.1562(a) in this subpart and § 416.962(a) in subpart I of part 416.)
(c) However, the absence of any relevant work experience becomes a more significant adversity for persons of advanced age (55 and over). Accordingly, this factor, in combination with a limited education or less, militates against making a vocational adjustment to even this substantial range of work and a finding of disabled is appropriate. Further, for persons closely approaching retirement age (60 or older) with a work history of unskilled work and with marginal education or less, a finding of disabled is appropriate.
Table No. 3—Residual Functional Capacity: Maximum Sustained Work Capability Limited to Medium Work as a Result of Severe Medically Determinable Impairment(s)
| Rule | Age | Education | Previous work experience | Decision |
|---|---|---|---|---|
| 203.01 | Closely approaching retirement age | Marginal or Illiterate | Unskilled or none | Disabled. |
| 203.02 | ......do | Limited or less | None | Do. |
| 203.03 | ......do | Limited | Unskilled | Not disabled. |
| 203.04 | ......do | Limited or less | Skilled or semiskilled—skills not transferable | Do. |
| 203.05 | ......do | ......do | Skilled or semiskilled—skills transferable | Do. |
| 203.06 | ......do | High school graduate or more | Unskilled or none | Do. |
| 203.07 | ......do | High school graduate or more—does not provide for direct entry into skilled work | Skilled or semiskilled—skills not transferable | Do. |
| 203.08 | ......do | ......do | Skilled or semiskilled—skills transferable | Do. |
| 203.09 | ......do | High school graduate or more—provides for direct entry into skilled work | Skilled or semiskilled—skills not transferable | Do. |
| 203.10 | Advanced age | Limited or less | None | Disabled. |
| 203.11 | ......do | ......do | Unskilled | Not disabled. |
| 203.12 | ......do | ......do | Skilled or semiskilled—skills not transferable | Do. |
| 203.13 | ......do | ......do | Skilled or semiskilled—skills transferable | Do. |
| 203.14 | ......do | High school graduate or more | Unskilled or none | Do. |
| 203.15 | ......do | High school graduate or more—does not provide for direct entry into skilled work | Skilled or semiskilled—skills not transferable | Do. |
| 203.16 | ......do | ......do | Skilled or semiskilled—skills transferable | Do. |
| 203.17 | ......do | High school graduate or more—provides for direct entry into skilled work | Skilled or semiskilled—skills not transferable | Do. |
| 203.18 | Closely approaching advanced age | Limited or less | Unskilled or none | Do. |
| 203.19 | ......do | ......do | Skilled or semiskilled—skills not transferable | Do. |
| 203.20 | ......do | ......do | Skilled or semiskilled—skills transferable | Do. |
| 203.21 | ......do | High school graduate or more | Unskilled or none | Do. |
| 203.22 | ......do | High school graduate or more—does not provide for direct entry into skilled work | Skilled or semiskilled—skills not transferable | Do. |
| 203.23 | ......do | ......do | Skilled or semiskilled—skills transferable | Do. |
| 203.24 | ......do | High school graduate or more—provides for direct entry into skilled work | Skilled or semiskilled—skills not transferable | Do. |
| 203.25 | Younger individual | Limited or less | Unskilled or none | Do. |
| 203.26 | ......do | ......do | Skilled or semiskilled—skills not transferable | Do. |
| 203.27 | ......do | ......do | Skilled or semiskilled—skills transferable | Do. |
| 203.28 | ......do | High school graduate or more | Unskilled or none | Do. |
| 203.29 | ......do | High school graduate or more—does not provide for direct entry into skilled work | Skilled or semiskilled—skills not transferable | Do. |
| 203.30 | ......do | ......do | Skilled or semiskilled—skills transferable | Do. |
| 203.31 | ......do | High school graduate or more—provides for direct entry into skilled work | Skilled or semiskilled—skills not transferable | Do. |
204.00 Maximum sustained work capability limited to heavy work (or very heavy work) as a result of severe medically determinable impairment(s). The residual functional capacity to perform heavy work or very heavy work includes the functional capability for work at the lesser functional levels as well, and represents substantial work capability for jobs in the national economy at all skill and physical demand levels. Individuals who retain the functional capacity to perform heavy work (or very heavy work) ordinarily will not have a severe impairment or will be able to do their past work—either of which would have already provided a basis for a decision of “not disabled”. Environmental restrictions ordinarily would not significantly affect the range of work existing in the national economy for individuals with the physical capability for heavy work (or very heavy work). Thus an impairment which does not preclude heavy work (or very heavy work) would not ordinarily be the primary reason for unemployment, and generally is sufficient for a finding of not disabled, even though age, education, and skill level of prior work experience may be considered adverse.
[45 FR 55584, Aug. 20, 1980, as amended at 56 FR 57944, Nov. 14, 1991; 68 FR 51164, Aug. 26, 2003; 73 FR 64197, Oct. 29, 2008; 85 FR 10602, Feb. 25, 2020]